
Abstract
This article describes 5 all-hazards regional exercises conducted by Public Health Regional Surveillance Teams (PHRSTs) in North Carolina in 2009 and highlights 4 benefits that resulted from the exercises beyond meeting explicit objectives to test plans and identify areas for improvement: building relationships among response partners, promoting public health assets, testing multiple communications systems, and training exercise evaluators.
All-hazards exercises bring together emergency response partners at the local, regional, state, and federal levels for the primary purposes of testing response plans, defining roles and responsibilities, assessing capabilities, and making necessary improvements prior to an actual incident. To better understand the benefits and challenges of conducting regional (ie, multicounty) exercises, a study was carried out by the North Carolina Preparedness and Emergency Response Research Center at the University of North Carolina Gillings School of Global Public Health. This article describes 5 all-hazards regional exercises conducted by Public Health Regional Surveillance Teams (PHRSTs) in North Carolina in 2009 and highlights 4 unique benefits that resulted from the exercises beyond meeting explicit objectives to test plans and identify areas for improvement: (1) building relationships among response partners, (2) promoting public health assets, (3) testing multiple communications systems, and (4) training exercise evaluators. Challenges of planning and conducting regional exercises also are addressed, followed by recommendations for maximizing the effectiveness of regional public health exercises.
All-hazards exercises are an effective way to convene responders at local, regional, state, and federal levels for the purpose of testing response plans, defining roles and responsibilities, and assessing capabilities for a broad spectrum of potential threats. 2 Exercises allow for the identification of strengths and areas for improvement that can be corrected prior to a real incident. 3 It is critical to use the lessons learned from exercises to make improvements in planning and “advance the iterative cycle of preparedness to protect communities in the future.” 4 (p101)
This study examines 5 regional exercises conducted by the North Carolina Public Health Regional Surveillance Teams (PHRSTs) in 2009 that brought together various preparedness partners to respond to all-hazards simulated events. The study outlines the benefits and challenges of implementing regional public health all-hazards exercises. The goal of the study was to help the North Carolina Public Health Office of Preparedness and Response (NC PHP&R) identify system-level recommendations for improving regional exercises. This study was not an evaluation of how well each exercise met its specific goals; it is unique in that it assesses the implementation of public health preparedness exercises by regional entities for multiple jurisdictions (ie, counties), rather than single agency exercises.
Background
In an effort to coordinate and improve their preparedness activities, many states have adopted regional preparedness structures.5,6 Regionalization can increase efficiency by consolidating resources rather than distributing them to numerous local health departments.7,8 Regional structures can promote collaboration among health departments and support sharing of resources.9,10 Strengthening preparedness networks, creating new relationships, and enhancing trust and mutual aid agreements among health departments and various preparedness agencies are all ways in which regionalization builds social capital.7,10 In a case study of several regional public health preparedness programs, Koh et al 9 noted that regionalization can enhance connections among health departments and partner agencies. Additional benefits associated with regionalization include building local and regional capacity and improved training and exercises.7,9,10 For example, in Massachusetts, regionalization was credited with improved communication across jurisdictions and with regions serving as new platforms for conducting training, drills, and exercises. 10
Several studies have examined the use of exercises for assessing and improving public health preparedness. Biddinger et al 4 analyzed 14 after-action reports (AARs) from exercises conducted by the Harvard School of Public Health Center for Public Health Preparedness (HSPH-CPHP) and identified key system challenges. These included “a lack of understanding of individual and agency roles and responsibilities, inconsistent coordination among responders, limited communications capabilities, and limited integration of public health expertise in the response.” 4 (p101) A study by Lurie et al 11 consisted of conducting site visits and smallpox outbreak tabletop exercises in 7 jurisdictions in California to evaluate preparedness. Wide variation was found in levels of preparedness in the areas of leadership capacity and exercise experience, as well as the ability to detect outbreaks and alert physicians and hospitals and the timing to alert the public. 11 The authors concluded that “some sort of regionalization and sharing of resources could increase efficiency.” 11 (pW4–351)
Research in assessing the use of regional platforms in public health exercises is limited. However, in another study by the Harvard School of Public Health Center for Public Health Preparedness, Biddinger et al 12 found that participants in regional exercises reported higher levels of satisfaction in several preparedness areas compared to participants in single institution or agency exercises. The areas of increased satisfaction included increasing participants' understanding of agencies' roles and responsibilities, providing the right environment to practice working together, and promoting region-wide cooperation and mutual aid. 12 The work of the Harvard center through their exercise program demonstrated the usefulness of public health exercises, particularly to help clarify the roles and responsibilities of public health workers and promote the transfer of knowledge among individuals and organizations. 12 System-level challenges can be identified through exercises and, if addressed and corrected, ultimately can lead to improved preparedness and response.
Regionalization in public health preparedness in North Carolina began in December 2001 with the establishment of 7 Public Health Regional Surveillance Teams. According to the PHRST operations manual, the mission of the teams is “to build and support local public health capacity to prevent, prepare for, and respond to public health emergencies in coordination with local, regional, state, and federal resources.” 13 (p6) PHRSTs are located in local health departments around the state and originally were designed to include a physician/epidemiologist, an industrial hygienist, a nurse/epidemiologist, and an administrative support technician. The 7 teams also share 3 pharmacists and have access to veterinary medical response specialists and laboratory services. Through these teams, the NC PHP&R is able to work closely with the state's 85 local health departments and the Health and Medical Division of the Eastern Band of Cherokee Indians to prepare for and respond to public health emergencies.
Each PHRST provides a range of support and services, primarily to a designated regional group of local health departments ranging in number from 7 to 17, with an average of 12 (see Figure 1). 14 The support and services include preparedness planning, exercises, epidemiology and surveillance, consultation and technical assistance, training, and public health event response.
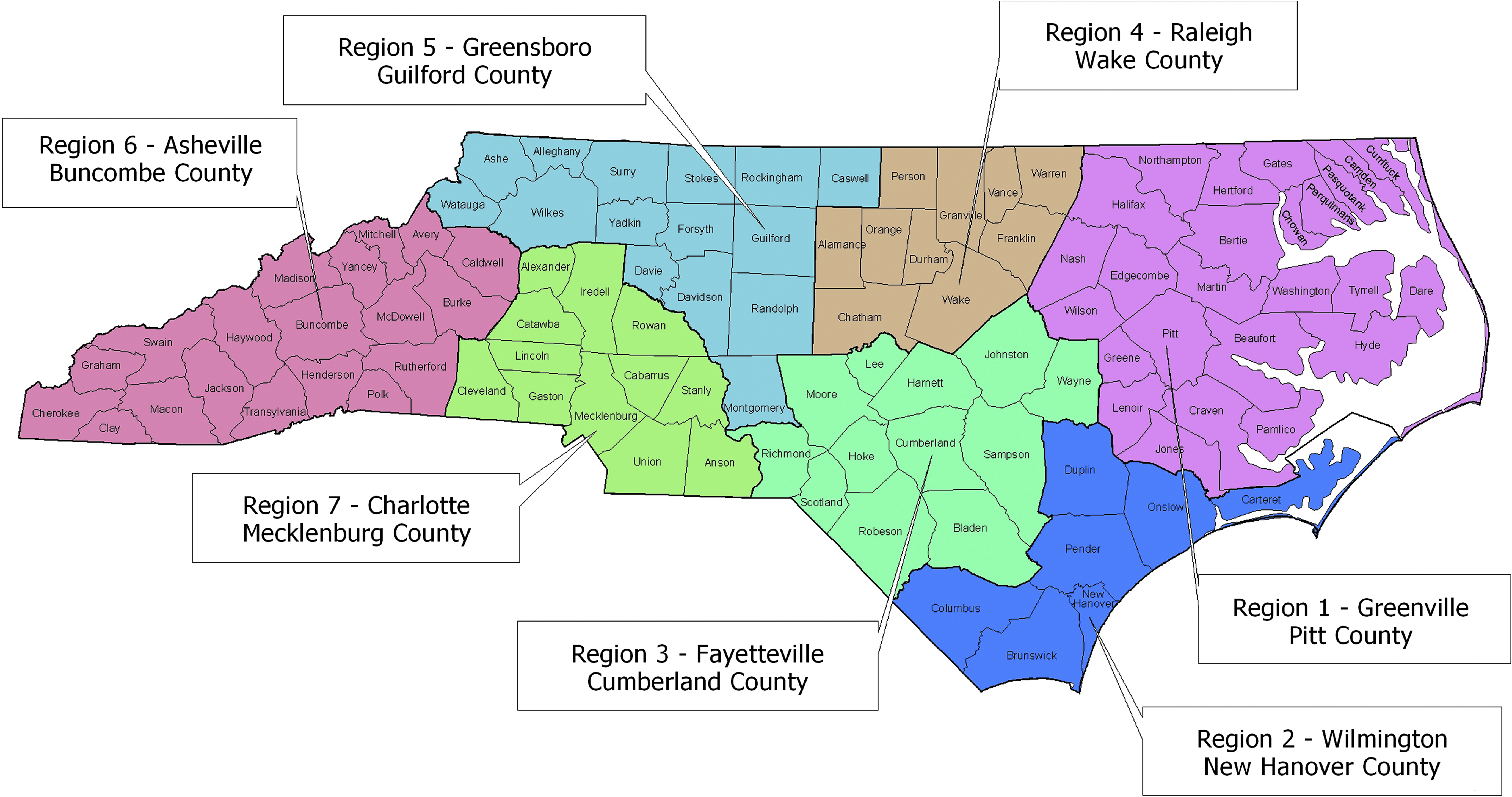
The 7 PHRSTs correspond to the 7 regions of local health departments in North Carolina. Color images available online at www.liebertonline.com/bsp.
In 2009, each PHRST received funding ($20,000/team) to plan and facilitate an all-hazards exercise for its region. This was the first time the teams had been charged by the NC PHP&R with planning and conducting a regional exercise. Prior to 2009, the teams had participated in federal, state, and local exercises. The PHRST members also are trained through the Federal Emergency Management Agency's Homeland Security Exercise and Evaluation Program (HSEEP), which provides tools and training in exercise design, development, implementation, and evaluation. As of October 2009, over 73% of team members had completed both the online and in-person HSEEP training. 14
Methods
Between February and July 2009, the North Carolina Preparedness and Emergency Response Research Center (NCPERRC) at the University of North Carolina Gillings School of Global Public Health observed 5 PHRST exercises. NCPERRC staff aimed to better understand the benefits and challenges of conducting regional exercises. Each exercise was observed by 2 or more research team members using an exercise observation guide. The guide included 7 categories of information: goals/objectives, setting and equipment, exercise execution, systems used, participants, partners, and evaluation. After each exercise, a research team member conducted a semistructured interview with the PHRST exercise leader to obtain information on the leader's experience in planning and conducting the exercise. Each interview was recorded, transcribed, and reviewed for themes related to the lessons learned from the exercises.
In addition, the research team reviewed the PHRSTs' planning and exercise materials, including planning conference notes, exercise evaluation guides, slide presentations, participant handouts, after-action reports, and improvement plans. The research team received supplemental material and information (eg, planning notes, meeting notes) from the NC PHP&R and several PHRSTs. These resources were reviewed for themes related to lessons learned about conducting regional exercises.
Data analysis used case study techniques. A case record was developed for each of the 5 exercises observed and included a detailed description of the exercise, completed observation guides, interview transcripts, and the supplemental materials described above. Case records were reviewed systematically to identify benefits and challenges of individual exercises, as well as common themes across exercises.
Results
Each of the 5 exercises was unique (see Table 1). The scenarios and target capabilities were selected by the PHRST exercise leaders from the Department of Homeland Security master scenario list. The scenarios included an explosion of a radioactive dispersal device (RDD), delivery of CHEMPACK materials, food contamination in a meat processing plant, pandemic influenza, and a mass casualty incident with chemical contamination. Three PHRSTs conducted tabletop exercises, and 1 conducted a functional exercise. Because of the H1N1 outbreak, 1 team modified its exercise from a functional pandemic flu exercise to an after-action review of the H1N1 outbreak response. Depending on the region, the number of exercise participants ranged from 50 to 270, with the number of counties involved ranging from 7 to 19. Two regions cancelled or postponed their exercises as a result of the H1N1 outbreak.
Description of North Carolina Public Health Surveillance Teams' Regional Exercises, 2009
Specifically observed by research team.
Benefits of Regional Public Health Exercises
Four benefits were observed for the counties and regions involved as a direct result of the exercises: (1) building relationships among response partners across counties and agencies and thereby enhancing social capital; (2) promoting the visibility of public health and public health assets in an emergency response; (3) testing multiple communication systems; and (4) training public health practitioners in exercise evaluation.
Partners from various organizations (eg, emergency management, law enforcement, hospitals) were brought together to form teams within their counties in 4 of the exercises. These county teams communicated with other county teams in the region and with the PHRSTs via audio conferencing and WebEOC (an Internet-based information-sharing system). In PHRST region 2, all county participants were brought together in a single facility. This allowed regional-level responders from outside public health (eg, emergency management area coordinator) to interact with individual county personnel and to communicate with all counties in the region simultaneously. As the PHRST region 2 exercise leader noted, the exercise “offered the opportunity to network and meet with other people who had this expertise that they might not have had the opportunity to meet otherwise” and to “understand the capabilities of the rest of the counties.”
The exercises involved extensive planning processes that further served to build relationships between partners. For example, the CHEMPACK functional exercise carried out by PHRST region 3 involved a planning process that was attended by partners from law enforcement, emergency management, hospitals, and others throughout the region. PHRST region 7's mass casualty tabletop exercise was planned in collaboration with another regional entity, the Metrolina Trauma Advisory Committee. PHRST region 4 worked closely with the North Carolina Department of Agriculture during their food contamination exercise and the roll-out of the food emergency response plan.
A second benefit of the observed exercises was that they promoted the visibility of public health (and public health assets) in emergency response. In all of the exercises observed, PHRSTs took a lead role in planning and conducting the exercise. In addition, 1 exercise focused on the promotion of CHEMPACK materials as a public health asset. In PHRST region 3, a DVD of the CHEMPACK program was developed, and a seminar preceding the functional exercise demonstrated these materials.
A third benefit that resulted from the regional exercises observed was that multiple communications systems were tested. PHRST region 3 used the Voice Interoperability Plan for Emergency Responders Radio (VIPER) system to manage its functional CHEMPACK exercise. PHRST region 4 used Foodshield.org web-based videoconferencing as well as WebEOC's chat function to allow participants to query subject matter experts. PHRST region 6 used Polycom (www.polycom.com) and SmileTiger (www.smiletiger.com) video and audio conferencing and WebEOC, while PHRST region 7 used WebEOC, VIPER, and fax.
A fourth benefit of the exercises was that they resulted in a cadre of trained exercise evaluators. As one exercise leader noted, “As we learned in the past [it's important] to get a good evaluator who can really give good comments. And not everyone knows how to do that.” One PHRST was proactive in training local health department staff from nonplaying counties to serve as evaluators for its exercise. As a result of the 5 observed exercises, 32 public health practitioners were trained as evaluators or gained experience evaluating exercises.
Challenges of Regional Exercises
Two major challenges to conducting regional exercises were identified. First, in planning and conducting regional exercises, PHRSTs often were unable to fully play their response roles. Most PHRSTs had either the team leader or the exercise leader facilitate the exercise while other PHRST members served as small group facilitators or evaluators. A significant disadvantage of this was that these PHRST members could not participate as active players in the exercise. As a result, none of the exercises observed provided PHRSTs with the opportunity to fully play their roles as regional responders.
A second challenge of regional exercises is creating scenarios and conducting exercises that involve regional, as opposed to single-county, collaboration among response partners. In all but one of the exercises observed, the counties conducted their exercise play simultaneously but independently. Therefore, there was limited or no county-to-county interaction across the region. While preparedness partners (eg, emergency management, public health) within a county interacted, counties were not required to interact with their neighboring counties or other counties in the region.
Discussion
All of the observed exercises contained elements that had the potential benefit of building interpersonal relationships among response partners within and across counties. In 4 of the observed exercises, partners from various organizations (eg, emergency management, law enforcement, hospitals) were brought together within their county, which allowed for relationship building and networking at the local level. This benefit in building relationships among response partners across counties and agencies and helping clarify specific roles and responsibilities is consistent with findings from a previous study. 4 Biddinger et al noted a similar key lesson related to the “importance of personal relationships and contacts, as well as explicit face-to-face discussion of the assumptions behind agency-specific plans.” 4 (p100)
In all of the exercises observed, PHRSTs took a lead role in planning and conducting the exercise. This had the potential to raise the visibility of public health as a leader in emergency response in the region. This benefit also was documented in studies by Koh et al.9,10 Informing other preparedness partners about public health assets was a benefit of the exercises. According to the director of PHRST region 3, many preparedness officials were unaware of the CHEMPACK program, and as a result they were eager to participate in the exercise. Public health preparedness programs can use exercises as opportunities to promote their assets and leadership capacity with their partners.
The need for extensive communication systems can be attributed to the fact that the exercises were regional (as opposed to local). Testing of communication systems occurred in all observed exercises; in 4 cases, multiple communication systems were used to link the participants with the exercise moderators (PHRSTs) and response partners in different counties. While difficulties with communication systems were observed in all of the 5 exercises, the opportunity to test these systems, train public health practitioners and other response partners on their use, and identify technological challenges resulted in valuable learning in preparation for a real-life emergency.
The training of 32 public health practitioners as exercise evaluators can be partially attributed to the nature of the regional exercises, which tended to be larger than local exercises and often conducted in multiple locations. As such, regional exercises require a large number of evaluators, whose role in recording the actions and decisions of players is critical to the success of regional exercises. The use of these trained and experienced evaluators can enhance the effectiveness of future exercises.
PHRSTs were not charged by the NC PHP&R with planning and conducting a regional exercise that involved cross-county collaboration. However, one of the challenges observed in 4 of the 5 exercises—failure to develop exercise scenarios that test a coordinated regional response to an event—reduced the potential effectiveness of the regional exercises. As one exercise leader commented, “It's important that regional, multicounty exercises are conducted so that coordination can be developed.” Findings from the Harvard exercise program also document the effectiveness of regional exercises for “promoting region-wide cooperation and mutual aid.” 12 (p103)
A study challenge involved the variation in the exercise scenarios, type, and implementation. As a result, it was not always possible to compare the exercise processes and outcomes. Therefore, common themes were reviewed among all exercises, such as communication and coordination with partners. An additional limitation for some regions was that the NCPERRC team was unable to directly observe play in all locations. In these regions, exercises involved multiple counties (7 or more) playing simultaneously from separate locations. However, there were at least 2 observers at key locations for each exercise, and evaluation guides and improvement plans from all counties were reviewed. In an effort to overcome these challenges, the research team worked collaboratively with the NC PHP&R planner/evaluator in developing the research plan and determining the lessons learned from the regional exercises. This collaboration demonstrates the importance of government and academic partnership when conducting applied research.
Regional exercises provide opportunities for collaboration among preparedness partners from different jurisdictions and should be supported. This can be achieved by developing and promoting a statewide calendar of exercises that is used by response partners from various jurisdictions and sectors, including public health, emergency management, law enforcement, and others. To maximize the effectiveness of PHRST-coordinated regional exercises, PHRSTs may also want to consider collaborating with regional counterparts (eg, emergency management regional response teams) in the planning and facilitation of regional exercises to further build these relationships and practice the interagency coordination needed in a real-world emergency.
Future regional exercises should focus on testing regional response plans that promote coordination and communication among multiple local health departments and their county partners. Response partners could benefit from regional exercises that would allow them to respond to events collaboratively across counties rather than within their own county. As a regional entity, PHRSTs are the ideal unit for coordinating and implementing such exercises in North Carolina.
A wide range of communication systems were tested, and the use of these systems was problematic in all of the exercises observed. Recognizing that local health departments and their partners must be able to communicate with each other in a crisis, it would be beneficial for the PHRSTs to work with the NC PHP&R and other key preparedness partners in the state to identify common communication systems that can be used by all local health departments and their partners. Future regional exercises should focus on training staff in using and testing the selected systems.
As regional entities, the PHRSTs can collaborate with each other in planning, facilitating, and evaluating regional exercises, and they can ensure that materials developed by different teams are shared. PHRSTs could organize exercises in pairs or borrow neighboring PHRST staff to assist in facilitation and evaluation so that the “home” PHRST can be a full player in its own regional exercises. Similarly, PHRSTs may want to consider working together to develop strategies to effectively identify and train exercise evaluators, particularly local health department staff, so that a cadre of public health evaluators can be developed and available for regional exercises.
Unique response plans (eg, local RDD plan) and other resources (eg, CHEMPACK informational DVD) were developed in some of the observed exercises. Exercise leaders should ensure that the materials they develop are available to all the PHRSTs by posting them on an appropriate state-based file-sharing site, such as WebEOC. Outside of the North Carolina public health network, PHRSTs can share materials by posting them online through the FEMA Lessons Learned Information Sharing Website.
The 5 PHRST regional all-hazards exercises required significant planning and considerable effort. The identification of critical areas for improvement by PHRSTs, local health departments, and other partners in the after-action reports demonstrate the value of such exercises. In addition, the exercises further contributed to preparedness by enhancing partnerships among responders, promoting public health assets, testing communication systems, and training exercise evaluators.
Footnotes
Acknowledgments
The authors thank the PHRSTs for their collaboration and willingness to work with us on this project. We also thank Anne-Marie Meyer and Jessica Sage for their research assistance. This research was carried out by the North Carolina Preparedness and Emergency Response Research Center (NCPERRC), which is part of the UNC Center for Public Health Preparedness at the University of North Carolina at Chapel Hill's Gillings School of Global Public Health, and was supported by the Centers for Disease Control and Prevention (CDC) Grant 1PO2 TP 000296. The contents are solely the responsibility of the authors and do not necessarily represent the official views of CDC. Additional information can be found at ![]() .
.