
Abstract
Introduction:
Obesity is defined as an excess of accumulation of fat that can be harmful to health. Storage of excess fat in the adipose tissue triggers an inflammatory process, which makes obesity a low-grade chronic inflammatory disease. Obesity is considered a complex and multifactorial disease; hence, no intervention strategy appears to be an ideal treatment for all individuals. Therefore, new therapeutic alternatives are often studied for the treatment of this disease. Currently, herbal medicines are gaining ground in the treatment of obesity and its comorbidities. In this context, much attention is being paid to Cannabis sativa derivatives, and their therapeutic functions are being widely studied, including in treating obesity.
Objective:
Highlight the pharmacological properties of Δ9-tetrahydrocannabivarin (THCV), Δ9-tetrahydrocannabidinol (THC), and cannabidiol (CBD), the predominant isolated components of Cannabis sativa, as well as its therapeutic potential in the treatment of obesity.
Methods:
This is a narrative review that shows the existing scientific evidence on the clinical application of Cannabis sativa as a possible treatment for obesity. Data collection was performed in the PubMed electronic database. The following word combinations were used: Cannabis and obesity, Cannabis sativa and obesity, THCV and obesity, THC and obesity, CBD and obesity, and Cannabis sativa and inflammation.
Results:
Evidence shows that Cannabis sativa derivatives have therapeutic potential due to their anti-inflammatory properties. In addition, people who use cannabis have a lower body mass index than those who do not, making the plant an option to reduce and reverse inflammation and comorbidities in obesity.
Conclusion:
It is concluded that phytocannabinoids derived from Cannabis sativa have therapeutic potential due to its anti-inflammatory, antioxidant, and neuroprotective properties, making the plant a study option to reduce and reverse inflammation and comorbidities associated with obesity.
Introduction
Obesity has become one of the greatest public health challenges, warranting a state of alert, as the prevalence of this disease in all age groups continues to increase.1,2 Updated global data from the World Health Organization (WHO) reveal a rapid increase in the prevalence of obesity. 3 These data are very worrying, considering the global economic impact of this disease. In addition to excessive expenditure on health care, obesity also imposes costs in the form of lost productivity at work, mortality, and permanent disability. 4
According to the WHO, obesity is an excess of accumulation of fat that can be harmful to health. 3 This accumulation occurs due to an imbalance between high caloric consumption and low energy expenditure. 5 Excess fat stored in adipose tissue triggers an initially local and subsequently systemic inflammatory process, which makes obesity a low-grade chronic inflammatory disease. 6
Seen as an inflammatory disease and a trigger for other comorbidities, obesity exhibits the need for specific treatment. The first line of treatment for this disease is a change in lifestyle, which consists of reducing caloric consumption plus increasing physical exercise. Pharmacological therapy plays a minor role, and in addition to having a less lasting effect, it has shown therapies developed to date have shown numerous side effects, even leading to the withdrawal of drugs from the market as they present an unfavorable risk-benefit ratio.7–9
In addition, the development of obesity depends on a diversity of genetic, biological, psychological, sociocultural, and environmental factors. 10 In view of these facts, no intervention strategy appears as an ideal treatment for all individuals. Great variability in response to treatment for weight loss is a common theme among intervention studies for this purpose, demonstrating that different treatments may be effective for some individuals, but result in little or no benefit in others. 11
Therefore, new therapeutic alternatives are often studied for the treatment of obesity. Currently, much attention is being paid to Cannabis sativa derivatives that interact with constituents of the endocannabinoid system (ECS), such as Δ9-Tetrahydrocannabivarin (THCV), THC, and CBD, due to their anti-inflammatory properties, antioxidants, anorectic and thermogenesis, which propose its use in the treatment of obesity.12,13
Therefore, the objective of this narrative review was to summarize the existing scientific evidence on the clinical application of Cannabis sativa as a possible treatment for obesity. This review was carried out in the electronic database PubMed, collecting articles related to the topic. The following word combinations were used: cannabis and obesity, Cannabis sativa and obesity, THCV and obesity, Δ9-tetrahydrocannabidinol and obesity, CBD and obesity, e Cannabis sativa and inflammation.
The Extent of the Obesity Epidemic Problem
Lifestyle and diet in most modern and developing societies has undergone significant changes in the past decades. Sedentary lifestyle, as well as the excessive consumption of calorie-dense foods, has established an “obesogenic” environment and contributed to a serious obesity epidemic. 14 Thus, obesity is defined as the excessive accumulation of fat that results mainly from the imbalance between high caloric intake and low energy expenditure that compromises the health of individuals. 15
Obesity not only increases the risk of cardiovascular disease and certain types of cancer, but is also characterized as a key factor in the development of other components of metabolic syndromes. These components include insulin resistance, hyperglycemia with prediabetes or type 2 diabetes mellitus (DM), dyslipidemia, and hypertension, points that constitute a systemic metabolic dysfunction.16–18 In view of this, obesity has become a rapidly growing public health problem and affects several countries around the world, due to its prevalence, costs, and damage to health. 19
Obesity has had its incidence numbers tripled since 1975, in 2016 reaching >1.9 billion adults >18 years being overweight (39%), and 650 million (13%) with some degree of obesity. Furthermore, WHO data reveal that 340 million children and adolescents between 5 and 19 years were overweight or obese. In 2019, 38 million children <5 years were diagnosed as overweight or obese. 3 With this, and being recognized as a pathology that has affected the population at increasingly early ages, obesity has been gaining prominence in the worldwide epidemiological scenario, reaching the WHO classification of an epidemic. 20 However, an increase in adiposity is a chronic and potentially reversible process, with adequate diagnosis and treatment. 21
The main means of assessment for obesity adopted by the WHO is the body mass index (BMI), which consists of the division of weight in kilograms by the square of height in meters (kg/m2). This method is used for the diagnosis of overweight and obese individuals, in addition to associating them with the risk of developing other comorbidities. 15 However, in general, BMI is not sufficient for the assessment of nutritional status, and should be associated with other measures, such as skinfolds and segment circumferences, bioimpedance, magnetic resonance, computed tomography, and dual energy X-ray densitometry.22–24 The early diagnosis of obesity is essential due to factors related to pathophysiology, as well as to avoid worsening of the disease and an increase in comorbidities associated with obesity. 25
The Pathophysiological Mechanism of Obesity and Its Relationship with the Inflammatory Response
Obesity is an inflammatory disease influenced by several genetic and environmental factors. However, its main cause is the imbalance between high caloric consumption through food and low energy expenditure, providing a positive balance of energy. This excess energy is stored in the form of triglycerides in the cells of the white adipose tissue (WAT) called adipocytes. 26 WAT is an important endocrine and regulatory organ,27,28 its impairment reflects the homeostatic imbalance of substances important for energy storage and metabolism, such as leptin, insulin, and ghrelin.29,30
Leptin is an anorexigenic substance, produced by WAT, and acts on its receptors present in the arcuate nucleus of the hypothalamus. This substance is able to suppress neurons that produce neuropeptide Y (NPY) and agouti-related protein peptide, which exert an orexigenic effect (stimulate appetite), increase the activity of pro-opiomelanocortin and cocaine and amphetamine-regulated transcript, which are anorexigenic (inhibit appetite), regulating food when stored energy levels are sufficient. Its production is proportional to the increase in adipose mass; therefore, in obesity, its serum levels are high,31–33 and a resistance of its receptors is also observed at the hypothalamic level, causing an important imbalance in its interpretation in relation to satiety and energy stocks. 34
Obesity also influences the development of peripheral insulin resistance. Insulin is a hormone secreted by β-pancreatic cells that binds to specific receptors that provide the entry of serum glucose into cells, serving as a substrate for cellular respiration and formation of adenosine triphosphate. Resistance to this hormone leads to an accumulation of glucose in the bloodstream, contributing to the development of metabolic diseases, especially type 2 DM. 35
Concomitant with leptin and insulin, ghrelin has its activity compromised in obesity, since its secretion is increased. It is naturally secreted by stomach cells and acts on the arcuate nucleus of the hypothalamus to signal the need for nutrients, especially in the premeal and prolonged fasting states. It works by activating orexigenic neurons, mainly NPY producers, inducing hunger, with the opposite effect to leptin. When increased, ghrelin can be an important factor in the imbalance of the reward system.36,37
In addition, the high fat content stimulates adipocyte hypertrophy, a situation in which the adipocytes increase in size, thus, the lipid storage capacity can be expanded giving rise to additional adipocytes (adipogenesis) in a process called “hyperplasia.”38,39
The adipose expansion derived from obesity can lead to a narrowing of the extracellular space, compressing the blood vessels in the region, impairing blood supply and oxygen distribution, which favors the state of hypoxia.40,41 The condition of low oxygenation in the adipose tissue induces the infiltration of macrophages that act by eliminating necrotic adipocytes, which subsequently amplify a local inflammatory response, producing interleukin (IL)-6 and tumor necrosis factor (TNF)-α42,43 and reducing the production of adiponectin, promoting inflammation and oxidative stress in adipose tissue. 44 The high concentration of proinflammatory factors secreted at the site reaches the bloodstream, causing systemic chronic inflammation characterized by low intensity. 45
It is known that the macrophages residing in the adipose tissue of eutrophic individuals belong to the alternatively activated type M2, which are fundamental in the adipose tissue homeostasis. In contrast, the number of classically activated M1 macrophages increases in the adipose tissue of obese individuals, favoring the processes of inflammation and insulin resistance (IR).46,47
Elevated levels of proinflammatory cytokines, free fatty acids, and immune cells present in the bloodstream in obese individuals can generate brain inflammation. These substances in question can access the central nervous system (CNS) through fissures present in the blood–brain barrier and activate Toll-like receptors, thus stimulating an even greater production of proinflammatory factors in the hypothalamus, inducing neuroinflammation, microglial proliferation, and affecting other brain structures. 48
In addition, the impairment of energy metabolism, resulting from hormonal dysregulation, associated with inflammation installed in obesity, promotes an increase in glucose and serum lipids. This increase can generate an excessive supply of energetic substrates to the metabolic pathways in the cells, which may increase the production of reactive oxygen species (ROS), and reflect on the damage of proteins, lipids, and DNA of tissues. 49 Among the affected tissues, brain structures are severely impaired, due to the high amount of lipid in its composition, in addition to the use of glucose for its metabolism. 50 Considering that obesity and its comorbidities are not only peripheral disorders, but also imply neurological changes, effective therapies are certainly needed to minimize such damage.
Treatment for Obesity: From Lifestyle Changes to a Pharmacotherapeutic Approach
The first line of treatment and prevention of obesity consists of changing lifestyle to include frequent physical exercise and the adoption of a healthy diet with adequate distribution of macronutrients, as well as the regular consumption of fruits, vegetables, and micronutrients. These are considered as good strategies to reduce the prevalence of obesity and associated comorbidities. 51 In this way, it is possible to rebalance the consumption and expenditure of calories, culminating in the burning of stored fat and weight loss.9,52
However, treatment should not focus only on weight loss, but also on the prevention and reversal of associated metabolic comorbidities; therefore, pharmacological therapies are often used when caloric restriction and physical exercise are not sufficient in the weight loss process. 53 The use of pharmacotherapy for weight control is consistent with the treatment of obesity as a chronic disease that requires a multifaceted approach, including dietary modification, behavioral intervention, and appropriate medical intervention. Current guidelines suggest that individuals who do not respond to lifestyle interventions after 6 months of treatment and who have a BMI >30 kg/m2, or a BMI >27 kg/m2 with a comorbidity associated with obesity can be considered in drug treatment for weight loss. 54
Some drugs approved by the Food and Drug Administration (FDA) are used in the treatment of obesity only for a short period, due to the associated risks, whereas some others are approved for use in the long term. 53 Although some pharmacological therapies assist in the control of obesity, the majority of commonly used drugs are associated with adverse health effects 51 that include cardiovascular complications, possibly due to the formation of thrombi, insomnia, constipation, dry mouth, dizziness, dysgeusia, headache, fatigue, gastrointestinal symptoms, among others. As a result, many drugs have been withdrawn from the market due to unwanted side effects.9,53,55
Bariatric surgery is increasingly being performed in the medically complicated obese population, not only to achieve significant weight loss, but also to correct obesity-related diseases. 56 The criteria for considering bariatric surgery include the presence of obesity (BMI >30), history of multiple attempts to reduce weight by O'Brien 57 nonsurgical means, awareness of potential risks, and commitment to participate in the follow-up program. It is worth emphasizing that bariatric procedures can be associated with complications that include leaks, strictures, bleeding, and venous thromboembolic events. 58
In view of this, herbal medicines are gaining ground in the treatment of obesity and its comorbidities. Several plants and their derivatives have brought positive results, mainly in weight reduction, waist circumference, and suppression of inflammatory pathways.59–68 In this context, drugs derived from the Cannabis sativa plant, called phytocannabinoids, have been studied as a treatment option for several pathologies. This plant and its derivatives bring important results in the literature associated with anti-inflammatory, antioxidant, and anticonvulsant effects, among others,12,69–73 and can be an alternative for the metabolic re-establishment in obesity, given the complexity and incidence of adverse events related to the currently available therapeutic options.
Cannabis sativa, ECS, and Its Anti-Inflammatory Potential as Indirect Support in the Treatment of Obesity
The cannabis genus includes three species, Cannabis sativa, Cannabis indica, and Cannabis ruderalis. 74 Cannabis sativa, popularly known as marijuana,74,75 has been widely studied for its varied therapeutic potential,71,72 since it produces substances capable of interacting with receptors of a homeostasis system called the ECS. 78 This system was discovered in 1988, during in-depth studies of the effects of Cannabis sativa. 79
The ECS consists of two members of the family of receptors coupled to protein G, cannabinoid receptor 1 (CB1) and cannabinoid receptor 2 (CB2), as well as endogenous ligands, among these, the most studied are anandamide and 2-arachidonoylglycerol (2-AG).80,81 This signaling system occurs within the CNS and in various peripheral organs. 82 CB1 is present mainly in the CNS, modulating mood, appetite, memory, and pain.78,83 It is also expressed in several peripheral tissues, such as adipose tissue, liver, skeletal muscle, gastrointestinal tract, and pancreas.84,85 He is involved in studies evaluating the effects of Cannabis sativa on neuropsychiatric and neurodegenerative diseases. 80
In addition, CB1 is a primary mediator for energy capture, storage, and conservation. It works by enhancing the absorption and conservation of energy through various mechanisms. Stimulation of CB1 modulates the taste and smell pathways to increase the palatability of food. It also stimulates the brain's appetite centers, promoting hyperphagia and contributing to the accumulation of fat in adipose tissue.86–94 CB2 acts on the peripheral nervous system, is expressed in the spleen and tonsils, as well as in B cells, monocytes and T cells, and is associated with the balance of the immune system.78,83,95,96 Therefore, the interaction with CB2 is the cause of the anti-inflammatory and immunomodulatory effects of Cannabis sativa. 97
In addition to endogenous substances, phytocannabinoids, which are substances produced in plant trichomes in the genus Cannabis sativa, are also capable of interacting with ECS receptors.83,98 Cannabis sativa produces >400 compounds, 66 of which are classified as phytocannabinoids. 99 Among the phytocannabinoids present in Cannabis sativa, the ones that are most relevant to the studies are THCV, THC, and CBD.13,100
THCV primarily works by antagonizing the CB1 receptor; this compound can, therefore, have anorectic effects, inhibiting appetite, controlling food, and consequently decreasing body weight. 101 However, at high dosages, THCV can demonstrate CB1 agonism and partial CB2 agonism. 102 Therefore, even though it is a THC analogue, THCV behaves differently in relation to receptors, which may potentiate (in high doses), or antagonize the psychoactive or nonpsychoactive effects of THC (Fig. 1). 101
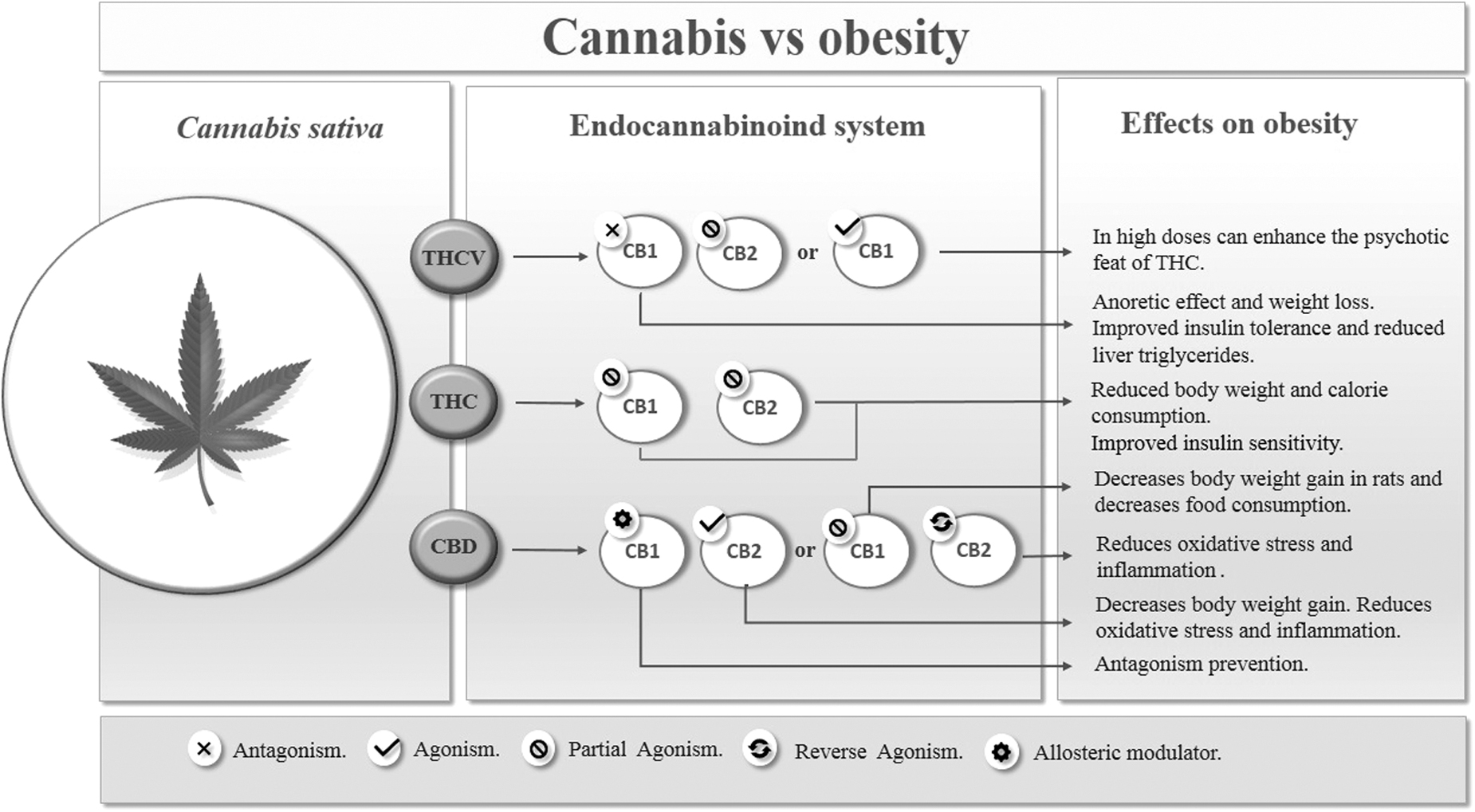
Cannabis versus obesity. THCV, Δ9-tetrahydrocannabivarin.
THC is the most abundant phytocannabinoid in the Cannabis sativa plant, being the main psychoactive constituent of the plant. It is a highly fat-soluble compound, a partial agonist of both CB1 and CB2 receptors, with greater affinity for CB1. 98 Therefore, this compound is responsible for the known psychoactive effects of Cannabis sativa, such as euphoria, sedation, and hallucination.83,102 This agonist effect on CB1 explains the use of this substance for pain relief in several clinical conditions, 103 such as neuropathic pain, 104 for nausea and vomiting associated with chemotherapy, 103 and for the treatment of psychiatric diseases such as anxiety and depression. 105 However, this compound used alone can cause several side effects (Fig. 1). 97
CBD, in contrast, acts as a weak antagonist (inhibits the effects) of CB1 and CB2 receptors, and an important inverse agonist (decreases the effect, but does not inhibit) of CB2 receptors.97,98 The anti-inflammatory potential of CBD can primarily be explained by the effect on CB2, since by softening the effect of receptors on immune cells, it automatically softens the activity of these cells (Fig. 1). 97
In addition to CB receptors, it has been suggested that CBD is also associated with other pharmacological substrates. In this context, CBD also showed an affinity for peroxisome proliferation-activated receptors (PPARs), which are a family of transcription factors inducible by ligands belonging to the nuclear hormone receptor superfamily. In humans, there are three PPAR PPARα, PPARβ/δ, and PPARγ isoforms that are encoded by distinct genes and are expressed in different ways in organs and tissues.106,107 CBD appears to activate the transcriptional activity of PPARγ, which plays an essential role in controlling adipocyte formation, insulin sensitivity, and activation of the inflammatory response. Thus, CBD activates PPARγ receptors causing less expression of proinflammatory genes (Fig. 2).108–110
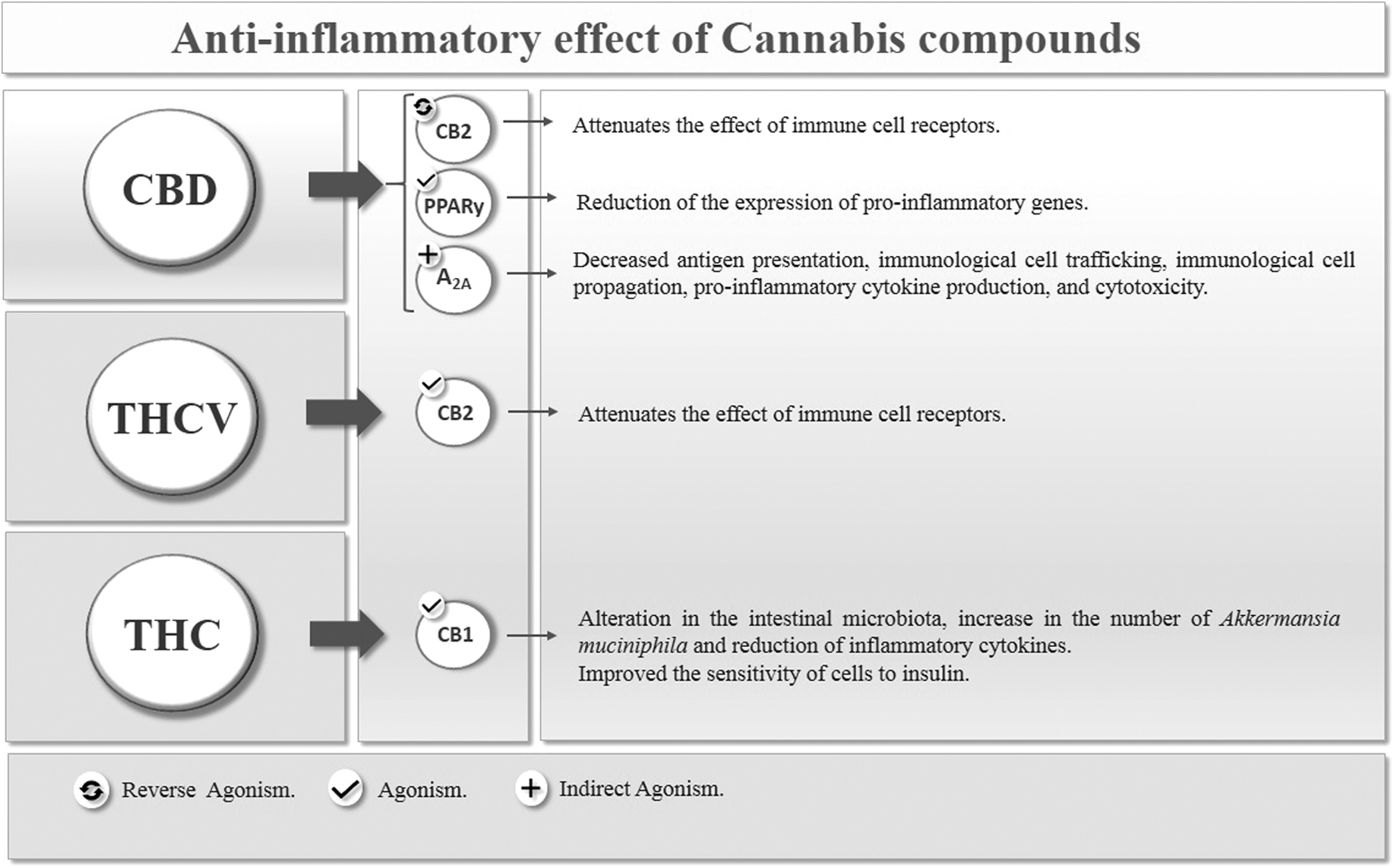
Anti-inflammatory effect of cannabis compounds.
The anti-inflammatory effect of CBD is also mediated by the adenosine A 2A (A 2A) receptor, whose activation attenuates the immune system, causing a decrease in antigen presentation, immune cell trafficking, immune cell propagation, proinflammatory cytokine production, and cytotoxicity. 111 CBD has been shown to intensify A 2A receptor signaling by inhibiting cell renewal of an adenosine transporter, generating anti-inflammatory and antioxidant effects (Fig. 2). 112
Along with the effects on the immune system, CBD demonstrates poorly understood antioxidant effects, which may have neuroprotective potential 113 and can modulate serotonin receptors. 102 Therefore, CBD can have a therapeutic function in several conditions involving inflammation and oxidative stress, such as Parkinson's disease,114,115 rheumatoid arthritis, 116 Alzheimer's disease, 117 ischemia-reperfusion injury, 118 metabolic diseases,119,120 among others. In addition, CBD demonstrates opposite effects to THC on CB1 receptors, which allows control of adverse effects when used in combination.98,121
Considering the properties mentioned (anti-inflammatory, antioxidant, and antiobesity), CBD appears to be a potential therapeutic agent that could be used in the treatment of obesity, type 2 DM and its complications, ischemia, and neurodegenerative diseases, in addition to pain relief and depression. Although the anti-inflammatory and neuroprotective properties of CBD are well determined, there are few studies that have investigated the antiobesity effects of this compound.12,87,122–128
Based on the data presented, the hypothesis arises that Cannabis sativa and its derivatives can be potentially effective in treating and reversing the damage caused by inflammation in obesity.
Cannabinoids as a promising metabolic re-establishment target in obesity
The therapeutic benefits of Cannabis sativa plant extracts and their subspecies have been widely studied. THCV, THC, and CBD are the predominant isolated components of Cannabis sativa and have been extensively studied in the modern literature.76,129
Some components of Cannabis sativa are known to stimulate appetite, whereas others are promising for the treatment of obesity. In view of this, there was an interest in investigating the role of the ECS in the control of obesity and in the associated metabolic syndrome130,131 (Table 1). This interest subsequently led to the development of an effective therapeutic strategy for obesity, which consisted of blocking CB1 cannabinoid receptors using ligands such as Rimonabant. 130 A synthetic CB1 receptor antagonist that performs its function in the ECS selectively blocking CB1 receptors, thereby decreasing appetite, leading to hypophagia and improving the metabolic profile.132–134
Use of Cannabinoids in Obesity
AM251, CB1 receptor antagonist drug; AM630, selective CB2 agonist drug; APO A, apolipoprotein A; BDS, botanical drug substance; CB1, cannabinoid receptor 1; CB2, cannabinoid receptor 2; CBC, cannabichromene; CBDA, cannabidiolic acid; CBDV, cannabidivarin; CBDVA, cannabidivarinic acid; CBG, cannabigerol; CBGA, cannabigerolic acid; CBGV, cannabigerivarin; CBN, cannabinol; DIO, diet-induced obesity; DPCPX, cyclopentyl-1,3-dipropylxanthine; HDL, high-density lipoprotein; IL, interleukin; I.P., intraperitoneally; IRS-1, insulin receptor substrate 1; IRS-2, insulin receptor substrate 2; PPAR, peroxisome proliferation-activated receptor; Rimonabant, CB1 receptor antagonist drug; THCA, tetrahydrocannabinolic acid; THCV, Δ9-tetrahydrocannabivarin; TNF, tumor necrosis factor.
In addition, it has been suggested that the clinical effects of rimonabant may be associated with antagonism of CB1 receptors not only in the brain, but also in the liver and adipose tissue, leading to reduced lipid storage and increased glucose sensitivity. 95
Animal and human studies have shown that CB1 receptor antagonism has increased O2 consumption and energy expenditure at rest. In comparison with the animals in the control group, rats treated with 3 and 10 mg/kg of rimonabant had an increase in O2 consumption of 18% and 49%, respectively, after 3 h. 135 In humans, blocking CB1 with rimonabant 20 mg, combined with a low-calorie diet for 1 year, promoted a significant decrease in body weight and waist circumference, and improved cardiovascular risk factors. 132 Although effective, Rimonabant has been linked to increased rates of depression, anxiety, and even suicide; it has, therefore, been withdrawn from the market.133,134,136
However, ongoing studies suggest that restricted peripheral CB1 antagonists, such as URB447 and AM6545, may provide therapeutic benefits in obesity without these psychiatric side effects.137–139
THCV is an inverse agonist of the CB1 receptor, similar to Rimonabant; however, it does not present the adverse effects of this medication.77,140,141 THCV is a natural analogue of THC. Although THCV has a structure similar to THC (differentiated only by the length of its lipophilic alkyl chain), it has several molecular targets and pharmacological profiles. Compared with THC, which expresses its effects through the weak partial agonist activity of CB1 and CB2 endocannabinoid receptors, THCV acts as a neutral CB1 antagonist and partial CB2 agonist. 142
Neutral antagonists have been suggested as a potentially safer alternative to Rimonabant in the treatment of obesity. It is suggested that THCV avoids the psychological effects of THC, which include anxiety, depression, cognitive impairment, and the potential for abuse and dependence. However, the mechanism by which THCV antagonizes the effect of THC is unknown.13,140
Animal studies have shown that neutral antagonists appear to decrease food consumption and weight gain similar to Rimonabant, but unlike this drug they do not inhibit activity in areas of emotion regulation, such as the ventral tegmental area and the basolateral amygdala. 140 However, the mechanism by which THCV interacts with the reward and aversion systems in the human brain is still unknown. 141
In this way, Tudge et al. 141 examined the effects of THCV using a reward and aversion processing model in the human brain. Since THCV is thought to be free of the depressogenic side effects seen with Rimonabant, it would consequently not alter the responses in areas that have been shown to be involved in reward processing. Twenty healthy volunteers received a single dose of THCV (10 mg) and placebo in random order on two separate occasions. The neural responses to gratifying stimuli (vision and/or chocolate flavor) and aversive stimuli (image of moldy strawberries and/or less pleasant strawberry flavor) were measured using functional magnetic resonance images. The volunteers assessed pleasure, intensity, and desire for each stimulus.
In conclusion, the findings showed that treatment with THCV increased responses to chocolate stimuli in the midbrain, anterior cingulate cortex, caudate, and putamen. In addition, it increased responses to aversive stimuli in the amygdala, insula, middle orbitofrontal cortex, caudate, and putamen, that is, it did not reduce the processing of rewards, but improved activations in the main areas of rewards and aversion processing. This may indicate that THCV does not compromise motivational processes, probably because does not cause depressive symptom, since it does not mitigate the activation of stimuli with positive or negative values in key areas of brain motivation. This effect profile suggests therapeutic activity in obesity, perhaps with a lower risk of depressive side effects. 141
Wargent et al. 143 evaluated the effect of THCV on metabolic disorders that accompany obesity, such as hyperglycemia, dyslipidemia, and fatty liver using diet-induced obese (DIO) and genetically obese (ob/ob) mice. Thus, they performed two studies of dose variation in DIO mice; study 1: 0.3, 1, 2.5, 5 and 12.5 mg/kg, orally twice a day for 30 days and study 2: 0.1, 0.5, 2.5 and 12.5 mg/kg, orally once a day for 45 days. A pilot study (study 3: 0.3 and 3 mg/kg, orally once daily) and a complete varied dose study (study 4: 0.1, 0.5, 2.5 and 12.5 mg/kg, oral once daily) in ob/ob for 30 days. The results were compared with a potent CB1 inverse agonist (AM251) administered orally at 10 mg/kg once daily or 5 mg/kg twice daily as a positive control.
According to the results, THCV did not significantly affect food intake or body weight gain, but it did produce an early and transient increase in energy expenditure. Depending on the dose, glucose intolerance decreased in ob/ob mice, improved glucose tolerance, and increased insulin sensitivity in DIO mice; in addition, the higher doses of THCV (2.5 and 12.5 mg/kg) led to a reduction in the concentration of hepatic triglycerides in ob/ob mice. In conclusion, the authors suggest that THCV may be useful for the treatment of metabolic syndrome and/or type 2 DM associated with obesity, alone or in combination with existing treatments.
Riedel et al. 101 evaluated the effects of antagonists of synthetic cannabinoid receptors and THCV in fasting and nonfasting mice. A standard fasting protocol and a long-term domestic cage observation system with free-feeding animals were used to assess the feeding behavior of mice treated with the CB1 AM251 antagonist. Likewise, the effects of THCV were also determined in animals with feed released. AM251 suppressed food intake and weight gain in fasting and nonfasting animals. THCV also induced a reduction in weight and hypophagia at doses as low as 3 mg/kg. In conclusion, the authors suggested that THCV is a new compound with hypophagic properties and a potential treatment for obesity.
In a randomized double-blind placebo-controlled clinical trial, 62 subjects with type 2 DM not treated with insulin were randomized to five treatment groups: CBD (100 mg twice daily), THCV (5 mg twice daily), 1: 1 ratio of CBD and THCV (5 mg/5 mg, twice daily), 20: 1 ratio of CBD and THCV (100 mg/5 mg twice daily) or combined placebo for 13 weeks. This study showed that THCV significantly reduced fasting glycemia with parallel improvement in β cell function, as well as increased apolipoprotein A (APO A), and adiponectin compared with placebo, CBD decreased resistin and increased levels of glucose-dependent insulinotropic peptide. CBD and THCV were well tolerated. 144
APO A is an important structural protein and an indispensable component of high-density lipoprotein, which plays an essential role in the reverse transport of cholesterol and in the homeostasis of cellular cholesterol. It also plays a multifunctional role in immunity, inflammation, apoptosis, viral, bacterial infection, and so on. 145
Adiponectin is the most abundant peptide secreted by adipocytes, the reduction of which plays a central role in diseases associated with obesity, such as insulin resistance/type 2 DM and cardiovascular diseases. Evidence has shown that the administration of adiponectin in humans and rodents has insulin sensitizing, antiatherogenic, and anti-inflammatory effects, and, in some situations, also reduces body weight. 146
Resistin, in turn, was initially known as a hormone secreted by adipocytes (adipokine) associated with obesity and insulin resistance in rodents. Currently, it is known that it is primarily expressed and secreted by macrophages in humans. Circulating resistin levels are correlated with inflammatory markers, such as C-reactive protein, TNF-α, and IL-6 in the general population and in individuals with DM2, coronary atherosclerosis, rheumatoid arthritis, and/or sepsis.147–152
It has been suggested that the antiobesity characteristic of THCV can be attributed to its ability to interact with other receptor sites. Evidence has shown that THCV interacts with different transient receptor potential channels (TRP), including TRP vanilloid 1 (TRPV1) and TRP vanilloid 2 (TRPV2).142,153 TRP channels are a group of membrane proteins involved in the transduction of a multitude of chemical and physical stimuli. These channels coordinate the entry of ions, mediating several neural signaling processes involved in the sensations of temperature, pressure, and pH, in addition to smell, taste, vision, and pain perception. Several diseases are associated with TRP channel dysfunction, including neuropathic pain, inflammation, and respiratory disorders. 154
The stimulating effects of cannabinoids on TRPV1 and TRPV2 channels result in desensitization of these channels. Desensitization can have important consequences for the potential use of cannabinoids as therapeutic agents, especially in those disorders in which these channels have been shown to be involved and play a permissive role, such as inflammation, and may contribute to the effects anti-inflammatory, analgesic, and anticancer.142,153
It is well established that the ECS is associated with both the control of energy balance and the development of obesity. Cannabinoid receptor antagonists and neutral antagonists are understood to inhibit food intake. 140 Whereas, conversely, the activation of the CB1 receptor by agonists stimulates short-term feeding when administered acutely. 155 The main psychoactive compound of Cannabis sativa, THC, increases food intake and synthetic THC, Dronabinol®, is prescribed as an appetite stimulant, as well as for the improvement of chemotherapy-induced nausea and vomiting. 156 However, contrary to what might be expected, the BMI of regular cannabis smokers was lower than that of nonusers. 157
There is ample evidence that exposure to cannabis and/or THC causes negative regulation of CB1. Continued use of cannabis is associated with desensitization and negative regulation of CB1, and CB1 levels remain low for 3–4 weeks after stopping use.158–162 CB1 is known to play an essential role in the assimilation, storage, and conservation of energy, and this reduced regulation leads to a decrease in endocannabinoid tone. 82 Therefore, BMI is reduced in cannabis users and is expected to decrease further when users stop using cannabis, as CB1 remains under reduced regulation for many weeks after chronic cannabis use.158–162
Recently, abstinent users would experience reduced appetite and increased metabolic rates during this period. However, they will no longer have short-term stimulation of appetite, energy intake, and storage and decreased metabolic rates during each episode of acute cannabis use. Therefore, weight loss will increase as energy intake and storage remain reduced and metabolism stimulated, until CB1 returns to levels before cannabis use. 82
In view of this, Cluny et al. 163 investigated the effect of chronic THC administration on body weight and intestinal microbiota in DIO and lean mice. DIO adult males and lean mice were treated daily with vehicle or THC (2 mg/kg for 3 weeks and 4 mg/kg for an additional week). The results showed that THC reduced weight gain, fat mass gain, and energy intake in DIO, but not in lean mice. This effect may be associated with the fact that THC is a partial agonist of the CB1 and CB2 receptors. Thus, it does not produce maximum stimulation of the aforementioned receptors and may prevent complete endogenous agonists, such as anandamide, from binding to CB1 receptors in situations of high endocannabinoid tone, as observed in obesity. They also showed that DIO-induced changes in the selected intestinal microbiota were prevented in mice administered chronically with THC.
The intestinal microbiota alters endocannabinoid signaling in obesity; increasing intestinal permeability and favoring low-grade inflammation associated with obesity and influencing adipogenesis. 164 This study demonstrates that THC-induced weight gain prevention is associated with changes in the microbiota. In the same study, the authors observed an increase in the abundance of Akkermansia muciniphila in DIO mice treated with chronic THC. The abundance of A. muciniphila, a bacterium that deteriorates mucin, has been inversely associated with body fat mass and glucose intolerance in rats. 165
A. muciniphila has been characterized as a beneficial participant in body metabolism and has great prospects for the treatment of obesity-related metabolic disorders, in addition to being considered as a state-of-the-art therapeutic agent. It can reduce the serum level of inflammatory cytokines, such as IL-2, interferon-gamma, subunit beta of interleukin 12 (IL-12p40), and monocyte chemoattractant protein-1 (MCP-1) (Fig. 2).166,167
In addition, it has previously been indicated that THC has a beneficial effect on the regulation of insulin sensitivity in adipocytes resistant to this hormone. In a study by Gallant et al. 168 was evaluated the biological effects of a lipophilic Cannabis sativa extract containing THC levels ranging from 2.5 to 10 mg/mL, in normal and insulin-resistant 3T3-L1 adipocytes.
The results demonstrated that the extract considerably improved the gene expression of the glucose transporter isotype 4 (GLUT4), and the insulin receptor substrate 1 and 2 (IRS-1 and IRS-2), in addition to decreasing adipogenesis in an in vitro model, thus optimizing the ability of adipocytes to respond to insulin stimulation. In the same study, it was observed that the level of TNF-α in 3T3-L1 cells was significantly reduced in the presence of the extract containing THC, which also improved the sensitivity of cells to insulin.
In a study by Ngueta et al., 169 the relationship between cannabis use, obesity, and insulin resistance was analyzed. Data from 786 Inuit adults from the Nunavik Inuit Health Survey (2004) were analyzed. Information on cannabis use was obtained from a self-administered questionnaire.
The results showed that cannabis use was highly prevalent in the study population (57.4%) and was statistically associated with lower BMI (p<0.001), lower% of fat mass (p<0.001), lower fasting insulin (p=0.04), and lower homeostasis model assessment of insulin resistance (HOMA-IR) (p=0.01), after adjusting for several confounding variables. The authors concluded that the use of cannabis was associated with a lower BMI, and this association did not occur through the glucose metabolic process or related inflammatory markers. The association between cannabis use and insulin resistance was mediated by its influence on weight.
Rajavashisth et al. 170 conducted a cross-sectional study to determine the association between DM and cannabis use. The study included participants from NHANES III, a nationally representative sample of the U.S. population. The total analytical sample was 10,896 adults. The study included four groups (n=10,896): nonusers of cannabis (61.0%), ex-users of cannabis (30.7%), light (once to four times/month; 5.0%), and heavy (more than five times/month) current cannabis users (3.3%). DM was defined based on self-report or abnormal glycemic parameters. The results showed that cannabis users had a lower prevalence of age-adjusted DM compared with non-cannabis users (odds ratio [OR] 0.42, 95% confidence interval [CI] 0.33–0.55; p<0.0001).
A meta-analysis, conducted by Alshaarawy and Anthony, showed epidemiological estimates of eight independent replicates (1) of the National Health and Nutrition Examination Surveys and (2) of the National Drug and Health Surveys (2005–12). For each participant in the national survey, computer-assisted self-interviews assessed cannabis smoking (CS) and DM diagnosed by doctors. The results showed that recently active CS and DM are inversely associated. The OR of the meta-analytical summary is 0.7 (95% CI 0.6–0.8). 171
Klein et al. 172 examined the interactions between THC and CBD during chronic treatment and at equivalent doses. Adolescent rats were treated with increasing daily doses of THC for 21 days (1 and 3 and 10 mg/kg). Some rats received equivalent doses of CBD 20 min before each THC injection to allow examination of possible antagonistic effects of CBD. The findings showed that CBD potentiated an inhibition of body weight gain caused by chronic THC.
A publication by Le Foll et al. 130 suggested that chronic treatment with THC, as well as administration of combined THC/CBD medications in carefully controlled circumstances, can lead to weight loss and possibly improvement of metabolic symptoms in individuals with obesity. It is possible for THC to maintain its effectiveness in combination with CBD, but this has not yet been determined.
According to Clark et al., 82 an increase in the ratio of omega-6 to omega-3 fatty acids contributes to obesity rates by increasing the levels of endocannabinoid N-arachidonoylethanolamide (or anandamide) and 2-AG, overstimulating CB1 and leading to increased caloric intake, reduced metabolic rates, and weight gain. Cannabis, or THC, also stimulates CB1 and increases caloric intake during acute exposures. Thus, the authors conducted a meta-analysis to establish a relationship between the use of cannabis and the BMI and provide a theoretical explanation for this relationship. BMI data for cannabis users and nonusers, or studies reporting adjusted ORs for obese or overweight cannabis users, were obtained from the literature.
Studies addressing the health impact of cannabis use have been identified using database searches and citation lists. The present meta-analysis revealed that the BMI and obesity rates are significantly reduced in cannabis users, together with the increase in caloric intake. The authors provide, for the first time, a causal explanation for this paradox, in which the rapid and long-lasting regulation of CB1 after acute cannabis consumption reduces energy storage and increases metabolic rates, thus reversing the impact of the BMI.
CBD is one of the most common nonpsychotropic constituents of the Cannabis sativa plant. It was revealed that CBD generates a series of pharmacological effects through several mechanisms. It works as a negative allosteric modulator of the CB1 receptor; allosteric modulators of CB1 receptors have the ability to treat the CNS and peripheral disorders, preventing the adverse effects associated with the orthostatic agonism or antagonism of these receptors. 173 Therefore, it has therapeutic potential in the treatment of CNS diseases such as neurodegenerative diseases, epilepsy, anxiety, and depression, without simultaneous psychotic adverse effects.174–176 In addition, it has been indicated that CBD is able to block the CB1 receptor, thus producing antiobesity effects. Conversely, CBD unexpectedly exhibited a high affinity for the CB2 receptor, for which it could act as an agonist. 177 An interesting result of studies is the fact that CBD has a greater affinity for several receptors, including 5-HT1A, TRPV, and PPARγ channels.110,153,178 Activation of the 5-HT1A receptor can act as an antioxidant by capturing ROS preventing membrane oxidation. 179 Therefore, through the activation of 5-HT1A, CBD can neutralize the peroxidation of phospholipids and thus participate in the protection of biomembranes against oxidative changes. 180
CBD activates TRPV, thereby directly or indirectly increasing the level of endogenous anandamide, which is one of the endogenous TRPV1 agonists. Modulation of these channels by cannabinoids, such as CBD, is complex and the relationship between channels and their activation in response to cannabinoids can be further explored for various therapeutic uses, including chronic pain and inflammation. 154
Studies by Hegde et al. 181 and by Esposito et al. 109 indicated that CBD considerably induced PPARγ transcriptional activity. It is known that PPARγ is a potential therapeutic target for the treatment of inflammatory disorders due to its important role in regulating adipogenesis and lipid storage, as well as in glucose homeostasis, lipoprotein metabolism, and inflammation. In addition, it is a central participant in thermogenesis and is an active modulator of lipid metabolism and insulin sensitivity.182,183
Parray and Yun 184 investigated the effects of CBD in inducing the darkening of 3T3-L1 adipocytes. For CBD treatment, 3T3-L1 preadipocytes were incubated with different doses of CBD (1, 5, and 10 μM) during differentiation and until mature adipocyte formation. According to the results, CBD improved the expression of a main set of specific marker genes (Ucp1, Prdm16, Cidea, Fgf21, and Pgc-1α) and proteins (UCP1, PRDM16, and PGC-1α) for brown fat. The increased expression of UCP1 and other specific brown fat markers contributed to the darkening of 3T3-L1 adipocytes, possibly through activation of PPARγ and PI3K.
In addition, CBD increased the levels of protein expression of CPT1, ACSL, SIRT1, and PLIN, while regulating JNK2, SREBP1, and LPL. These data suggest the possible roles of CBD in the darkening of white adipocytes, increased lipolysis, thermogenesis, and reduced lipogenesis. 184
In a study by Ignatowska-Jankowska et al., 177 the effects of repeated administration of CBD on body weight gain in rats were investigated. The animals received intraperitoneal injections of CBD at doses of 2.5 and 5 mg/kg per day for 14 consecutive days and body weight gain was monitored. Both doses of CBD produced a significant decrease in body weight gain, with the effect produced by treatment with 5 mg/kg being more pronounced.
These results suggest that CBD has the ability to alter body weight gain, possibly by acting on the CB2 receptor. CB2 receptors can play a role in regulating body weight. Furthermore, it is important to note that the activation of CB2 leads to a decrease in the levels of ROS and TNF-α, which reduces oxidative stress and inflammation (Fig. 2). 185
In conclusion, the data suggest that CBD plays dual modulating roles in the induction of the brown phenotype, in addition to promoting lipid metabolism. Thus, CBD can be explored as a potentially promising therapeutic agent for the prevention of obesity. 184
Conclusion
From the data presented, it can be concluded that the derivatives of Cannabis sativa can produce an increase in lipolysis, thermogenesis, and a reduction in lipogenesis, playing a role in the regulation of body weight, through action on several receptors. In addition, studies have shown that derivatives of Cannabis sativa can reduce levels of ROS and proinflammatory cytokines such as TNF-α, causing a reduction in oxidative stress and inflammation.
Given the aforementioned, it is clear that phytocannabinoids derived from Cannabis sativa have therapeutic potential due to their anti-inflammatory, antioxidant, and neuroprotective properties, making the plant a study option for reducing and reversing inflammation and comorbidities associated with obesity.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research has not received any specific grants from funding agencies in the public, commercial or non-profit sectors.