
Abstract
Introduction:
Diabetic neuropathies are the most prevalent chronic complications of diabetes, characterized by pain and substantial morbidity. Although many drugs have been approved for the treatment of this type of pain, including gabapentin, tramadol (TMD), and classical opioids, it is common to report short-term results or potentially severe side effects. TMD, recommended as a second-line treatment can lead to unwanted side effects. Cannabidiol (CBD) has been gaining attention recently due to its therapeutic properties, including pain management. This study aimed to characterize the pharmacological interaction between CBD and TMD over the mechanical allodynia associated with experimental diabetes using isobolographic analysis.
Materials and Methods:
After diabetes induction by streptozotocin (STZ), diabetic rats were systemically treated with CBD or TMD alone or in combination (doses calculated based on linear regression of effective dose 40% [ED40]) and had the mechanical threshold evaluated using the electronic Von Frey apparatus. Both experimental and theoretical additive ED40 values (Zmix and Zadd, respectively) were determined for the combination of CBD plus TMD in this model.
Results:
Acute treatment with CBD (3 or 10 mg/kg) or TMD (2.5, 5, 10, or 20 mg/kg) alone or in combination (0.38+1.65 or 1.14+4.95 mg/kg) significantly improved the mechanical allodynia in STZ-diabetic rats. Isobolographic analysis revealed that experimental ED40 of the combination (Zmix) was 1.9 mg/kg (95% confidence interval [CI]=1.2–2.9) and did not differ from the theoretical additive ED40 2.0 mg/kg (95% CI=1.5–2.8; Zadd), suggesting an additive antinociceptive effect in this model.
Conclusions:
Using an isobolographic analysis, these results provide evidence of additive pharmacological interaction between CBD and TMD over the neuropathic pain associated with experimental diabetes induced by STZ.
Introduction
Diabetes has become one of the largest health issues of the 21st century. According to the International Diabetes Federation, it was estimated that 463 million adults had diabetes in 2019 globally, and this is expected to reach ∼700 million people by 2045. 1
Peripheral diabetic neuropathy (PDN) is one of the most common and debilitating outcomes of the disease, 2 affecting about 50% of diabetic patients.3,4 The most reported symptoms of patients with PDN are grouped into positive symptoms, including pain, dysesthesia, tingling, and itching, and negative symptoms such as numbness, muscle weakness, and trouble with balance. 5 Some additional manifestations are described by patients who manifest the painful form of PDN, which include hyperalgesia, allodynia, prickling, pins and needles, electric shocks, burning, stabbing, and dull aching.6,7 When compared with nonpainful PDN, the painful PDN can lead to considerably increased morbidity and a decreased quality of life, reducing productivity and employability. 8
Due to the multiplicity of mechanisms that lead to the development of diabetic neuropathic pain (DNP), pharmacological management is multimodal. First-line drug treatments include dual antidepressants or anticonvulsants. 9 If these treatments are unsuccessful, weak opioids such as tramadol (TMD) are recommended as a second-line treatment, or strong opioids such as oxycodone or morphine may be prescribed as a third-line treatment. 10 Even after such pharmacological approaches, alone or in combination, less than one-third of patients reach 50% of pain relief, which represents a challenge in clinical practice.11,12
The use of opioids clinically has become highly controversial although several studies have shown that opioid analgesics have provided great relief of neuropathic pain when compared with placebo, 13 with an analgesic relief equivalent to that found with antidepressants or gabapentin. 14 Being an atypical opioid, TMD has a double action mechanism: selective action on the μ-opioid receptors and inhibition of norepinephrine and 5-HT reuptake, modulating descending monoaminergic inhibitory pathways. 15 TMD is primarily reserved for those patients who do not respond well to first-line drugs, often not as a substitute therapy, but taken simultaneously with these classes of drugs. In addition, TMD, depending on adopted doses, may induce several side effects, such as vomiting, nausea, dizziness, and constipation, 16 which limits its routine use in medical practice. 17
The combined administration of dual antidepressants with TMD may precipitate serotonergic syndrome. 18 Thus, a safer alternative is needed. In this way, cannabidiol (CBD), a nonpsychoactive compound and the second most abundant phytocannabinoid found in the Cannabis sativa plant, has been gaining much notice recently in many countries in terms of its therapeutic properties and its legal liberation in medicinal practices.
CBD has been shown to produce a therapeutic effect in different conditions such as inflammation, oxidative stress, and nerve loss.19–21 These properties are due to CBD's action upon multiple targets such as the serotonergic system,22,23 noncompetitive negative allosteric modulator of CB1 receptors, 24 inhibition of cellular uptake and catabolism of anandamide, 25 and others.26–28 CBD has also been associated with allosteric modulation of μ and δ-opioid receptors at high doses, and it may as well be a valid alternative to opioids in the clinical setting. 29 In addition, considering CBD's favorable safety profile,30,31 issues associated with TMD use, including unwanted opioid side effects, could be reduced.
Although research using cannabinoids or CBD for DNP is scarce, our group recently demonstrated the beneficial effect of CBD alone on a nonclinical DNP model. 23 Hence, this study aimed to investigate the type of pharmacological interaction between CBD and TMD on the mechanical allodynia associated with experimental diabetes induced by streptozotocin (STZ) using an isobolographic analysis. 32
Materials and Methods
Experimental animals
All experimental animals (adult male Wistar rats, initially weighing between 180 and 220 g) were provided by the Federal University of Parana's animal breeding facility. The animals were maintained in the appropriate environmental standard conditions of temperature (21±2°C) and illumination cycles (12-h light/12-h dark; lights on at 7 a.m.) housed in groups of four per cage (plastic boxes measuring 41 cm×32 cm×16.5 cm). The wood shaving bedding was replaced daily, with food and water ad libitum. The study was conducted according to the National Institutes of Health (NIH) Guide for the Care and Use of Laboratory Animals (NIH Publication, revised in 1978) and previously approved by the Institutional Ethics Committee at the Federal University of Parana (CEUA/BIO-UFPR: No. 1215) and complied with the guidelines of the Committee for Research and Ethical Issues of the International Association for the Study of Pain. Every possible effort was made to minimize animal suffering and reduce the number of rats used in this study.
Drugs and solutions
STZ was provided by Santa Cruz Biotechnology, Inc., (Santa Cruz, California, USA) and freshly dissolved in sodium citrate buffer (10 mM, pH 4.5; Merck S.A. Pharmaceutical, Brazil). CBD (99.6% pure without any other cannabinoid) was kindly supplied by BSPG-Pharm (Sandwich, UK). TMD was supplied by Hipolabor Pharma (Belo Horizonte, MG, Brazil). CBD stock was provided as a solid and was freshly diluted in a solution of 1:3:16 of tween 80, ethanol, and 0.9% sodium chloride (NaCl) solution, whereas TMD was diluted in 0.9% NaCl solution.
Diabetes induction
After 12 h of overnight fasting, diabetes was induced by a single intraperitoneal (i.p.) injection of STZ (60 mg/kg; freshly dissolved in citrate buffer [10 mM, pH 4.5]; at the volume of 1 mL/kg). The hyperglycemic status was then confirmed 3 days after the STZ administration using blood samples (5 μL) obtained by pricking the rat tail and applying the blood onto test strips containing oxidase glucose (Accu Check Active™; Roche), and again at the end of experimental protocols. Only animals with nonfasting blood glucose levels of 250 mg/dL or greater were considered diabetic and included in the study. A normoglycemic (NGL) control group was conducted in parallel and was treated with an i.p. injection of an equivalent volume of citrate buffer (10 mM, pH 4.5).
Electronic Von Frey test
The withdrawal threshold for mechanical stimulation was assessed with an electronic von Frey apparatus (Insight Ltda, Ribeirão Preto, SP, Brazil), which consisted of a rigid plastic tip (tip area=0.7 mm2) connected to a hand-held probe unit. The rats were placed in an acrylic cage (12 cm×20 cm×17 cm) with a wire-grid floor for 30 min to allow behavioral acclimation to the environment. A tilted mirror below the grid provided a clear view of the animal's hind paws. Increasing upward pressure was applied with the plastic tip against the mid-plantar surface of each hind paw. The applied weight in grams was continuously recorded by the main unit connected to the probe during this procedure. The threshold was determined by the removal of the paw, which is often followed by flinching movements. Thus, the movement of the probe stopped, and the threshold was automatically determined. The average of three measurements with a minimum interval of 3 min was taken. 33
Isobolographic analysis
The time course of mechanical hypersensitivity was constructed using the mechanical threshold in grams measured in the electronic von Frey apparatus against time in minutes or hours after the different treatments. The area under the curve (AUC) was estimated using the trapezoidal method of integration. The initial dose ranges of CBD and TMD were selected based on the previous studies.23,34,35 Antinociceptive effects were measured as a percentage of the maximum possible effect (% MPE) according to the formula: % MPE=100×(A−B)/(C−B), where A is the average mechanical threshold of each animal in the treated group (drugs alone or in combination); B is the mechanical threshold of STZ-induced diabetic animals treated with vehicle; and C is the averaged mechanical threshold of the NGL animals treated with vehicle. Experimental design and statistical isobolographic analysis were conducted essentially as previously described.32,36
Briefly, dose–response curves were first obtained for CBD and TMD administered alone. Line equations, slope values, effective dose 40% (ED40) values, and 95% confidence limits were obtained using linear regression.32,37,38 The slope values were used to assess whether the dose–effect of these drugs alone exhibited a constant potency ratio, which is necessary to perform fixed dose–pair combinations of drugs.32,37,38 Doses of individual drugs in the combinations were determined as a proportion of their ED40 values, considering the different efficacy of the tested drugs. The proportion was constant and estimated based on a factor derived from the individual variances of the ED40 values. This fixed proportion of agents was necessary to assess whether the combination displayed enhanced potency indicative of synergism. The total amount of CBD+TMD in a drug pair treatment was defined as: a + b=c, wherein: a=the quantity of CBD (in mg); b=the quantity of TMD (in mg); and c=sum (in mg) of the quantities of CBD and TMD in the mixture. The proportion of a and b was fixed and calculated according to the formulae bellow: a=A*×f; b=(1−f)×B wherein: A=ED40 of CBD; B=ED40 of TMD; f=proportion factor. The proportion factor f was calculated based on the variances of the ED40 values from CBD (A) and TMD (B) according to the formula: f=V(B)/V(A) + V(B) wherein: V(A)=variance of ED40 of CBD and V(B)=variance of ED40 of TMD.
Dose–response curves of associated drugs are constructed to obtain the doses that achieved the same effect level (40% MPE) compared with drugs given alone. This experimentally obtained ED40 (here called Zmix) was compared (t-test) with a theoretically calculated ED40 value for additive interactions (Zadd). The Zadd was obtained according to the formula Zadd=f×A + (1−f)×B wherein A=ED40 of CBD; B=ED40 of TMD; and f=proportion factor. The variance of Zadd was estimated by the formula: V(Zadd)=f2×V(A) + (1–f)2×V(B) wherein f=proportion factor, V(A) and V(B)=variances of ED40 of CBD and TMD, respectively.
Graphical assessments of synergy are also presented using isobolographic analysis. Measurement of the interaction index (α) was obtained by dividing experimentally obtained ED40 of the drug pair by the theoretical additive ED40 of the drug pair. The γ interaction index provides a measure of the degree of synergism. The level of significance for all tests was set at p<0.05. GraphPad 8 was used for graph creation and statistical analysis.
Experimental protocols
All experimental procedures conducted in the present study are summarized in Figure 1. All test animals were first transported from the Federal University of Parana (UFPR's) breeding facility to a temperature- and light-controlled protected room in the Department of Pharmacology to assimilate to the new environment for at least 3 days. All behavioral tests were conducted in a room with 40 lx of illumination by an experimenter blind to treatments, but not blind to the diabetic condition, since apparent signs of the diabetic condition, including polyuria, polyphagia, polydipsia, and weight gain reduction, are observed. Before diabetes induction, both body weight and the mechanical threshold baseline in the von Frey apparatus were evaluated. After 12 h of fasting, the diabetic designed groups received an i.p. STZ injection (60 mg/kg), while the NGL animals received only an injection with an equivalent volume of citrate buffer. The plasma glucose level was measured 3 days after the injection (peak blood glucose increase after STZ injection), and again at the end of the 4-week experiment to confirm the maintenance of the diabetic state during the experimental period.
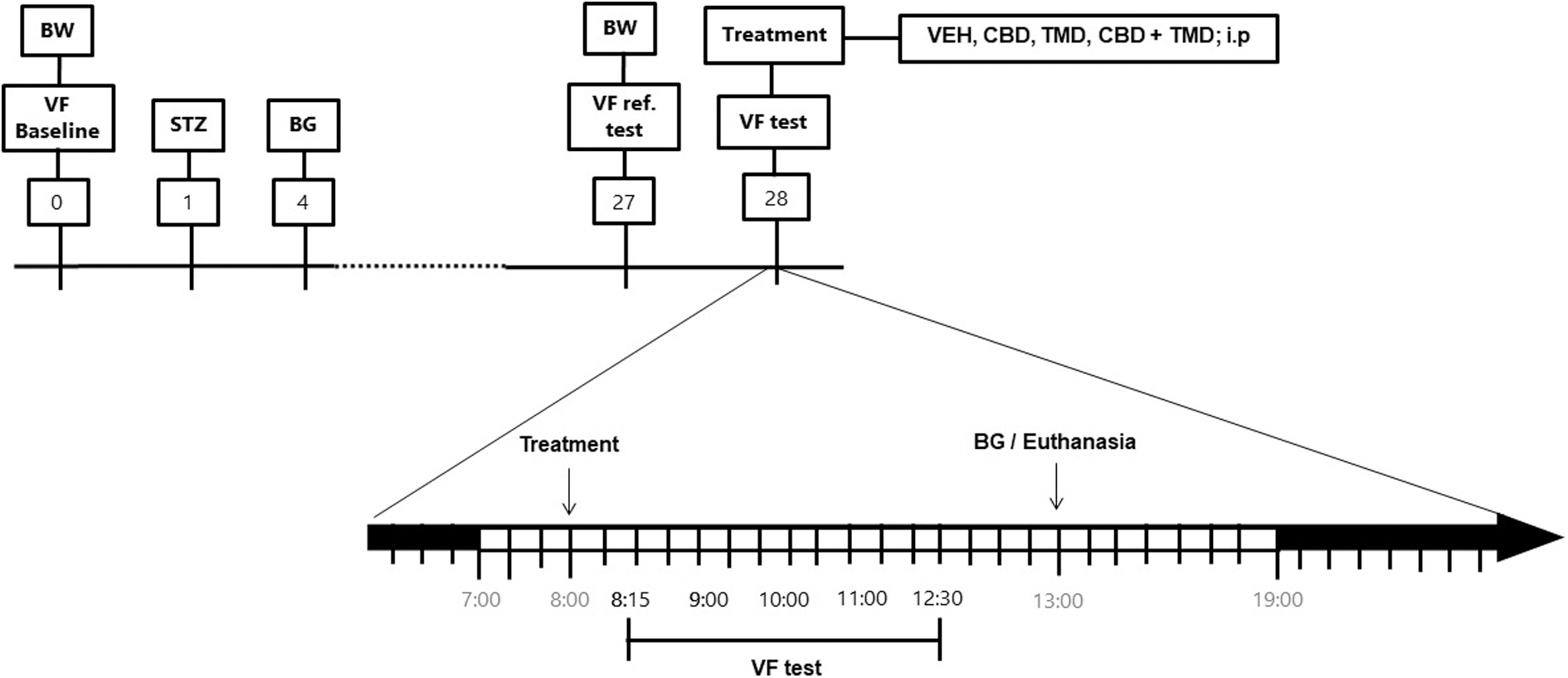
Timeline of the experimental protocol. Numbers represent days after STZ injection. Body weight was measured before STZ and again at the end of the protocol (28 days). The blood glucose levels were measured 3 days after STZ injection and again at the end of the experiment for confirmation of diabetic status. BG, blood glucose; BW, body weight; CBD, cannabidiol; i.p., intraperitoneally; STZ, streptozotocin; TMD, tramadol; VEH, vehicle; VF, electronic von Frey test.
On day 28 after diabetes induction, all animals were again weighted and had the mechanical thresholds evaluated (28 days; reference data). Diabetic animals received CBD (at doses of 0.1, 0.3, 1, 3, or 10 mg/kg; i.p.; at the volume of 1 mL/kg; based on previous studies from our group),23,35 TMD (1.25, 2.5, 5, 10, or 20 mg/kg; i.p. at the volume of 1 mL/kg 34 ) or the combination of CBD and TMD (CBD was injected 30 min before the TMD administration; both i.p. at the volume of 1 mL/kg each; 0.04+0.18 mg; 0.13+0.55 mg; 0.38+1.65 mg or 1.14+4.95 mg; calculated as described above). The mechanical threshold was then reevaluated 60, 120, 180, and 240 min after CBD injection. This time marker was selected based on the pharmacokinetics of CBD after systemic treatment, whose plasmatic level's peak is 1–2 h in both rats and humans. 39
The mechanical withdrawal threshold was measured 15, 30, 60, 120, 180, and 240 min after TMD single-dose injection, following previous studies. 34 When tested in combination, the mechanical thresholds were evaluated 30, 60, 120, 180, and 240 min after the TMD injection. The control group of NGL or diabetic animals treated with vehicle were also documented throughout the experiments.
Statistical analyses
All data are presented as mean±standard error of the mean per experimental group. Data were analyzed by one-way ANOVA followed by Bonferroni post-hoc for the comparison between the experimental groups or two-way ANOVA (treatment and time) followed by Bonferroni post-hoc for multiple comparisons of experimental groups within each time point. The statistical analyses of dose–response curves were made between subjects. The level of significance was set at p<0.05. All tests were conducted using the GraphPad Prism software (version 9.1.0; San Diego, CA, USA). All statistical analyzes (with specific p values) are shown in the Supplementary Tables S4–S15).
Results
Effect of acute treatment with CBD over the mechanical allodynia associated with experimental diabetes
As shown in Figure 2A and B and corroborating with previous results, while the mechanical withdrawal thresholds of NGL animals did not change throughout the experimental period, the mechanical withdrawal thresholds of all diabetic rats were significantly lower 28 days after STZ injection. In addition, the treatment with CBD reached its MPE at 60 min (Fig. 2A). Two-way ANOVA with repeated measures showed the treatment effect [F(6, 56)=15.67; p<0.0001], time effect [F(5, 280)=159.1; p<0.0001], and the interaction between these factors [F(30, 280)=6.657; p<0.0001]. Bonferroni's post-hoc test showed that the decrease of mechanical allodynia was maximal at 60 min after CBD (0.3 to 10 mg/kg) treatment, which elicited a significant increase in the force required for paw withdrawal in a dose-dependent manner and lasted until 120 min at the 3 and 10 mg/kg doses (p<0.05, when compared with STZ+VEH-treated group). Administration of the lower dose of CBD (0.1 mg/kg) had no effects on mechanical allodynia (Fig. 2A).
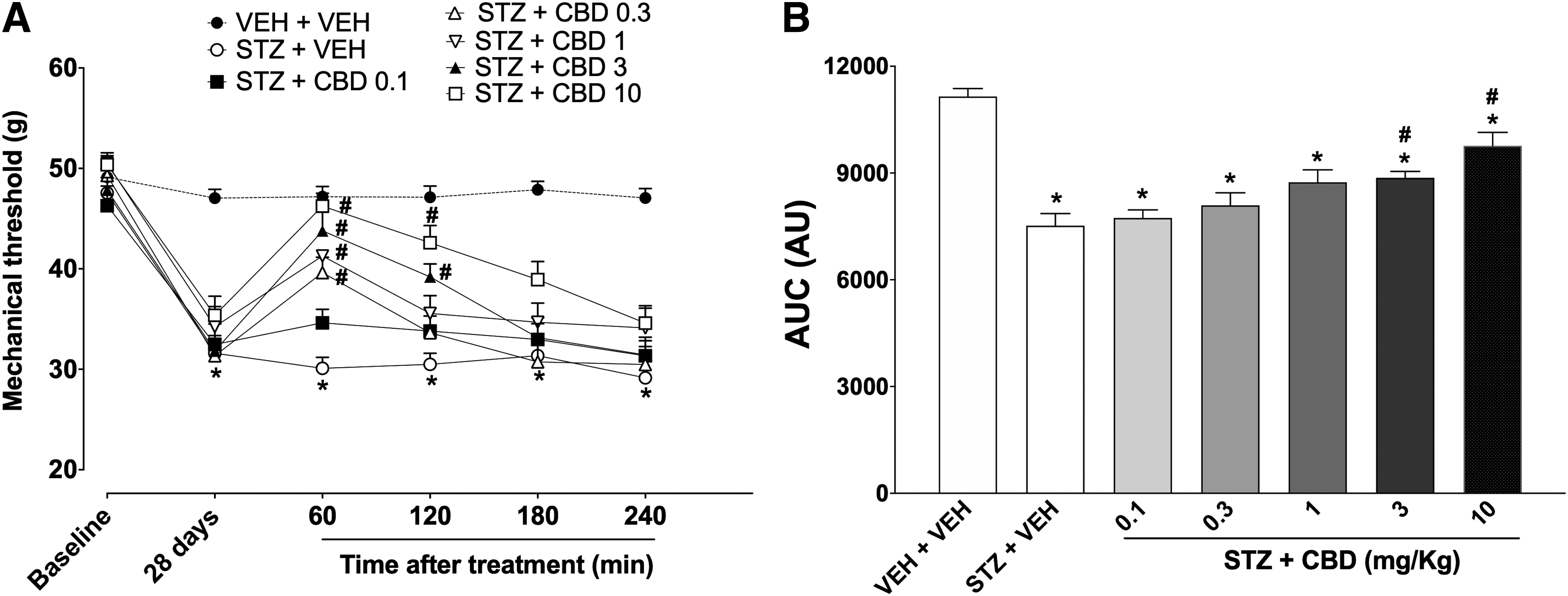
Effect of CBD treatment over the mechanical allodynia in STZ-diabetic rats.
Analyzing the AUC of the total mechanical threshold for 4 h after the CBD treatment, one-way ANOVA showed a significant effect of the treatments [F(6, 56)=17.08; p<0.0001]. Bonferroni's post-hoc test showed that the experimental groups treated with STZ were significantly different when compared with the vehicle-treated NGL control group, except for rats treated with CBD 10 mg/kg. Diabetic groups treated with CBD (at doses of 3 or 10 mg/kg) were statistically different from the vehicle-treated diabetic control group (p<0.05; Fig. 2B).
Effect of acute treatment with TMD over the mechanical allodynia associated with experimental diabetes
Two-way ANOVA with repeated measures shows the treatment effect [F(6, 44)=21.80; p<0.0001], time [F(7, 308)=106.1; p<0.0001], and in the interaction between these factors [F(42, 308)=7.606; p<0.0001] (Fig. 3). Bonferroni's post-hoc showed a significant difference between the vehicle-treated diabetic group (STZ+VEH) and those treated with TMD (at doses of 5, 10, and 20 mg/kg, 15 min after treatment and at doses of 2.5, 5, 10, or 20 mg/kg from 30 to 120 min after treatment). From 180 min onward, there were no significant statistical differences between the TMD-treated groups compared with the vehicle-treated control group (p>0.05; Fig. 3A).
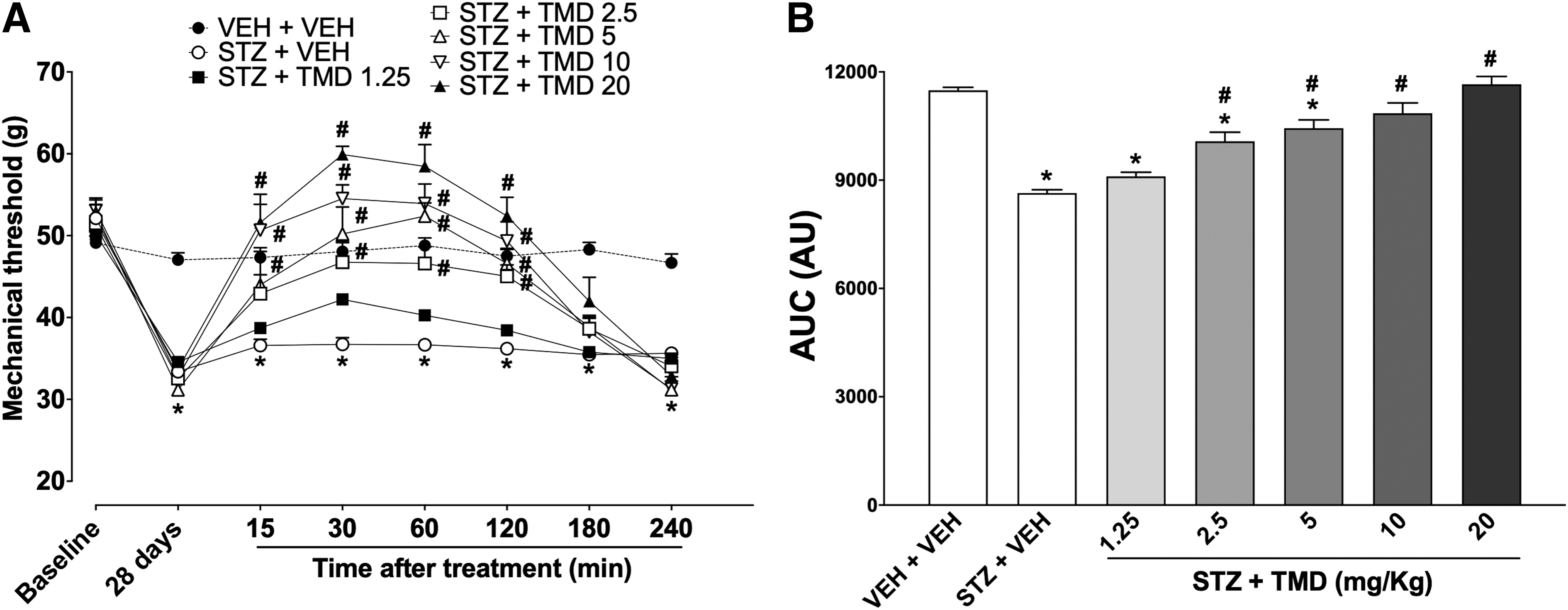
Effect of TMD treatment over the mechanical allodynia in STZ-diabetic rats.
The cumulative effect of the TMD treatment is shown in Figure 3B. One-way ANOVA analysis shows treatment effect [F(6, 44)=28.50; p<0.0001]. Bonferroni's post-hoc test showed that the experimental groups treated with STZ (except those treated with TMD 10 or 20 mg/kg) were significantly different when compared with the vehicle-treated NGL control group. Diabetic groups treated with TMD (at doses of 2.5, 5, 10, or 20 mg/kg) were statistically different from the vehicle-treated diabetic control group (p<0.05).
Effect of acute treatment with CBD and TMD over the mechanical allodynia associated with experimental diabetes: ED calculation and isobolographic analysis
The slope ED40 values, considering the cumulative effect during the experimental time course and on the peak of effect (60 min after the treatments) as well as the 95% confidence limits are demonstrated in Fig. 4 (panels A and B, respectively). According to dose–response curves (Fig. 4C, D), CBD reduced the mechanical allodynia with an experimental ED40=2.8 (95% confidence interval [CI]=1.2–6.3; total effect) or 0.5 (95% CI=0.3–1.2; 60 min after the treatment). TMD reduced the mechanical allodynia with an experimental ED40=1.9 (95% CI=1.4–2.7; total effect) or 1.1 (95% CI=0.7–1.8; 1 h after the treatment) (Table 1).
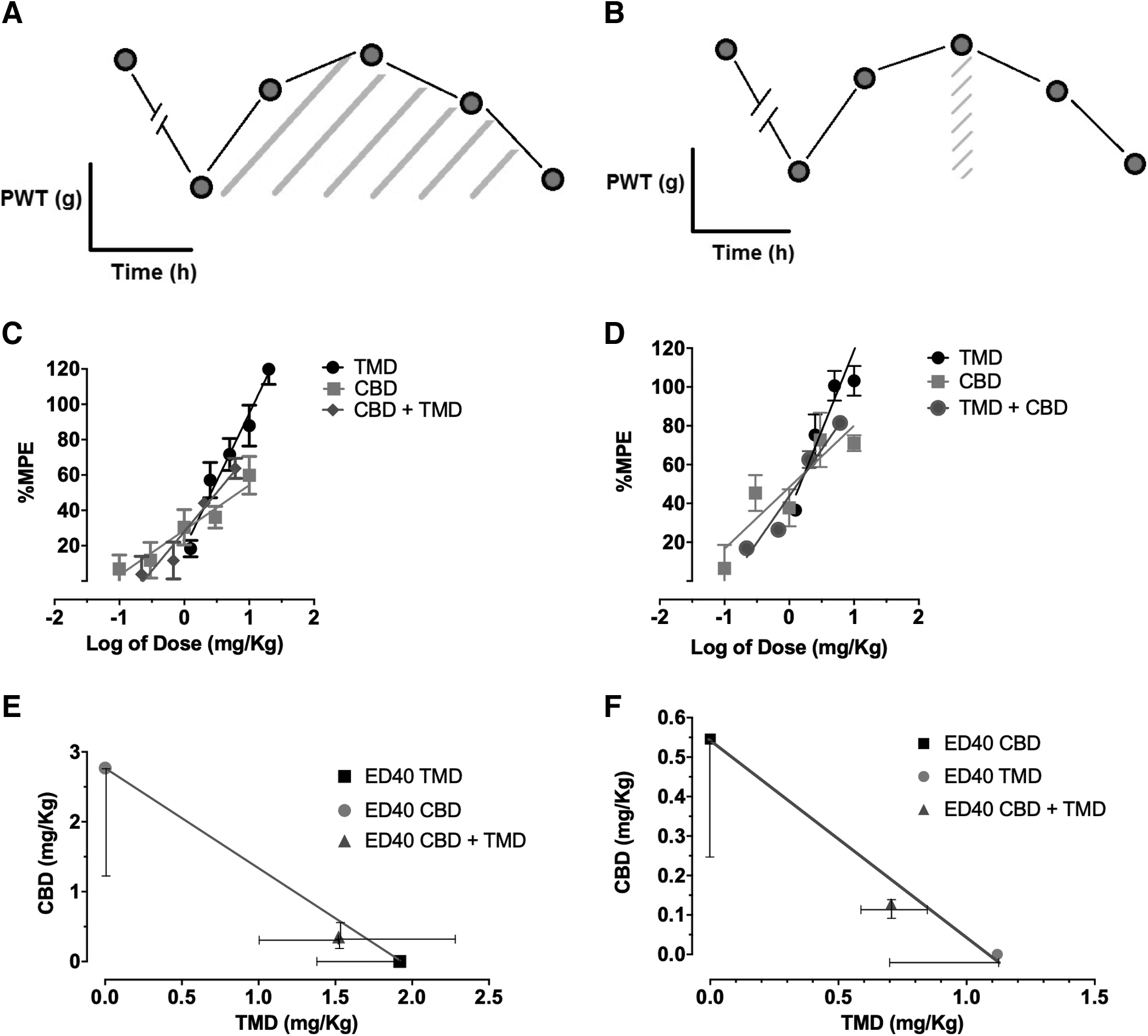
Isobolographic analysis of the antinociceptive interaction between CBD and TMD over the mechanical allodynia associated with experimental diabetes induced by STZ in rats. Percentages (%) of MPE were normalized as a function of the area under the curve
Antinociceptive Effective Dose 40% of the Agents over Mechanical Allodynia in STZ-Diabetic Rats
Antinociceptive doses ED40 are expressed in mg/kg. Values in parenthesis are 95% confidence intervals. The ED40 was determined from the dose–response curves. The theoretical additive (Zadd) was calculated based on the dose–response curves of the agents alone. The combined (Zmix) was determined from the experimentally determined dose–response curves of CBD+TMD.
Additive interaction (p>0.05 vs. theoretical additive).
AUC, area under the curve; CBD, cannabidiol; ED40, effective dose 40%; MPE, maximum possible effect; TMD, tramadol.
The antinociceptive effect of acute i.p. administration of CBD plus TMD combination over the mechanical allodynia in STZ-diabetic rats was evaluated experimentally (Fig. 5A, B). Two-way ANOVA with repeated measures shows the treatment effect [F(5, 38)=25.89; p<0.0001], time [F(6, 228)=284.9; p<0.0001], and in the interaction between these factors [F(30, 228)=17.40; p<0.0001]. Bonferroni's post-hoc showed a significant difference between the vehicle-treated diabetic group (STZ+VEH) and those treated with combinations of CBD and TMD (at doses of 0.38+1.65 or 1.14+4.95 from 30 to 120 min after treatment and doses of 1.14+4.95, this effect was sustained until 180 min after treatment). At 240 min, none of the tested doses of the combinations CBD plus TMD was sufficient to significantly alter the mechanical allodynia in diabetic animals (Fig. 5A).
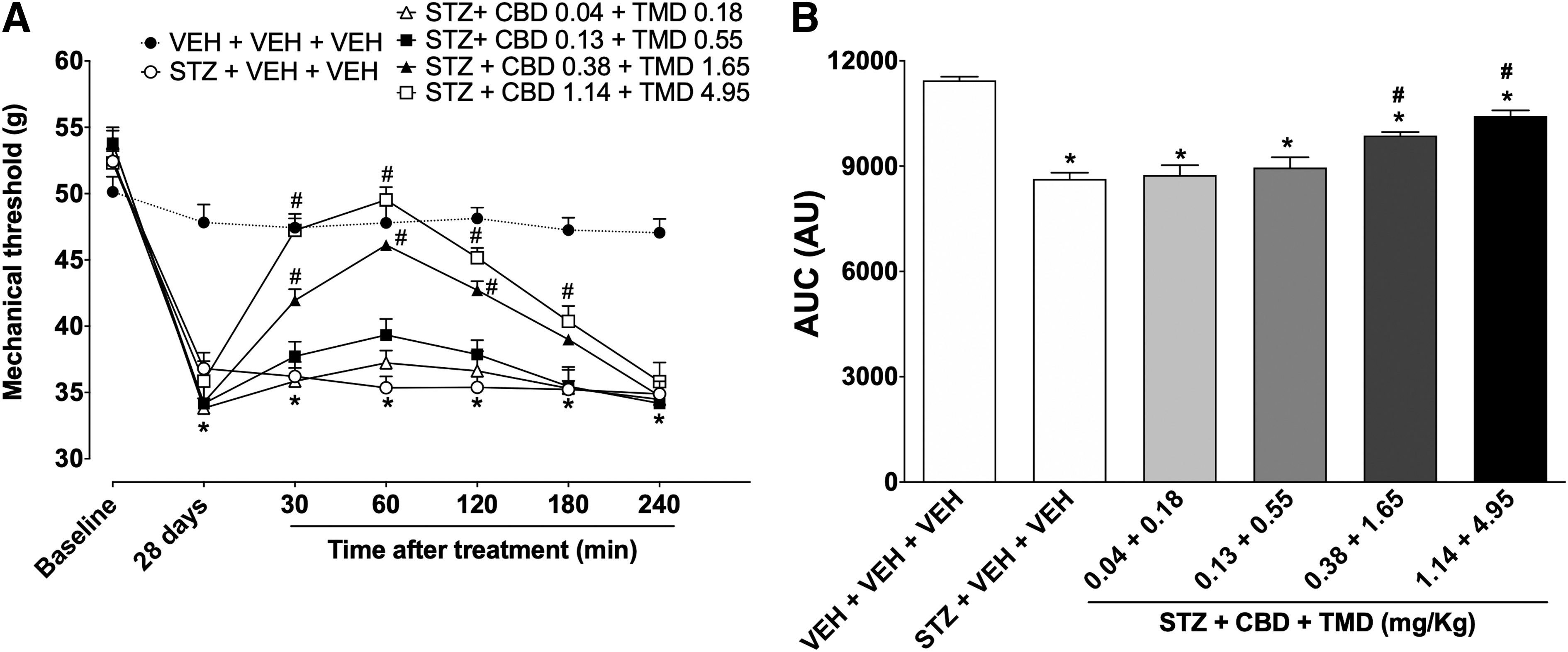
Effect of combined treatment with CBD and TMD treatment over the mechanical allodynia in STZ-diabetic rats.
The cumulative effect of the combination of CBD and TMD treatment is shown in Figure 5B. One-way ANOVA analysis shows treatment effect [F(5, 38)=33.20; p<0.0001]. Bonferroni's post-hoc showed that all experimental groups treated with STZ were significantly different when compared with the vehicle-treated NGL control group. Diabetic groups treated with CBD and TMD (at doses of 0.38+1.65 or 1.14+4.95) were statistically different from the vehicle-treated diabetic control group (STZ+VEH; p<0.05; Fig. 5B).
The isobolographic analysis (considering the % MPE as a function of the AUC for up to 240 min after treatment) revealed that experimental ED40 of the combination (Zmix) was 1.9 mg/kg (95% CI=1.2–2.9) (Fig. 4D and Table 1), and it did not differ from the theoretical additive ED40 2.0 mg/kg (95% CI=1.5–2.8) (Zadd; Student's t-test; p>0.05). This value lies close to the theoretical line of additivity, indicating that the antinociceptive interaction between CBD and TMD is additive in our model (Table 1).
To assess whether the antinociceptive interaction could be underestimated at the peak of action, we performed a new analysis estimating the % MPE as a function of the threshold at the peak of action (60 min after treatment; Fig. 4F). The averaged ED40 values of drugs alone or in combination were lower than those values seen in the AUC analysis (Table 1). Despite this, the experimental ED40 (Zmix) of the combination at the peak of action was not statistically different from the ED40 theoretical additive (Zadd), corroborating an additive interaction (Fig. 4F).
Discussion
Pharmacological interaction studies might be an opportunity to develop possible therapeutic strategies to improve the use of opioids. In the present study, using an experimental model of DNP induced by STZ, we demonstrated that systemic treatment with CBD and TMD per se or combined induced a significant antinociceptive effect on mechanical allodynia in diabetic rats. In the framework of the isobolographic analysis, this study showed that CBD and TMD exert an additive antinociceptive effect in this animal model of DNP.
STZ is one of the most utilized animal models for the chemical induction of diabetes, resulting in classic signs (polyuria, polyphagia, hyperglycemia) soon after its systemic administration. About changes in biophysical and behavioral parameters, it is also well established that the peak occurs about 4 weeks after STZ administration.40–42 In this study, treatments with CBD and TMD alone or in combination were performed during week 4 (28 days). We observed, as expected that all STZ-treated animals had a significant reduction in body weight during the 4 weeks of experiment and had a significant increase in blood glycemia. Furthermore, none of these acute treatments (alone or in combination) was able to alter either the blood glycemia or the body weight of the diabetic rats when compared with the vehicle-treated diabetic control groups (Supplementary Tables S2 and S3).
Previous studies from our department and others have already demonstrated that the systemic treatment with CBD alone reduced neuropathic pain associated with, or without diabetes.22,23,26 CBD has been shown to produce therapeutic effects in pain states and in different conditions such as inflammation, oxidative stress, and nerve loss due to the broad spectrum of targets that CBD acts on.43–45 Considering DNP, the antinociceptive effect of CBD over the mechanical allodynia in STZ-diabetic rats is prevented by 5-HT1A receptor antagonist intrathecal treatment, but not by CB1 or CB2 cannabinoid receptor antagonists. Moreover, the acute treatment with CBD increased the spinal levels of 5-HT in STZ-diabetic rats. 23
The antinociceptive effect of TMD over neuropathic pain states has already been described in the literature previously (for review see Duehmke et al. 46 ). It acts as a weak μ-opioid agonist and has a range of other sites that may contribute to its analgesic effect, including 5-HT and norepinephrine reuptake inhibition. Although classified as an atypical opioid, TMD use is associated with many classic opioid side effects such as nausea and vomiting, constipation, and respiratory depression that usually manifest in a dose-dependent manner. 47 Our results demonstrated a significant antinociceptive effect of TMD over the mechanical allodynia associated with experimental diabetes, even after the acute treatment with low doses (2.5 mg/kg), in which the effect lasted up to 2 h after administration. Interestingly, the higher doses of TMD used in this study (10 and 20 mg/kg) induced an increase in the mechanical threshold that exceeded the threshold of the NGL group. Although not investigated in this study, this effect may be associated with the potential sedative effects of opioids, which were probably mediated by its anticholinergic action. 48
Considering the dose–responses, when analyzing the total effect (during 4 h after the CBD or TMD treatment), TMD exhibits lower ED40 when compared with CBD. Conversely, at the peak of action (at 60 min after treatment), CBD exerted the antinociceptive effect with the lowest ED40, corroborating its potential alternative to manage neuropathic pain states related to diabetes.
Drug combinations are very common in the treatment of infections, cancers, and painful neuropathies. When two drugs are administered in adjunct, the results may be greater than or less than the effect of their potencies. The isobologram, a graph that was introduced by Loewe (1953), 32 has been constructed to evaluate and illustrate the effect of two compounds used in combination. While analyzing the line of additivity, one can differentiate the synergistic, additive, or antagonistic interactions. 32 If the combined effect is more significant than their potencies, synergism has occurred. In the case of synergism, it allows for the use of lower doses of individual drugs when used in combination.
In this study, the isobolographic analysis suggested that CBD and TMD exerted an additive antinociceptive effect over the mechanical allodynia associated with experimental diabetes induced by STZ. In the framework of isobolographic analysis, although it has been shown only as an additive-type interaction when analyzed isobolographically, this result may have high clinical relevance since the association of CBD plus TMD induced a significant antinociceptive effect that lasted longer (180 min after the treatment) when tested experimentally at doses below the ED40.
Even after the highest doses, the antinociceptive effect of TMD, or CBD alone, did not exceed 120 min. Although the mechanisms related to this prolongation of the effect have not been investigated, the ability of TMD to prevent the reuptake of 5-HT, 46 and that CBD exerted its antinociceptive effect also dependent on the serotonergic system,22,23 reinforce the idea that both may have a joint and multimodal activity in reducing DNP. In addition, this effect may be related to the allosteric modulation in the μ and δ-opioid receptors by CBD, 29 revealing the feasibility of a possible positive interaction between phytocannabinoids and opioids in the treatment of pain.
Other studies have already investigated possible pharmacological interactions of TMD over experimental pain models.49–52 Interestingly, it has been demonstrated that the interaction between gabapentin and TMD was synergic over the thermal hyperalgesia in STZ-diabetic mice. 51 Considering the combined treatment with TMD and acetaminophen in STZ-diabetic rats, the isobolographic analysis also revealed an additive effect. 34
It is important to mention that, although our findings demonstrate the additive antinociceptive effect of the CBD plus TMD combination, further studies are needed to scale the translational importance of these findings. The benefit of this association may go beyond pain relief and include, for example, opioid sparing and better patient quality of life. The reduction of common adverse effects (nausea, constipation, tolerance, psychomimetic effects, cognitive impairment) or serious adverse effects (overdose, respiratory depression, dependence, and withdrawal) associated with the use of opioids or cannabinoids, in general, can clinically ratify the indication of combinations like the one investigated in the present study.
Conclusion
Altogether, for the first time, our data provided evidence of a pharmacological interaction between CBD and TMD over the mechanical allodynia associated with experimental diabetes. Although these drugs interact in an additive way, the extension of the antinociceptive effect and a possible reduction of side effects associated with the use of opioids may somehow represent a pharmacological advantage of the use of these drugs in combination. These results together may provide support for the proposition of using CBD combined with opioids for the management of DNP, with fewer adverse effects for the patient suffering from this type of pain.
Footnotes
Data Availability Statement
The results presented in this article have been derived from the doctoral thesis of the student A.A.E., defended on July 9, 2021, at the Federal University of Paraná, as a prerequisite for the attainment of the degree of Philosophy Doctor in Pharmacology. The thesis can be accessed through the following website: https://acervodigital.ufpr.br/bitstream/handle/1884/74542/R%20-%20T%20-%20ALLAN%20ARNOLD%20EVANS.pdf?sequence=1&isAllowed=y)
Acknowledgment
The authors thank BSPG-Pharm (Sandwich, UK) who kindly donated CBD.
Disclaimer
The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; and decision to submit the article for publication.
Author Disclosure Statement
J.A.S.C. is a member of the International Advisory Board of the Australian Center for Cannabinoid Clinical and Research Excellence (ACRE)–National Health and Medical Research Council (NHMRC). J.A.S.C. and J.E.C.H. have received travel support to attend scientific meetings and personal consultation fees from BSPG-Pharm. J.A.S.C., J.E.C.H., and A.W.Z. are coinventors of the patent “Fluorinated CBD compounds, compositions, and uses thereof. Pub. No.: WO/2014/108899. International Application No.: PCT/IL2014/050023,” Def. US number Reg. 62193296; July 29, 2015; INPI on August 19, 2015 (BR1120150164927; Mechoulam R, Zuardi AW, Kapczinski F, Hallak JEC, Guimarães FS, Crippa JAS, Breuer A).
Universidade de São Paulo (USP) has licensed this patent to Phytecs Pharm (USP Resolution No. 15.1.130002.1.1) and has an agreement with Prati-Donaduzzi to “develop a pharmaceutical product containing synthetic CBD and prove its safety and therapeutic efficacy in the treatment of epilepsy, schizophrenia, Parkinson's disease, and anxiety disorders.” J.A.S.C., J.E.C.H., and A.W.Z. are coinventors of the patent “Cannabinoid-containing oral pharmaceutical composition, method for preparing and using same,” INPI on September 16, 2016 (BR 112018005423-2). The other authors declare that they have no conflicts of interest.
Funding Information
This work was supported by the Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP), and by the Instituto Nacional de Ciência e Tecnologia Translational em Medicina (INCT-TM; CNPq/FAPESP; 2008/09009-2; 2020/05416-4). J.A.S.C. received a grant from the University Global Partnership Network (UGPN)–Global Priorities in Cannabinoid Research Excellence Program. J.A.S.C., J.E.C.H., and A.W.Z., are recipients of CNPq research fellowships.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.