
Abstract
Purpose:
The purpose of this pilot study was to investigate cannabidiol (CBD) cream’s effects on muscle soreness and performance after exercise.
Materials and Methods:
This double-blinded, placebo-controlled experiment included 15 men and 13 women (n = 28; mean ± standard deviation age: 23.29 ± 2.54 years) untrained in lower-body resistance training. Participants were randomized into control (NG, n = 9), CBD (CG, n = 9), or placebo (PG, n = 10) groups. Participants completed a lower-body fatigue protocol (FP) consisting of unilateral maximal concentric and eccentric isokinetic muscle actions of the quadriceps and hamstrings (5 sets, 10 repetitions, both legs). CG and PG participants applied ∼100 mg CBD or placebo cream, respectively, matched for weight and appearance to the quadriceps on three separate days. NG participants engaged in a sitting rest period matched in duration to cream application processes. Questionnaires, pressure–pain threshold (PPT), peak torque test (PTT), and countermovement jump (CMJ) were assessed. Mixed-model analysis of variance was conducted to assess main effects and interactions (group × muscle × time; group × time).
Results:
There were no significant interactions or main effects for group for PPT, CMJ, or PTT. There were main effects for time (p < 0.05) for all soreness questions, PPT, CMJ, and PTT. There was one significant interaction (group × time; p = 0.045) for cream/rest effect questions, in which PG participants perceived the effect of cream to be greater than the effect of rest for NG participants. There were main effects for group (p ≤ 0.031) for all soreness questions, in which PG participants perceived enhanced recovery.
Conclusions:
The present pilot study did not discover any significant impacts of CBD cream use for muscle recovery. For individuals seeking to attenuate muscle soreness and improve performance, the current dose of this topical CBD product may not be an effective treatment.
Introduction
Exercise-induced muscle damage (EIMD) results from unaccustomed exercise 1 and is associated with impaired muscle function and delayed onset muscle soreness (DOMS). 2 Muscular impairments may reduce performance capabilities due to decreased joint proprioception, decreased strength and power, altered joint kinematics, and altered muscle recruitment patterns. 3 DOMS typically peaks within 24–48 h post-exercise but may persist for 5–7 days, 4 influencing investigations into novel recovery interventions to optimize recovery.
Cannabidiol (CBD), an active compound derived from the cannabis plant, has increased in popularity 5 and has been purported to attenuate soreness and pain.6–8 This nonintoxicating cannabinoid interacts with cannabinoid receptors (CB1 and CB2) within the endocannabinoid system (ECS) 9 as well as other molecular targets, such as transient receptor potential (TRP) channels, to yield diverse physiological effects including antinociception. 10 Coupled with no evidence of abuse potential, 11 CBD has generated innumerable attention from medical and sport communities.
Anecdotally, there is evidence to support the efficacy of CBD for pain relief,6–8 but clinical trials have yielded conflicting results. In some experiments, oral CBD supplementation (150 mg dose 12 and 5 mg/kg body mass dose 13 ) had no effect on either muscle soreness or muscle function. However, other studies have suggested oral CBD intake results in a quicker reduction in muscle pain (16.67 mg), 14 enhanced ratings of pleasure during exercise (300 mg), 15 a greater retention of anaerobic fitness level over time (50 mg), 16 and faster recovery of muscle function (60 mg) 17 when using CBD. Discussions on social media regarding CBD’s use as a topical cosmetic 18 have drawn attention to CBD cream. In a pilot study to assess tolerability of CBD cream (10 mg, administered twice daily), results indicated CBD was well tolerated and yielded significant improvements in self-reported pain. 19 Furthermore, there is evidence to suggest CBD may modulate TRP channels (TRPV1-4, TRPA1, and TRPM8), suggesting a topical formulation may have potential to attenuate localized muscular pain.20,21 However, clinical evidence supporting the use of topical CBD for muscle soreness and recovery is both scarce and conflicting. For example, Alpy et al. reported 1000 mg of CBD ointment had no effects on maximal voluntary isometric contractions (MVICs) for elbow flexion or ratings of soreness, 22 whereas Xu et al. reported 250 mg of topical CBD oil significantly reduced pain in patients with peripheral neuropathy. 23 Notably, these experiments did not assess dynamic muscular function through a range of motion or pressure–pain sensitivity. Therefore, the efficacy of CBD cream for muscle soreness and recovery using a variety of measures should be investigated.
The purposes of this investigation were to assess the effect of topical CBD on (1) muscle soreness (local and systemic) and (2) voluntary muscular performance following fatiguing exercise. We hypothesized that (1) CBD cream would decrease perceived local muscle soreness when compared with a placebo or control group and (2) recovery of muscular power would be quicker when CBD cream is applied when compared with a placebo or control group.
Materials and Methods
Study design
This study was a randomized, double-blinded, placebo-controlled experiment. Participants were divided into three experimental groups, randomized, and matched for age and biological sex: control group (NG), CBD group (CG), and placebo group (PG). Randomization and cream allocation were conducted by an independent investigator with no involvement in the recruitment, data collection, and data analysis processes. Sequence generation and allocation determination were completed using Microsoft Excel (Microsoft, Redmond, WA, USA).
Study overview
The study’s flow diagram is displayed in Figure 1. Before official enrollment, individuals reviewed and signed the written informed consent form and underwent health history screening. Participants completed five sessions over the span of 7–11 days, all occurring at the same time of day. Session 1: body size (height, weight) was determined. Body composition (body fat percentage [BF%]) assessments were completed within 30 days of enrollment. Dynamic strength measures using an isokinetic peak torque test (PTT) and power measures using a countermovement jump (CMJ) were determined. Familiarization processes to all equipment and procedures were embedded within this session. Session 2: 3–7 days later (4.68 ± 1.47 days separation, determined by participant availability), participants completed a questionnaire (pre-fatigue protocol [FP]) to assess baseline sensations of soreness to gauge subjective recovery throughout the investigation. Participants then completed a pressure–pain threshold (PPT) test to assess muscular sensitivity, followed by an isokinetic FP designed to exhaust the lower extremity. A post-FP questionnaire (0-h pre-cream/rest [C/R]) was completed, followed by C/R procedures, in which CG and PG participants applied CBD and placebo creams, respectively, using a standardized process, and NG participants engaged in a sitting rest period that matched in duration to cream application processes. The session concluded with another questionnaire (0-h post-C/R), PPT, and CMJ. Sessions 2–5 were separated by 24-h each. Sessions 3 and 4: participants completed a questionnaire (24-h and 48-h, respectively), PPT, CMJ, and C/R procedures. After C/R, participants completed another questionnaire (24-h post-C/R and 48-h post-C/R, respectively), PPT, and CMJ. Session 5: participants completed a questionnaire (72-h) and then repeated the research procedures of the first session, with the exclusion of anthropometric testing. This session concluded with a questionnaire (post-study), in which CG and NG participants answered cream-specific questions. A detailed visual overview of the experiment’s primary measures is depicted in Supplementary Material S1.
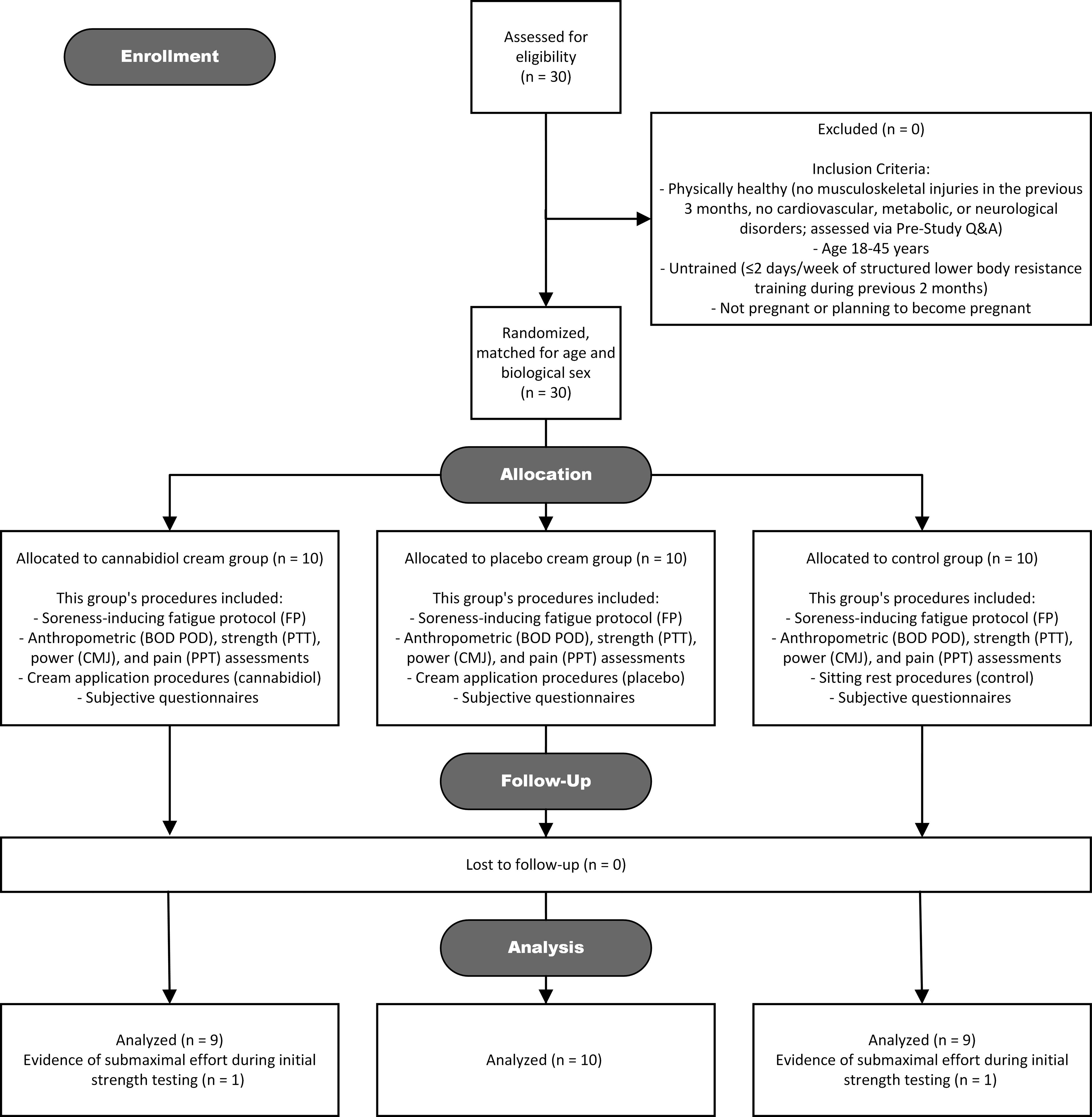
Consort flow diagram. CMJ, countermovement jump; FP, fatigue protocol; PPT, pressure–pain threshold; PTT, peak torque test.
Participants verbally confirmed abstinence from structured physical activity, external recovery interventions, and nonprescription drugs to mitigate external influences on muscular recovery. Each session, participants were encouraged to communicate abnormal discomfort and side effects to the investigator for documentation. Participants also indicated whether they had experienced redness or irritation in their daily questionnaire. If necessary, the study’s medical supervisor would be contacted for evaluation. No participants at any point during or after the study reported adverse effects and warranted medical evaluation.
Participants
Healthy individuals (no musculoskeletal injuries in the previous 3 months; no cardiovascular, metabolic, or neurological disorders) aged 18–45 years and untrained in lower-body resistance training were recruited. For the purposes of this study, individuals were considered “untrained” if they had not participated in lower-body resistance training 2 days per week during the previous two months. Self-reported cannabinoid, nicotine, and nonprescription drug users who refused to undergo a 1-week period of abstinence before beginning the study were excluded. Based on the U.S. Food and Drug Administration (FDA)’s recommendations, 24 those who self-reported to be pregnant or planned on becoming pregnant were excluded. Habitual diets were encouraged to be maintained.
Thirty untrained participants (15 men, 15 women; age: 23.1 ± 2.6 years; body mass: 73.2 ± 12.9 kg; BF%: 22.7 ± 7.8%) volunteered to participate in the study. There were no withdrawals from any of the participants. Two participants were cut in a post hoc overview owing to evidence that they did not provide a maximal effort during initial strength testing. Thus, 15 men and 13 women (n = 28; mean ± standard deviation age: 23.3 ± 2.5 years; body mass: 73.1 ± 12.9 kg; BF%: 22.2 ± 7.8%) were included for data analysis (Table 1).
Descriptive Characteristics for All Participants (n = 28)
All data are reported as mean ± SD. Baseline characteristics were similar across all groups (all p ≥ 0.535).
CG, cannabidiol group; NG, control group; PG, placebo group.
Ethical approval
All protocols were approved by the University of Kentucky’s Institutional Review Board (IRB) on August 8, 2022 (#80177) and registered with ClinicalTrials.gov (NCT06320327). All individuals provided IRB-approved written informed consent, where they were informed of the procedures, risks, and benefits of participating in the investigation. After informed consent, physical readiness screening took place to ensure individuals had no physical or cognitive abnormalities.
Anthropometric measures
Height and body mass were recorded using a stadiometer and digital platform scale, respectively. BF% was determined using air displacement plethysmography (BOD POD Body Composition System, COSMED, Rome, Italy) 25 within 30 days of enrolling.
Electronic questionnaires
Digital questionnaires used Research Electronic Data Capture software. Questions used a 0–10 Likert scale (0 indicating maximum muscle impairments or no condition effect; 10 indicating no muscle impairments or maximum condition effect). To minimize confusion, each Likert scale was accompanied with text to describe what numbers on each scale indicate. The full list of questions used throughout the entirety of the study is cataloged in Supplementary Material S2.
Pressure-Pain Threshold
PPT is the minimum quantity of pressure that induces pain. 26 A digital pressure algometer (Pain Test FPX 50, Wagner Instruments, Greenwich, CT, USA) equipped with a 1-cm2 rubber tip was used. When pressed against a surface, a force reading appears on its digital screen. Participants were marked in four locations (quadriceps: midline of the anterior leg, midway between the anterior superior iliac spine and superior border of the patella; hamstrings: midline of the posterior leg, midway between the ischial tuberosity and popliteal fossa). Testing began with the quadriceps and was followed by the hamstrings (dominant leg and then nondominant leg). For quadriceps, participants sat with the knee at 90° flexion. For hamstrings, participants laid prone with the knee extended. Force was manually applied to each site gradually (5–7 N·sec−1). When discomfort was felt, participants said “stop,” and the value was recorded. A single researcher who conducted all PPT tests extensively practiced proper technique to improve reliability. Three trials were performed for each site, and the mean value was used for analysis. This process is visually outlined in Supplementary Material S1.
Warm-up
All participants completed a standardized warm-up before testing to standardize exercise readiness (walking at self-selected pace [3 min]; bodyweight squats [2 sets, 10 repetitions]).
Countermovement Jump
CMJ correlates well with lower-body muscular performance 27 and has been used to estimate force-generating capacity after damaging exercise. 28 Portable force plates (ForceDecks Dual Force Plate System, Vald Performance, Newstead, Queensland, Australia) were sampled at 1000 Hz. Data were collected within the device’s software on a tablet (Apple iPad, 9th generation, Cupertino, CA, USA). During each jump, participants were instructed to place their hands on their hips while standing evenly on the force plates. On the investigator’s cue, participants squatted down and proceeded to jump as high as possible. Squat depth was visually monitored. A single jump concluded when the participant landed back onto the plates. Maximal effort for each jump was verbally encouraged. Jump height (JH) and peak power (PP) were automatically calculated. Three trials were performed, separated by 30 sec. The maximum values were used for analysis. This process is visually outlined in Supplementary Material S1.
Isokinetic torque protocols
PTT and FP used an isokinetic dynamometer (Biodex System 4 Pro dynamometer, Biodex Medical Systems, Shirley, NY, USA), set up in accordance with the manufacturer’s guidelines. Chair position was recorded to maintain consistency throughout the study. Both tests were performed unilaterally at a speed of 60 deg·sec−1, beginning with the dominant leg and concluding with the nondominant leg. Each participant was verbally encouraged to deliver maximal effort for every repetition of both tests. Both protocols are outlined in Supplementary Material S1.
PTT included maximal concentric knee extension (CON EXT), concentric knee flexion (CON FLX), eccentric knee flexion (ECC FLX), and eccentric knee extension (ECC EXT) efforts. Testing consisted of five repetitions for each movement type, separated by 2 min of rest. Testing was preceded by a familiarization period to ensure participants understood the actions required.
FP included repeated, maximal CON EXT and ECC FLX efforts and maximal ECC EXT and CON FLX efforts. Testing consisted of 5 sets of 10 repetitions for each movement type, separated by 30 sec of rest, with 2 min of rest allowed for switching legs during the protocol. Borg’s Rating of Perceived Exertion (RPE) scale was used after every set to evaluate subjective perception of effort. 29
Cream application and sitting rest
The CBD cream used in the present study was Myaderm Advanced RX10 Fast Acting Relief Cream (Myaderm, Englewood, CO, USA), a commercially available topical CBD product, which contained 11.27% CBD (0% tetrahydrocannabinol [THC]; Batch #1191) and 10.29% CBD (0% THC; Batch #1222). Both batches were laboratory tested by an independent party (SC Labs, Santa Cruz, CA, USA). This product was chosen because of its extensive third-party laboratory testing and null-THC content. Currently, Epidiolex, a formulation used to treat seizures associated with Lennox–Gastaut syndrome, is the only CBD product approved by the FDA. 30 Therefore, the CBD cream used in this study was not FDA-approved. The manufacturer’s guidelines were used for administered dose (two pumps from the built-in dispensing actuator for each leg, equating to ∼100 mg per leg). The placebo cream used was Gold Bond Diabetics’ Dry Skin Relief Lotion (Gold Bond Diabetics, Chattanooga, TN, USA). This cream was selected following a blinded assessment by individuals independent to the study to best match physical characteristics to the CBD cream.
An independent investigator with no involvement in the recruitment, data collection, or data analysis processes was responsible for cream allocation (weight-matched), supplied in coded plastic containers, which were not decoded until all testing had concluded. All containers were stored in a cool, dry area. Cream was applied to both legs during Sessions 2–4, totaling three time points in which cream was applied. Detailed application procedures to ensure rigorous control of these processes are outlined in Table 2.
Cream Application Process for CBD and Placebo Groups
Note that subjects within the control group engaged in sitting rest to match in duration to these processes (3 min).
CBD, cannabidiol.
Instead of applying cream, NG participants engaged in sitting rest for 3 min. This procedure consisted of the participant sitting in a relaxed position on one of the laboratory chairs. This duration was chosen so that it matched the duration of the cream application processes.
Statistical analyses
Unilateral measures were assessed for a statistically significant difference between limbs (p < 0.05) using a paired t-test. There were no significant differences between left and right legs throughout all PPT tests for every participant; therefore, interlimb PPT values were averaged, and this value was used for analysis. Two-way mixed analysis of variance (ANOVA) tests (group × time) were used to assess interaction and main effects for RPE, CMJ, and questionnaires regarding soreness. To determine local (quadriceps) or systemic (quadriceps and hamstrings) effects, three-way mixed ANOVA tests (group × muscle × time) were used to assess interaction and main effects for PPT, torque, and questionnaires regarding cream effect. Mauchly’s test of sphericity was used to determine violations of sphericity (p < 0.05). If violated, a Greenhouse–Geisser correction was applied. Pairwise comparisons were used for post hoc analyses. The level of statistical significance for all interaction effects and main effects was set at p < 0.05, and a Bonferroni adjustment was made to declare significance for simple interactions and effects. Effect sizes, as expressed as partial eta squared (η2), were classified as small (0.01), medium (0.06), or large (0.14). 31 All statistical analyses were completed using SPSS (IBM, Armonk, NY, USA).
Results
Rating of Perceived Exertion
For RPE during FP, there were no significant interactions (group × set; all p ≥ 0.560) for any leg or movement. RPE increased throughout each set of the FP, for each leg and all movements (all set effects p < 0.001), indicating all groups perceived the increase in difficulty throughout the FP similarly (Table 3).
Results of Two-Way Mixed ANOVA for Ratings of Perceived Exertion Reported During Each Set of the Fatigue Protocol (n = 28)
Bold text donates statistical significance (p < 0.05).
ANOVA, analysis of variance; CON EXT, concentric knee extension; CON FLX, concentric knee flexion; ECC EXT, eccentric knee extension; ECC FLX, eccentric knee flexion; L, left leg; R, right leg; F, F-statistic.
Muscle soreness questionnaires
For overall body soreness, there were no significant interactions (group × time; p = 0.976) or significant main effect for group (p = 0.531). There was a main effect for time (p < 0.001; Fig. 2). Post hoc pairwise comparison revealed the rating of overall soreness during pre-FP was significantly higher (i.e., less sore) than 0-h pre-C/R, 24 h, 48 h (all p < 0.001), and 72 h (p = 0.007). By 72 h, overall soreness was reported to be significantly less when compared with 0-h post-FP (p < 0.001).

Ratings of overall soreness level over time. Data are presented as mean ± SD for the mean rating (0–10). ** Denotes there was a significantly lower rating when compared with pre-FP for the main effect of time (p < 0.01). *** Denotes there was a significantly lower rating when compared with pre-FP for the main effect of time (p < 0.001). Denotes there was a significantly higher rating when compared with 0 h (pre-C/R; p < 0.001). C/R, cream/rest; SD, standard deviation.
For soreness level (magnitude), soreness pattern (frequency), and tightness, there were no significant interactions (group × time; all p ≥ 0.082; Fig. 3). There were main effects for group for questions regarding quadriceps soreness level, pattern (both p = 0.031), and tightness (p = 0.024; Fig. 3). Post hoc pairwise comparison revealed nonsignificant differences in soreness between PG and CG (p = 0.061), but PG experienced less soreness frequency than CG (p = 0.044) and less tightness than NG (p = 0.028). There were main effects for time (all p < 0.001) for soreness level, pattern, and tightness (Fig. 3).
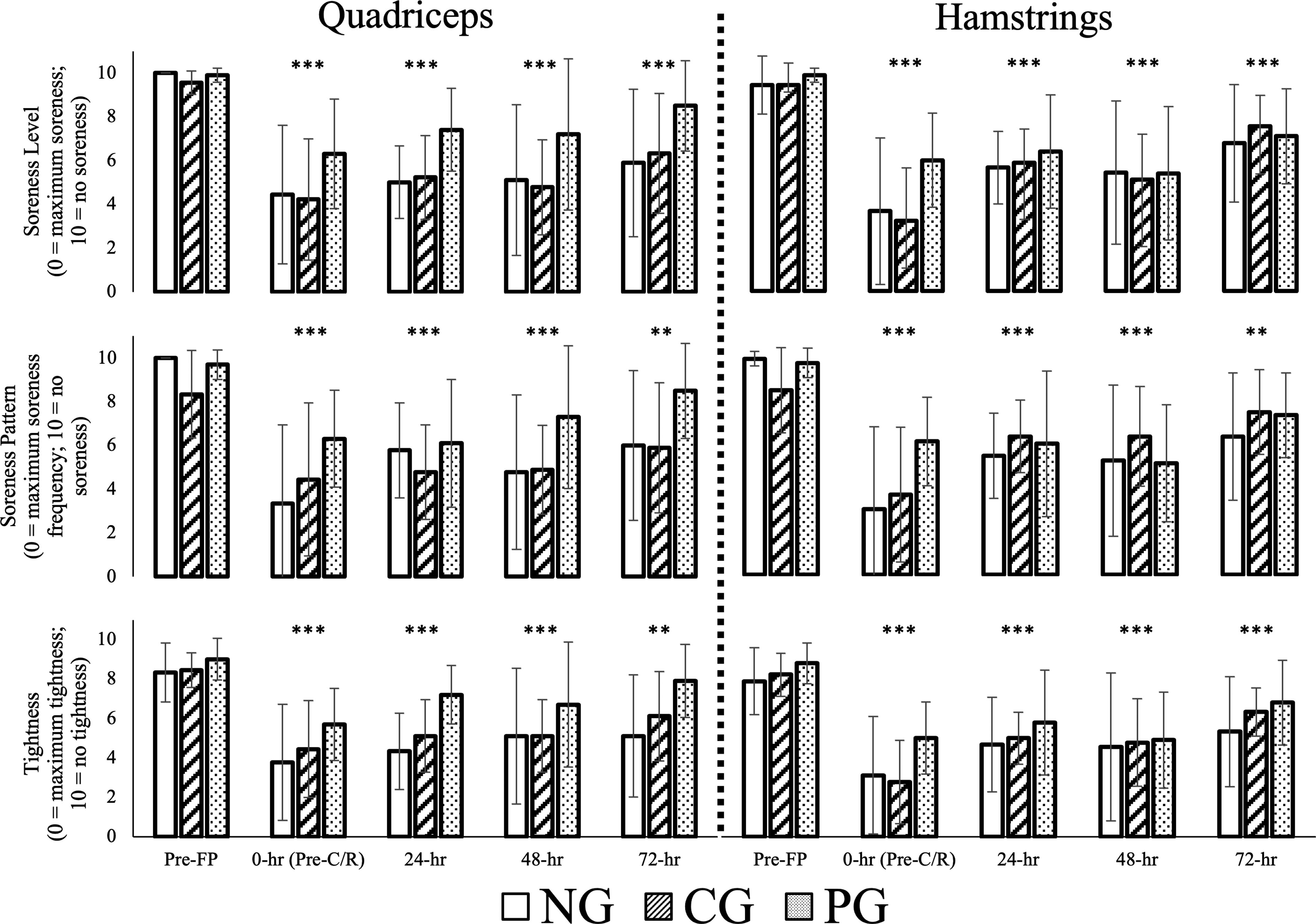
Ratings of soreness level (top), soreness pattern (middle), and tightness (bottom) over time. Data are presented as mean ± SD for the mean rating (0–10). ** Denotes there was a significantly lower rating when compared with pre-FP for the main effect of time (p < 0.01). *** Denotes there was a significantly lower rating when compared with pre-FP for the main effect of time (p < 0.001).
Pressure-Pain Threshold
For PPT, there were no significant interactions (group × muscle × time; all p ≥ 0.177) or significant main effects for group (p = 0.303) or time (p = 0.065; Fig. 4). There was a main effect for muscle (p = 0.008). Post hoc pairwise comparison revealed PPT of hamstrings was significantly less than quadriceps (p = 0.008) throughout all testing.
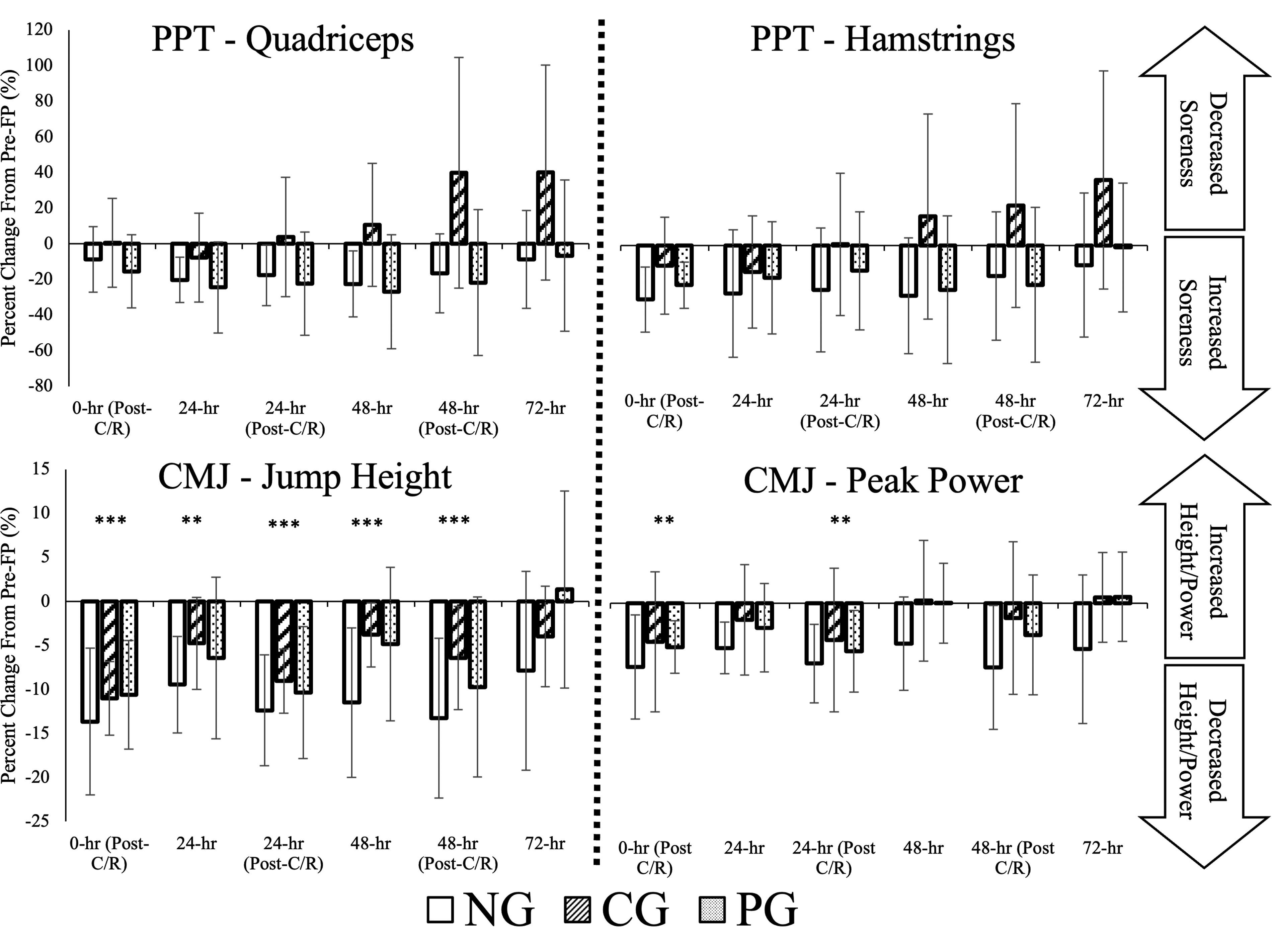
Average pressure–pain threshold (PPT) between legs for quadriceps (top left) and hamstrings (top right), and countermovement jump height (JH; bottom left) and peak power (PP; bottom right). Data are displayed as percent change from baseline values recording during Session 2. Data are presented as mean ± SD for the mean percent change (%). ** Denotes there was a significantly lower value when compared with pre-FP for the main effect of time (p < 0.01). *** Denotes there was a significantly lower value when compared with pre-FP for the main effect of time (p < 0.001).
Countermovement Jump
For JH, there were no significant interactions (group × time; p = 0.289) or significant main effect for group (p = 0.412; Fig. 4). There was a main effect for time (p < 0.001). Post hoc pairwise comparison revealed JH was significantly greater at pre-FP than 0-h post-C/R (p < 0.001), 24 h (p = 0.010), 24-h post-C/R (p < 0.001), 48 h (p < 0.001), and 48-h post-C/R (p < 0.001).
For PP, there were no significant interactions (group × time; p = 0.490) or significant main effects for group (p = 0.829; Fig. 4). There was a main effect for time (p < 0.001). Post hoc pairwise comparison revealed PP was significantly greater at pre-FP than 0-h post-C/R (p = 0.008) and 24-h post-C/R (p = 0.008).
Peak Torque
For PTT, there were no significant interactions (group × muscle × time; all p ≥ 0.072) or significant main effects for group (all p ≥ 0.505) or time (all p ≥ 0.632) for CON or ECC torque of right or left legs (Supplementary Material S3).
Cream/Rest effect
For questionnaire answers regarding C/R effect, there was one significant interaction (group × time; p = 0.045), in which the effect of cream on the quadriceps was perceived to be greater in PG when compared with rest in NG at 24 h (p = 0.014; Table 4). There was a main effect for muscle (p < 0.001). Post hoc pairwise comparison revealed C/R effect was greater in quadriceps than hamstrings (p < 0.001). There was no main effect for group (p = 0.276) or time (p = 0.051).
Ratings of Cream or Rest Effect Over Time
Data are presented as mean ± SD for the mean rating (0–10). 0 = No effect on soreness. 10 = Substantially significant decrease in soreness.
Denotes there was a significant group × time interaction (p < 0.05).
C/R, cream/rest.
Post-study questionnaire
At the conclusion of the study, 55.6% of CG participants (n = 5) and 40% of PG participants (n = 4) guessed their respective creams accurately (Supplementary Material S4).
Discussion
The purpose of this study was to investigate the effects of topical CBD on muscle soreness and voluntary contractile performance after exercise. Contrary to our hypotheses, CBD did not significantly decrease perceived muscle soreness (no localized effect) or improve recovery of muscular power.
DOMS is dependent on exercise intensity, so it was paramount that the FP was perceived similarly across groups. According to RPE, it appears all groups perceived the difficulty of the protocol similarly, independent of group and preliminary strength capabilities. Immediately after FP, body soreness ratings for all groups were significantly worsened. Therefore, within the limitations of the study, we assume all groups were similarly fatigued.
The topical CBD used within this study had no effect on CMJ or torque assessments following FP. These data agree with Crossland et al.’s experiment, in which CBD had no impact on vertical jump after a muscle damage protocol. 13 The findings also agree with previous experiments in which strength measures in the CBD conditions were not significantly different from placebo conditions.12,13,22 However, these findings conflict with those of Isenmann et al., 17 in which CBD resulted in increased squat performance 72 h after muscle-damaging exercise. These contrasting results could be due to differences in training statuses or CBD administration. Although long-term CBD supplementation may aid in power retention compared with placebo, 16 the allocated dose and type of topical CBD cream used in this study do not appear to restore dynamic muscle function.
CBD cream appeared to have no consistent effect on self-perceived soreness. Although group differences did exist in favor of PG’s quadriceps recovery, this is likely due to the variability in perceptions of soreness rather than the cream itself. These results contradict those of Hatchett et al., 14 in which subjective soreness ratings were significantly lower after an exercise protocol in a CBD group when compared with placebo and control groups, and Xu et al., 23 in which CBD oil reduced pain associated with peripheral neuropathy.
All groups believed the effect of C/R was greater in the quadriceps despite its failure to improve recovery. In CG/PG, all participants who believed they received CBD voted the cream had a long-term effect on the decrease in quadriceps soreness (n = 11), and all participants who believed they had received the placebo voted the cream did not have a long-term effect on the decrease in quadriceps soreness (n = 8): 91.6% of online posts about CBD claim it possesses physical or mental benefits 32 ; therefore, it is possible that the idea of CBD influenced perception of the cream’s effects in cream-receiving groups.
Although pressure algometry is used in research settings, 33 it possesses limitations. The sites tested, although adapted from previous methodologies,3,34 were at the respective midpoints of the muscles. Localization of tenderness in the distal portion of the muscle is typically observed after EIMD because of the oblique arrangement of muscle fibers and increased concentration of pain receptors near the myotendinous junction. 35 Testing multiple sites could have provided a more comprehensive understanding of muscular sensitivity. However, the purpose of this test was not to establish definitive thresholds of pain but to evaluate trends in muscular sensitivity over time. These data revealed CBD did not significantly change PPT at the testing sites assessed within this study.
This pilot investigation has several limitations that must be acknowledged. First, future investigations should use larger sample sizes, as this pilot study had low statistical power, likely compromising the ability to detect three-way interactions. Readers should not interpret the data from the present study as definitive findings owing to the limited sample size; rather, this pilot study should be used to guide future investigations related to CBD and exercise recovery.
Second, the dose of the CBD used in the present study was likely too low to elicit a noticeable effect. In line with previous topical CBD studies, the manufacturer’s recommended dose was used for the present experiment.22,23 This trial would have greatly benefited from conducting blood analyses for cannabinoid concentration to provide insight on the absorption of CBD. A credible blood concentration has been reported to be ∼100 nM of free CBD21. Furthermore, topical CBD product peak concentrations may not be achieved until after 7–10 days of use. 36 Future topical CBD studies should consider deviating from simply following the manufacturer’s recommendations unless dosing is supported by peer-reviewed evidence. Investigators should instead conduct approved and registered pre-clinical trials to determine adequate doses and frequencies of application to elicit optimal free CBD concentration; this should be followed by the implementation of these product-specific findings to a clinical trial to determine the designated dose of CBD’s effects on the measures of interest.
Third, over-the-counter topical CBD product formulations should be carefully assessed. Typical drug delivery through the skin begins with the substance partitioning into the stratum corneum and undergoing further diffusion, proceeded by additional partitioning into viable epidermis layers. 37 Topical CBD permeation is limited to its formulation and the biochemical properties of the epidermis. Previous experiments conducted on human skin samples assessed several topical CBD formulations and their cutaneous delivery and distribution abilities. 38 Colloidal systems were more effective than other commercial products in targeting CBD delivery. Notably, a CBD formulation in propylene glycol, an ingredient within the cream used in the present study, appeared to be less effective. Thus, the presence of effective permeabilizers within CBD formulations should be investigated before implementing into future trials.
Lastly, muscle soreness is a physiological response to novel exercise. It is possible that the stimulus used within the current trial exceeded any potential analgesic effect that the CBD cream might have elicited. Conducting blood analyses to determine biomarkers of muscle damage (e.g., creatine kinase, myoglobin) would have provided insight on the biological impacts of the FP. Furthermore, unstructured physical activity, sleep, and diet were not controlled. These variables could have also impacted recovery rates after the FP.
Despite its limitations, this study has noteworthy strengths. First, the study’s design was rigorous, as it was a randomized, double-blinded, placebo-controlled experiment. Although a study design consisting of three groups with a smaller sample size limits statistical power, its design enables the differentiation between the pharmacological effects of CBD, the psychological effects of believing one has received the CBD, and the natural physiological progression after novel exercise without any treatment. Second, to the authors’ knowledge, this is the first study to examine the effect of a commercially available CBD cream formulation on muscle soreness and performance. Lastly, the variety of measures used to assess strength and muscular pain were both novel to the area of CBD research and provided a holistic understanding of the physical impacts of a fatiguing exercise protocol.
Conclusions
The present study did not discover any significant impacts of CBD cream use for muscle recovery. For individuals seeking to attenuate muscle soreness and improve performance, the current dose of this topical CBD product may not be an effective treatment.
Footnotes
Acknowledgment
The authors would like to acknowledge the individuals who participated in the study.
Authors’ Contributions
J.T.P.: Conceptualization (lead); writing—original draft (lead); writing—reviewing and editing (equal); investigation (lead); methodology (equal); project administration (lead); formal analysis (lead). M.G.A.: Conceptualization (supporting); writing—reviewing and editing (equal); methodology (equal). L.M.B.: Conceptualization (supporting); reviewing and editing (equal); methodology (equal). S.A.B.: Conceptualization (supporting); reviewing and editing (equal); methodology (equal); project administration (supporting); supervision (lead); formal analysis (supporting).
Author Disclosure Statement
There were no competing interests, personal finance interests, funding, or employment associated with the completion of this study.
Funding Statement
No funding was received or used to complete this study.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.