
Abstract
Objectives:
Cannabidiol (CBD) is rising in popularity, including as a potential medicinal product. Yet data on use of commercial CBD for medicinal or health reasons in adolescents are lacking. In this study we aim to detail characteristics of adolescents given commercial CBD for health reasons (health CBD [hCBD]) and to investigate predictors of use.
Materials and Methods:
The Adolescent Brain Cognitive Development (ABCD) Study is a population-based cohort study following U.S. healthy, community-based adolescents annually, with data from 2018 to 2022 (11- to 15-year-olds; N=11,189). Participants and caregivers completed questionnaires, including whether adolescents were given CBD with parent or doctor's permission. Participants reported past-month pain, attention problems, externalizing symptoms, internalizing symptoms, and total mental health problems. Caregivers reported youth sociodemographics, sleep problems, whether the youth had mental health treatment or sought medical treatment, and rules about recreational cannabis use. We describe youth given hCBD, and run generalized estimating equations predicting odd ratios (ORs) and 95% confidence intervals of adolescents given hCBD by mental health, physical health, or sociodemographics of factors.
Results:
Of the 11,189 participants across up to three waves of data, 48% were female. Mean age across waves was 12.8 years old (SD=1). In total, 307 (2.8%) were given hCBD. Common administration methods were oil (42%), topical (31%), and edibles (29%). Increased hCBD odds were associated with being older (OR=1.32 [1.17–1.49]), White (relative to Black, OR=05.97 [2.81–12.65] or Hispanic, OR=1.82 [1.17–2.82]), parents with some college (relative to no high school diploma, OR=3.55 [1.09–11.6]), internalizing symptoms (OR=1.81 [1.13–2.91]), mental health treatment (OR=1.76 [1.3–2.38]), pain (OR=1.38 [1.09–1.76]), medical treatment (OR=1.39 [1.08–1.79]), and sleep problems (OR=1.69 [1.27–2.25]). Rules against recreational cannabis decreased odds of hCBD (OR=1.75 [1.30–2.36]).
Conclusions:
Findings indicate some healthy adolescents are given hCBD, and predictors of use include mental and physical health concerns, being White, older, and parents with some college education. Providers should ask if their youth patients are being given CBD medicinally, and transparently discuss potential benefits, consequences, and unknowns of CBD.
Introduction
Cannabidiol (CBD) is suggested as a potential treatment for numerous physical and mental health conditions in youth, including epilepsy, 1 anxiety, 2 and pain relief, 3 among others,4,5 although evidence for medicinal use is currently limited.5–8 Even so, the popularity of CBD is rising, in part owing to recommendations and advertising on social media platforms.9,10 Perhaps, accordingly, parents appear to increasingly seek to administer nonpharmaceutical-grade CBD products to generally healthy youth for medicinal reasons. 7
CBD is a cannabinoid within the cannabis plant and, with the U.S. 2018 Farm Bill, was legalized in all 50 states through hemp products (defined as containing <0.3% tetrahydrocannabinol [THC]); it is also legal in other countries around the world, in some in conjunction with recreational cannabis and in others with similar limits to THC content. 11 One plant-derived CBD medication is approved by the Food and Drug Administration (FDA) to treat rare forms of epilepsy (Epidiolex). 12 Beyond this, CBD is available across the United States in stores, dispensaries, online retailers, and even coffee shops. However, commercial CBD products are shown to be inaccurately labeled,13–15 contain THC levels exceeding the legal limit for hemp products,13,14,16,17 and to provide subtherapeutic CBD levels for those seeking relief from epilepsy (youth through adults). 17 Despite these issues, cases of parents giving their child CBD medicinally are documented, leaving clinicians uncertain how to best guide these families.7,18
There is much to be learned about commercial CBD taken for health reasons (health CBD [hCBD]) in youth. Knowledge about the characteristics (e.g., sociodemographics, physical and mental health) of otherwise healthy youth who may turn to hCBD is sparse. Furthermore, investigations that do consider commercial CBD use in youth are limited to only one or two diagnoses (e.g., Refs.5,19), rather than the myriad of conditions CBD is reported to treat. In this study we detail the sociodemographic, socioenvironmental, physical health, and mental health characteristics of 11- to 15-year-olds given hCBD in a community-based, generally healthy cohort. We then investigate longitudinally whether factors suggested as potential reasons for medicinal use (e.g., pain, sleep problems, mental health) predict which youth are given hCBD.
Materials and Methods
Data from the large, longitudinal, and diverse Adolescent Brain Cognitive Development (ABCD) Study were leveraged, which included N=11,878 participants enrolled at 9–10 years old with annual follow-up visits. Participants were recruited at baseline through epidemiologically guided probability-based sampling of schools at ages 9–10 years, 20 aiming to match U.S. Census data. Participants attended annual study session visits with their caregiver and completed self-report questionnaires, with cognitive battery and neuroimaging completed every other year; full details regarding the baseline protocol are published elsewhere.21–27 Exclusion criteria at baseline included magnetic resonance imaging contraindications, living outside the recruitment catchment area, not falling within the correct age range, being born <28 weeks or low birth weight (<1200 g), birth complications resulting in hospitalization for >1 month, having a major neurological disorder (e.g., epilepsy or history of seizures), diagnosis of schizophrenia, moderate/severe autism spectrum disorder, intellectual disability, or alcohol/substance use disorder.
For this study, all participants with data at Waves 2, 3, or 4 were included. Mean age across waves was 12.8 years old (SD=1 year) and 48% were female. Data collection occurred between September 1, 2016 (start of Wave 0) and January 15, 2022. In total, 11,189 participants were included with data from Waves 2 (n=10,853), 3 (n=10,174), or 4 (n=4648) (data release 5.0, https://nda.nih.gov/study.html?id=2147). Beginning at Wave 2, participants and their parents were asked whether the youth were given CBD products for medicinal or health reasons (hCBD). All aspects of the study protocol were approved by the University of California, San Diego institutional review board. Participants and their caregivers provided written informed assent/consent.
Measures
Sociodemographics
Caregivers reported sociodemographic characteristics of youth at baseline, including sex assigned at birth (hereafter referred to as sex), race, ethnicity, family household income, and highest level of parental education. 21
Recreational substance use
Youth were asked to report on all substance use since their last visit (approximately 1 year). 24 They were asked specifically about cannabis puffing, recreational cannabis use, recreational CBD use, and method of cannabis use. Cannabis use and recreational CBD use were coded as two separate binary variables.
Medicinal CBD use
Participants and their caregivers were separately queried on hCBD. Caregivers were asked, “Has your son/daughter used any CBD (or cannabidiol) products with your or your doctor's permission, such as Epidiolex or other over the counter CBD product, in the past year?.” Responses included, “yes,” “no,” or “I don't know.” Endorsement of CBD product use would prompt an additional question on method of hCBD use (e.g., oil, tincture). In addition, youth and their caregivers were asked the same question, but if use occurred within the past 24 h. Either the youth or caregiver endorsing use (past year or 24 h) was coded as hCBD use.
Toxicological testing
Subsamples of participants were selected by hair testing because of financial restrictions, with the majority of participants (>90%) selected owing to elevated risk for substance use onset (e.g., reporting peers use, family history of dependence, disclosing personal substance use) and the remainder randomly selected after receiving a low score on a risk algorithm (see Refs.28,29). A total of 111 hCBD participants had cannabinoid hair testing. Hair samples 3.9 cm in length were collected to provide a 3-month window of substance use detection and sent to Psychemedics (Culver City, CA) for washing to remove external contamination and tested by liquid chromatography tandem mass spectrometry for 11-nor-9-carboxy-THC (THCCOOH) and gas chromatography tandem mass spectrometry for THC and CBD.
Cannabis rules
Caregivers reported whether they had set rules regarding cannabis use for their children (never allowed, allowed at home with permission, allowed at home whenever, allowed wherever, they had no rules, or they had not made rules yet).30–33 Responses were reduced to a binary variable of never allowed versus any other response.
Geographic location
Region of study participation based on study site where data were collected. Coding is consistent with the U.S. Census Bureau (Midwest, Northeast, South, West).
Mental health
Caregivers reported whether youth had mental health treatment since their last study visit (approximately past year), coded as yes or no. Youth reported on their own mental health using the Brief Problem Monitor—Youth (BPM-Y). 34 Subscales of attention, externalizing, internalizing, and total problems were calculated, and t-scores were utilized. A binary variable of above/below the clinical threshold (t≥65) was included in analyses.
Physical health
Medical history was queried annually by parent report. 21 Here, whether youth participants had seen a medical provider for any reason other than an annual checkup was reported (1=yes; 0=no). Youth self-reported whether they had felt any pain within the past 30 days (1=yes; 0=no 35 ). Sleep was reported by caregivers on the Sleep Disturbances Scale for Children; 36 a total score of >39 indicates sleep problems.
Statistical analyses
R version 4.1.037 via RStudio 38 was used for all statistical analyses, with p<0.05 set as the threshold for significance.
Descriptives
Sociodemographics were examined for the whole cohort, with chi-squares assessing differences by hCBD status. Chi-squares were followed up with post hoc tests using pairwise proportion tests; these results are given in the Supplement Data.
Frequencies of other variables of interest are described within the hCBD group. Within these frequencies, given minimal reporting of hCBD use at multiple visits within the same participant, each instance of hCBD reporting is treated as an independent case (e.g., if reporting at Y2 and Y4 follow-up, data on both instances are reported separately).
Generalized estimating equations
A generalized estimating equation (GEE) was run using geepack 39 to examine longitudinal physical, mental health, and other predictors of initiation of hCBD by Wave 3 in youth with hCBD relative to youth without hCBD. Youth hCBD use was treated as a binary outcome. Observations were clustered on participant to account for the repeated measures design. Quasi Information Criteria was used to test various correlational structures to determine optimal model fit; 40 based on this approach, an exchangeable correlational structure was chosen and interpreted for the GEE model. Results were considered significant if the Wald statistic (Wχ 2 ) was at the p<0.05 level. In addition, standardized odds ratio (OR) and 95% confidence intervals were derived and included for interpretation with rescaling applied to continuous predictors. 41 For ORs <1, the inverse of the OR were calculated to aid in interpretation.
The GEE model contained sociodemographic factors (i.e., age, sex, race/ethnicity, parental education, and household income), physical health (i.e., sleep problems, medical history, pain), mental health (i.e., mental health treatment, and BPM-Y subscales: attention, internalizing, externalizing, and total problems, separately), and socioenvironmental factors (i.e., regions within the United States and parental rules regarding cannabis use).
Data from Wave 4 were excluded from GEE modeling given that fewer than half of participants' data were available in the present data release and it is therefore not representative of the full ABCD cohort. In addition, data from Waves 0 and 1 were excluded as hCBD was not queried. Given this, the total number of those with hCBD use included in the GEE was n=242 by Year 3. In addition, Asian-identifying youth were removed to improve GEE model fit because of no hCBD initiation within this group.
Missingness
Missingness for GEE was addressed utilizing multivariate imputation by chained equations in the MICE package, 42 with all missing variables imputed following 30 imputation iterations. Missing data ranged from 0% (hCBD use) to 11% (BPM-Y Total Problems; missingness by variable is listed in Supplementary Table S1). Several participants who did not have sex at birth as male or female or who did not report their current age were excluded from analyses. In addition, if participants declined to answer (e.g., for mental health treatment) or reported not knowing a response (e.g., for medical treatment), their responses were excluded from the model, for a total n=10,916.
Results
Patterns of use in youth given hCBD
A total of 307 participants were given hCBD (2.8% of participants) according to parent and/or youth report, including those with hCBD at multiple waves, 120 (1.1% of the full cohort) participants at Wave 2, 162 (1.6%) at Wave 3, and 107 (2.3%) at Wave 4 had hCBD reported, for a sum total of 389 cases of hCBD across waves. Fewer than 10 reported hCBD at all three waves, and 65 reported hCBD at two waves. Across all instances of hCBD reported regardless of year, 344 (88%) instances were reported solely by the parents, 13 solely by the youth, and 32 by both the parents and the youth.
Across all time points in those with hCBD (n=389), 32 cases reported recreational cannabis use (a puff or more); fewer than 10 youth reported recreational CBD use or reported both recreational CBD and other cannabis use.
Sociodemographic differences
Relative to the ABCD cohort overall, participants with hCBD tended to have higher levels of parental education (χ24=33.3, p<0.001) and were more likely to be of White race/ethnicity (χ24=55.8, p<0.001); no differences were seen in household income or sex of the youth (see Table 1 and Supplementary Table S2 for full results).
Sociodemographics in Health Cannabidiol Use
Bold text indicates p < 0.05.
hCBD=medicinal CBD use as reported by the youth, their caregiver, or both; consistent with NIH reporting requirements for Adolescent Brain Cognitive Development Study data, any cells that would indicate <10 participants (or <3% of hCBD or 0.01% of no CBD) are obscured.
CBD, cannabidiol; GED, general educational development; hCBD, health CBD; HS, high school.
Method of hCBD administration
The most common methods for CBD administration to youth were oil/tincture, topical/transdermal, and edible/capsule/pill. The majority (92%) used only one method of administration, whereas 6% used two methods, and the remaining participants either used three methods or did not know what method was used (Table 2).
Method of Cannabidiol Administration as Reported by Youth and/or Parents (n=307)
FDA, Food and Drug Administration.
Toxicological testing
A subset (n=111) of hCBD participants completed hair toxicological testing for cannabinoids. Thirteen of 111 (12%) participants' hair samples were positive for CBD; 25 (23%) had results indicating THC exposure (positive for THC or THCCOOH). Fewer than 10 were positive for both CBD and THC or THCCOOH.
Socioenvironmental factors
Seventy-one percent of caregivers of youth with hCBD reported their child was not allowed to use recreational cannabis at all, compared with 82% of no hCBD. The largest regional proportion in those with hCBD was 41% of youth who reside in the West (Table 3).
Regional Distribution of Health Cannabidiol Use
hCBD % within region indicates the percentage of participants who have ever been given hCBD within each region.
Mental health
On the BPM-Y, 26% hCBD youth reported clinically elevated attention problems (relative to 18% no hCBD), 12% reported internalizing symptoms (8% no hCBD), 5% reported externalizing symptoms (3% no hCBD), and 19% reported total mental health problems of any kind (9% no hCBD). Thirty-one percent reported having received mental health treatment since their last study visit, compared with 14% in the no hCBD group.
Physical health
Of the 307 hCBD users, 208 (68%) parents reported that their child had been seen by a medical professional for reasons other than a regular check-up since the youth's last study visit (∼1 year). Of those, most (n=106) reported “Other” as the medical condition for which their child was seen, and no participants reported being seen for seizures. Forty-seven percent of hCBD youth reported experiencing pain within the last month, with a mean pain score of 4.3 of 10 (SD=1.8); only 35% of non-hCBD participants reported past-month pain (mean=4; SD=1.7). Forty-two percent of youth with hCBD reported having above-threshold levels of sleep problems.
GEE model predicting hCBD
Full GEE model details are given in Supplementary Table S3. When combining all predictors (Fig. 1), higher odds of hCBD use was associated with being older (OR=1.32 [1.17–1.49], p<0.001), being White (relative to Black, OR=5.97 [2.81–12.65], p<0.001, OR inversed for interpretation; and Hispanic, OR=1.82 [1.17–2.82], p=0.01, OR inversed for interpretation), having parents with some college education (relative to <high school diploma, OR=3.55 [1.09–11.6], p=0.04), reporting clinical levels of internalizing symptoms (OR=1.81 [1.13–2.91], p=0.01), having had mental health treatment in the past year (OR=1.76 [1.3–2.38], p<0.001), having pain in the past month (OR=1.38 [1.09–1.76], p=0.008), seeking medical treatment in the past year (OR=1.39 [1.08–1.79], p=0.01), and having sleep problems (OR=1.69 [1.27–2.25], p<0.001). Parents without firm rules against cannabis use was associated with increased odds of hCBD (OR=1.75 [1.30–2.36], p<0.001; OR inversed for interpretation).
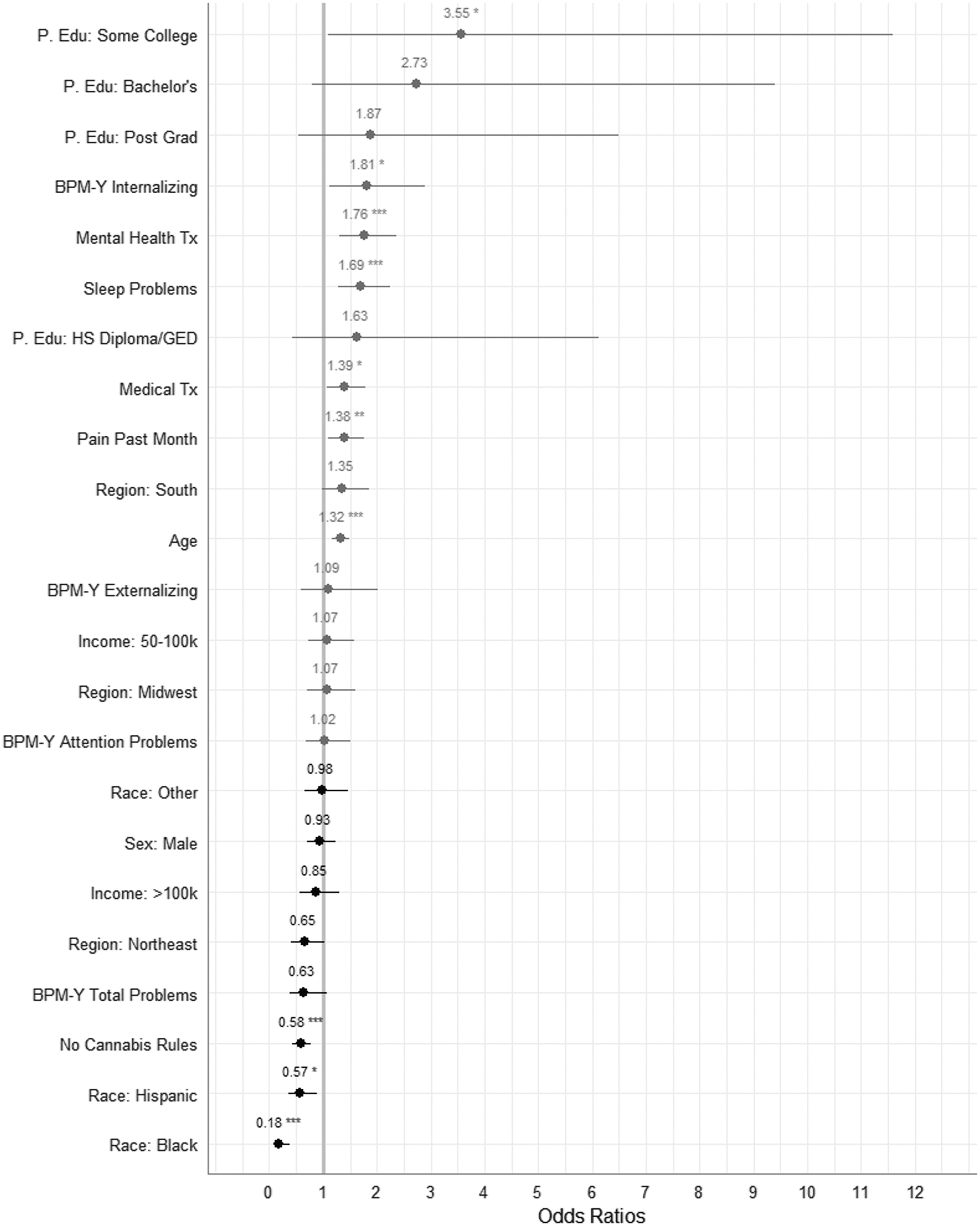
Full GEE model predicting OR of medicinal cannabidiol use. Blue represents increased odds and red represents decreased odds. OR is displayed with a 95% confidence interval with asterisk indicating statistical significance. GEEs were run with Wave 2 and Wave 3 data. BPM-Y, Brief Problem Monitor—Youth report; Edu, education; GEE, generalized estimating equation; OR, odds ratios; P., parental; Tx, treatment.
Discussion
Novel data presented here indicate 2.8% of 11- to 15-year-olds from a large longitudinal, diverse, and generally healthy cohort were reported to use hCBD. The present analyses detail indicators of who may be more likely to use hCBD in youth: having parents with some college education, being White, being 13–14 years (vs. 11–12 years), receiving mental health treatment and internalizing symptoms, having sleep problems, past-month pain, and seeking medical treatment. Youth with parents who do not allow recreational cannabis use were less likely to use hCBD. Finally, youth with hCBD use appeared more likely to use cannabis (with or without CBD) recreationally, as ∼10% of those with hCBD reported past-year recreational use (vs. 1% of the ABCD cohort overall at similar ages 43 ) and 23% of those with toxicologically tested hair were positive for THC or its metabolite.
Findings here mirror sociodemographic characteristics and mental and physical health reasons associated with hCBD in adults.44–47 It may be that parents who give their child hCBD use it themselves for similar or other health reasons. Parents were also the primary reporters of hCBD use in their children, rather than children reporting their use. This may be owing to (1) parents reporting on a longer timeframe of potential use (both past 24 h and past year), whereas youth only reported on past 24 h, or (2) that youth are unaware of what medications they are taking. Of interest, those with hCBD use do not appear to be wholly eschewing traditional treatment, as the majority also sought professional medical or mental health treatment. Indeed, the majority of those with hCBD use only reported use at one wave of assessment, suggesting its use as a temporary or perhaps adjunctive treatment. More explicit investigation into reasons for and frequency of hCBD in youth is needed.
No reported cases of hCBD used pharmaceutical-grade CBD (i.e., Epidiolex). As this is a generally healthy, community-based cohort, epilepsy was exclusionary at baseline and no participants reported past-year seizure treatment. Participants were primarily given hCBD through oil/tincture, a topical/transdermal method, or through an edible or pill form. Of importance, in addition to general concerns around dosing of commercial hCBD products,17,48 efficacy of topical methods may be limited because of lack of skin absorption without the required enhancing agents in CBD products. 49 Furthermore, large proportions of adults believe CBD is proven effective for a range of conditions and regulated by the FDA, 47 despite the limited authorization of Epidiolex for two forms of epilepsy and limited established efficacy of CBD for other conditions.5–8 Thus, patient education regarding the lack of regulation and standardization of commercial CBD is important.
Cannabinoid content, including both CBD and THC, is a concern when products are purchased from retail shops.13,15,16,50 Accordingly, here hCBD participants' toxicological results indicated both active THC and CBD use. As only hCBD was queried, it may be that some participants were knowingly given CBD products that contained THC. However, given broader commercial CBD data,14,50 it is likely that some youth were intending to only use CBD but the product also contained THC.
Clinically, clinicians may consider incorporating inquiring about cannabis use broadly and CBD specifically with their patients. CBD is not without side effects and adverse events, including drowsiness, fatigue, and gastrointestinal distress in youth. 51 With pharmaceutical-grade CBD (Epidiolex), contraindications include liver functioning; thus, liver functioning should also be monitored in any CBD use. On balance, there are real, known positive effects of CBD such as in its treatment of rare forms of epilepsy using Epidiolex. 1 Providers should transparently discuss the nuance, potential benefits, and consequences, and, particularly, the unknowns of CBD with their patients.
More broadly, public health campaigns are needed to educate communities regarding the nascent status of CBD research in youth. Additional prevention efforts should target youth with hCBD exposure to mitigate risk of transitioning into recreational cannabis use. This is particularly important given the potential for increasing vulnerabilities to cannabis during adolescence, 52 and considering the present findings of toxicological results indicating THC exposure and higher rates of self-reported recreational cannabis use in those with hCBD use. Government agencies such as the U.S. FDA should regulate commercial CBD products and improve communication efforts to detail the presently limited evidence of efficacy of CBD, particularly among those at greatest odds of using hCBD with their children (e.g., based on health, sociodemographic, and other characteristics identified here). Research funding is needed to assess the clinical efficacy of CBD across diagnoses, establish thresholds for dosing, and to disseminate this information—whether efficacy is supported or not—to the public.
Limitations
Analyses were limited to factors that were queried within the ABCD Study. Other reasons for hCBD exist beyond those considered here, and reason for hCBD was not asked. Furthermore, it is not known whether a medical provider suggested or was consulted in the use of hCBD, nor is dosage or frequency of hCBD known. Parents and youth differed in reporting timeframes for youth hCBD use. Directionality of hCBD results and outcomes were not assessed. The GEE model was limited to only two waves of data; findings require replication. Here sociodemographic differences were investigated in isolation, although intersectionality of identities is important and should be considered in future work.
Conclusions
Much remains to be studied in hCBD in healthy youth, both to validate clinical efficacy and to detail when and how CBD may be beneficial medicinally, whether in commercial or pharmaceutical-grade CBD. Notwithstanding, this is the first known investigation to document (1) prevalence estimates, (2) methods of administration, and (3) general predictors of commercial hCBD use in young community-based adolescents. Of importance, data here document that ∼3% of young adolescents have used hCBD. Predictors of use reflect those found in adults: mental and physical health concerns and certain sociodemographic characteristics.
With uncertain cannabinoid content, including cases here documenting THC exposure and higher rates of recreational cannabis use in those with hCBD use, and other reports of inaccurately labeled commercial CBD, patients should be warned to exercise caution in product use and greater governmental regulation of products should be considered. As the literature on hCBD in minors is sparse, public policy and public health efforts would be bolstered by concerted efforts within the pediatric research community to better understand hCBD use in youth, from birth through adolescence.
Footnotes
Acknowledgements
Authors would like to express their gratitude for the time and commitment of ABCD families, and to Samuel Wade for his contributions to this paper. A listing of participating sites and a complete listing of the study investigators can be found at https://abcdstudy.org/consortium_members/. ABCD consortium investigators designed and implemented the study and/or provided data but did not necessarily participate in the analysis or writing of this report. This article reflects the views of the authors and may not reflect the opinions or views of the National Institutes of Health or Adolescent Brain Cognitive Development consortium investigators. N.E.W. takes responsibility for the integrity of the work as a whole, from inception to published article. The ABCD data used in this report came from the ABCD 5.0 data release (![]() ).
).
Authors' Contributions
Conception and design: N.E.W., T.T.N.-L., A.L.W., S.F.T. Acquisition, analysis, or interpretation of data: N.E.W., T.T.N.-L., A.L.W., R.M.S., S.F.T. Drafting of the article: N.E.W. Critical revision for the article for important intellectual content: N.E.W., T.T.N.-L., A.L.W., R.M.S., S.F.T. Statistical analysis: N.E.W., T.T.N.-L., A.L.W., R.M.S. Obtaining funding: N.E.W., S.F.T. Administrative, technical, or material support: N.E.W.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
N.E.W. was supported by National Institute on Drug Abuse (DA050779). This work was also supported by T32 AA013525 (PI: Riley/Spadoni to A.L.W.). Data used in the preparation of this article were obtained from the Adolescent Brain Cognitive DevelopmentSM (ABCD) Study (https://abcdstudy.org), held in the NIMH Data Archive (NDA). This is a multisite, longitudinal study designed to recruit more than 10,000 children aged 9–10 years and follow them over 10 years into early adulthood. The ABCD Study® is supported by the National Institutes of Health and additional federal partners under award numbers U01DA041048, U01DA050989, U01DA051016, U01DA041022, U01DA051018, U01DA051037, U01DA050987, U01DA041174, U01DA041106, U01DA041117, U01DA041028, U01DA041134, U01DA050988, U01DA051039, U01DA041156, U01DA041025, U01DA041120, U01DA051038, U01DA041148, U01DA041093, U01DA041089, U24DA041123, U24DA041147. A full list of supporters is available at ![]() .
.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.