
Abstract
This pilot longitudinal study using measures from parents and teachers evaluated the effects of flexible doses of atomoxetine (ATX) on neuropsychological and functional outcomes in 21 children with attention-deficit/hyperactivity disorder (ADHD) (mean age, 8.0 ± 1.3 years; inattentive subtype, 71.4%; combined subtype, 28.6%). Among 16 children completing 6 months of ATX treatment, neuropsychological function measured by the NEPSY instrument found significant improvement from baseline in the memory and learning domain (p = 0.01); this change was also seen in an age- and sex-matched healthy control group (p = 0.011). The patient group showed significant improvement on the Test of Everyday Attention (TEA-Ch) and parent and teacher versions of the Behavior Rating Inventory of Executive Function (BRIEF), which assess attentional and executive processes, respectively. Functional improvement was also observed on the Weiss Functional Impairment Rating Scale–Parent Report (WFIRS-P) and parent and teacher versions of the ADHD Rating Scale (ADHDRS-IV), and the investigator-rated Clinical Global Impressions–Severity (CGI-S) scale evidenced reductions in ADHD symptoms. These findings suggest that potential benefits of ATX treatment may extend beyond reduction of core ADHD symptoms to amelioration of some neuropsychological and functional deficits.
Introduction
Pharmacotherapy is a mainstay in the management of ADHD (American Academy of Pediatrics 2001; Swanson et al. 2008). The effectiveness of medications for ADHD has historically been assessed using changes in core behavioral symptom checklists and rating scales (Klassen et al. 2004). Because of the focus on symptom reduction in clinical trials, limited research has been conducted to evaluate the effects of treatment with ADHD medications on other important indicators of outcome, such as neuropsychological function, health-related quality of life, and ability to function in daily life, despite evidence that children with ADHD frequently experience a wide range of deficits and problems (Matza et al. 2004). Studies that evaluate changes in neuropsychological functioning with ADHD medication may also contribute to a better understanding of the neural processes underlying any such changes.
Atomoxetine hydrochloride (ATX) is a nonstimulant, highly selective inhibitor of the noradrenergic transporter that is approved for the treatment of ADHD in children aged 6 years and older, adolescents, and adults (Corman et al. 2004). Clinical trials show that ATX is effective and well tolerated in reducing ADHD symptoms in children, adolescents, and adults (Michelson et al. 2001; Spencer et al. 2002; Michelson et al. 2003; Kelsey et al. 2004; Weiss et al. 2005; Kratochvil et al. 2007). Moreover, some clinical trials have suggested that in addition to treating core ADHD symptoms, ATX improves psychosocial aspects of health-related quality of life in children and adolescents with ADHD (Matza et al. 2004; Prasad et al. 2007).
ADHD is associated with substantial impairments that manifest across multiple settings. School is an important component of each child's and adolescent's life, and, consequently, effective medications should improve ADHD manifestations in the classroom. Toward this end, teacher ratings are an essential measure in assessing the efficacy of any ADHD medication. Atomoxetine was shown in a 7-week acute trial to significantly reduce the total score on the ADHD Rating Scale-IV (ADHDRS-IV)–Teacher Version (vs. placebo), as well as on the inattentive and hyperactive/impulsive subscales of this instrument (Weiss et al. 2005). The present pilot study is the first investigation of ATX that includes baseline and 6-month ratings obtained by direct interviews of teachers.
Executive function, one aspect of neuropsychological function, can be broadly defined as higher-order abilities that allow for strategic planning, cognitive flexibility, self-regulation, and goal-directed behaviors in novel and complex situations (Weyandt 2005). Deficits in executive function are evident in many children and adolescents with ADHD (Shallice et al. 2002; Willcutt et al. 2005; Seidman 2006). A pilot study in 9 children suggested that ATX treatment for 10 weeks improved executive function as measured by the motor screening and rapid visual information processing subtests of the Cambridge Neuropsychological Test Automated Battery (Barton et al. 2005). Moreover, two identical randomized, placebo-controlled studies in adults with ADHD showed that treatment with ATX for 10 weeks improved executive function in the Stroop color word test (Faraone et al. 2005). Because cognition may be related to academic performance and functional outcomes of patients, further research is warranted on the impact of ATX on broader outcome variables such as neuropsychological functioning. It is still unknown whether ATX has an effect on global neuropsychological functioning in children with ADHD. Therefore, we sought to determine whether ATX improves attention and executive function, as well as other cognitive domains (e.g., language, memory, or perception), by using an extended battery of tests.
The present single-center pilot study was designed to provide a longitudinal assessment of outcome over 6 months in children treated with flexible doses of ATX and to generate hypotheses for future research. Neuropsychological function was targeted concurrently with core ADHD symptoms and functional impairments. In addition, measures from both parents and teachers were obtained regarding executive and clinical function outcomes. As recommended in previous studies (Goldberg et al. 2007), a control group, matched individually by age and sex with the AHDH group of children, was included to evaluate longitudinal changes in neuropsychological function and exclude possible practice effects on tests of cognition. Consequently, the effect of ATX was to be considered significant only if the improvement in children with ADHD was greater than that observed in the control group. We hypothesized that the change in the NEPSY and the Behavior Rating Inventory of Executive Function (BRIEF) after 6 months of ATX would be greater in the ADHD cohort than in the control group. The Test of Everyday Attention (TEA-Ch) was not administered to controls because it bypasses practice effects.
Methods
Patients
At the initial screening visit, male and female outpatients aged 6–10.5 years underwent a medical examination. The diagnosis of ADHD was determined using DSM-IV-TR eligibility criteria for ADHD and confirmed by a child psychiatrist (M.M.) using the Kiddie Schedule for Affective Disorders and Schizophrenia for School Aged Children–Present and Lifetime Version: Behavioral Disorders Supplement (K-SADS-PL: Behavioral). Eligible children had a symptom severity threshold ≥1.5 standard deviations (SD) above the age and sex norms for total score on the parent version of the ADHDRS-IV and had normal intelligence (a score ≥80 on the two-subtest version of the Wechsler Abbreviated Scale of Intelligence [WASI]). Both treatment-naïve children and those who had received previous medication(s) for ADHD were eligible.
Patients were excluded from the study if they had a current or past history of bipolar disorder, psychosis, autism, Asperger syndrome, pervasive developmental disorder, or seizure disorder (other than febrile seizures), if they needed psychotropic medication in addition to the study drug, or if they had any medical conditions that would contradict the use of ATX. Children who were home schooled were ineligible, given the inclusion of teacher ratings.
Control group
An individual age- and sex-matched control group without any psychiatric disorders was also recruited for this study. Eligible control subjects were of normal intelligence as defined above and did not have a diagnosis of a psychiatric disorder or a medically significant disorder. Confirmation of the lack of a present or previous diagnosis of a behavioral disorder was made at the initial visit using the K-SADS-PL: Behavioral.
Study design
This study was conducted in accordance with ethical principles of the Declaration of Helsinki and in compliance with good clinical practices and all applicable regulations. The protocol and statement of informed consent were approved by the local university ethical review board before any patient was enrolled. This study had an open-label design and was conducted at a single study center during one school year starting in September, 2005, to obtain longitudinal teacher ratings in addition to parent ratings and investigator assessments. Children were treated with flexible daily doses of ATX up to a maximum of 1.4 mg/kg or 100 mg (whichever was less) for 6 months, consistent with the approved dosing regimen in Canada. Before starting ATX, children discontinued any psychotropic medications or health food supplements with central nervous system activity. Clinic visits were scheduled at baseline (day 0) and at 2, 3, and 5 weeks and 2, 4, and 6 months.
Assessments
A neuropsychological assessment was completed by a Ph.D. student in clinical neuropsychology (supervised by N.R.). Patients were tested individually in a quiet room. The NEPSY is a validated neuropsychological instrument consisting of 27 subtests that evaluate neuropsychological status of children aged 3–12 years across five domains (attention/executive functions, language, visual–spatial processing, sensorimotor, and memory and learning) (Korkman et al. 2001; Schmitt and Wodrich 2004). Most of the subtests have reported mean internal consistency reliability coefficients of 0.70–0.90, with interrater reliabilities of 0.97–0.99 (Korkman et al. 1998). The TEA-Ch, consisting of tests assessing sustained attention, selective attention, and attention control in children, was also administered (Manly et al. 2001). The TEA-Ch, which consists of two parallel versions, is constructed to be administered sequentially for test–retest; because there was not the same concern about practice effect as there was with the NEPSY, it was not administered to controls. Test–retest reliability coefficients of 0.64–0.92 have been reported for the nine subtests in a study cohort ranging in age from 6 to 16 years (reliability coefficients of 0.57–0.85 after adjusting for age) (Manly et al. 2001). The TEA-Ch has been validated with respect to attentional deficits unique to ADHD; children with ADHD performed significantly worse than a clinical control group on three of five subtests assessing sustained attention (Heaton et al. 2001).
Neuropsychological function was also assessed by teacher- and parent-completed ratings using the BRIEF. This rating scale consists of 86 items and provides a global composite score of executive function and subscale scores for behavioral regulation and metacognition (Gioia et al. 2002). The BRIEF has been validated in comparison with similar behavioral rating systems, and reported reliability coefficients for internal consistency range from 0.80 to 0.98, with a test–retest reliability for a parent rating subsample of 0.76–0.85, and that for a teacher rating subsample of 0.83–0.92 (Gioia et al. 2000). Each of these neuropsychological instruments was administered at baseline and after 6 months of ATX treatment to the children with ADHD.
The NEPSY and the BRIEF–Parent version were also completed at baseline and 6 months later for subjects in the control group. No other neuropsychological instruments were evaluated in the control cohort.
ADHD symptoms were assessed at baseline and after 2 and 6 months of treatment using the ADHDRS-IV: Parent and Teacher versions: Investigator Administered and Scored (Faries et al. 2001). This 18-item scale consists of one item for each of the 18 symptoms contained in the DSM-IV-TR diagnosis of ADHD. Each item is scored on a 4-point scale from 0 (none/never) to 3 (very often) by the investigator while interviewing the parent or teacher. The total score is determined from the sum of the scores for each individual item, and in addition, subscores for inattention and hyperactivity/impulsivity are determined from the sum of the scores for odd-numbered and even-numbered items, respectively. The Clinical Global Impressions–Severity (CGI-S) scale was used to assess the global severity of ADHD on a 7-point scale from 1 (normal) to 7 (severely affected) (National Institute of Mental Health 1985). The CGI-S was completed by the study psychiatrist at each clinic visit.
Daily functioning was evaluated using the Weiss Functional Impairment Rating Scale (WFIRS-P). At baseline and after 5 weeks and 2 and 6 months of ATX, parents used the WFIRS-P to rate 50 items measuring their child's function across six domains: Family, learning and school, life skills, child's self-concept, social activities, and risky activities. Each item was scored on a 4-point Likert scale with 0 = never or not at all, 1 = sometimes or somewhat, 2 = often or much, and 3 = very often or very much (Weiss et al. 2007).
Safety
All treatment-emergent adverse events that occurred during the course of this study were recorded on case report forms, and their relation to the study drug was evaluated by the investigator. Laboratory testing was not required during this study.
Statistical analysis
The primary analysis measured the change from baseline to 6 months in each of the five domain scores on the NEPSY. All patients who completed the 6-month assessment and who remained on ATX treatment and their matched controls were included in the primary analysis (n = 16). If more than one raw score was missing, then the combined score was also considered to be missing. However, if only a single item was missing, then the mean score for all other items was used to compute the total score. Secondary objective measures included changes from baseline in the scores on all other instruments and comparisons with the control group for the NEPSY and the BRIEF–Parent version at the 6-month end point. Analyses of changes from baseline to end point in ADHD symptoms included all enrolled patients, whereas only subjects who completed 6 months of treatment were included in the other objective measures. The distribution of each objective measure was checked for normality and homogeneous variance assumptions, if applicable. Changes from baseline to 6 months in the objective measures and comparisons with the control group used the paired t-test when these assumptions were met, and if not, the Wilcoxon signed rank test was used. All statistical tests were evaluated based on a two-sided significance level of 0.05. Raw scores and/or corresponding standard scores were used in change analyses as appropriate. All patients who received at least one dose of study drug were included in the safety analyses.
A post hoc analysis was completed that compared the ADHD patients with the control subjects on the NEPSY using an analysis of covariance (ANCOVA) model for each domain adjusted for baseline, age, sex, and intelligence quotient (IQ). A similar post hoc analysis was not performed for BRIEF, because the control group had scores within 1 SD below the norm (i.e., better function), and consequently had little room for improvement. Between-group comparisons for BRIEF were made using standardized T scores, which take norms into account.
Results
Patient disposition and demographics
Twenty-one children with ADHD were enrolled, and 16 (76.2%) completed the study. Three children (14.3%) discontinued owing to lack of efficacy, and 2 children discontinued owing to adverse events. The control group consisted of 20 age- and sex-matched children, all of whom had completed assessments at baseline and 6 months. One child with ADHD who dropped out early was not provided with a control.
The ADHD cohort included 16 boys (76.2%) and 5 girls (23.8%), and had a mean age of 8.0 years (Table 1). All but 1 was Caucasian. Most of the children had been diagnosed with ADHD, inattentive type (n = 15; 71.4%), with the others diagnosed with ADHD, combined type, and most (n = 13; 61.9%) had been treated previously with ADHD medications. The full-scale IQ on the WASI averaged 98.2 in the ADHD cohort. The control group was well matched demographically to the ADHD cohort but had a higher mean IQ (118.5).
n = 20; the remaining patient had a Wechsler Intelligence Scale for Children full-scale IQ of 116.
Abbreviations: ADHD = attention-deficit/hyperactivity disorder; SD = standard deviation; WASI = Wechsler Abbreviated Scale of Intelligence; IQ = intelligence quotient.
Neuropsychological function
Changes from baseline in the five functional domains of the NEPSY are shown in Table 2 for the 16 ADHD children who completed the 6-month study and were still receiving ATX. The mean score on the Memory and Learning domain of the NEPSY increased from 93.6 at baseline to 104.1 after 6 months of ATX treatment (mean change = 10.6; p = 0.01). At 6 months, all other domains were numerically higher than at baseline, but none of the changes was statistically significant. The control group also showed significant changes in the Memory and Learning domain, from 115.2 at baseline to 125.7 at 6 months (change = 10.5; p = 0.011) (Table 2). Planned analysis of comparisons between groups revealed that the changes from baseline in each domain of the NEPSY in the ADHD cohort did not differ significantly from those in the control group. The post hoc analysis using an ANCOVA model with adjustments for baseline values, age, sex, and IQ also did not find significant differences between the changes in the ADHD and the control group scores.
The normative mean for each domain is 100 ( ±values are the mean (±standard deviation). The p values were determined using Wilcoxon signed rank test for comparison between end point and baseline and paired t-test for comparison of change between groups.
Abbreviation: ADHD = Attention-deficit/hyperactivity disorder.
On the TEA-Ch, scores for “Sky Search Time Per Target” (raw score mean change = −1.8; p < 0.001) and “Sky Search Attention Score” (raw score mean change = −1.6; p = 0.004), which are measures of selective attention, “Creature Counting Accuracy” (raw score mean change = 1.1; p = 0.021) and “Creature Counting Time Scores” (raw score mean change = −2.4; p = 0.048), which are measures of attentional control, and “Walk, Don't Walk” (raw score mean change = 3.1; p = 0.024), a measure of sustained attention, improved significantly from baseline after 6 months of ATX treatment. Only “Sky Search Targets Found” and “Score!,” measures of selective and sustained attention, respectively, were not significantly improved after ATX. In addition, scores on five of seven domains moved toward age-scaled norm means after 6 months of ATX. The age-scaled scores on the TEA-Ch at baseline and after 6 months of ATX treatment are shown in Fig. 1.
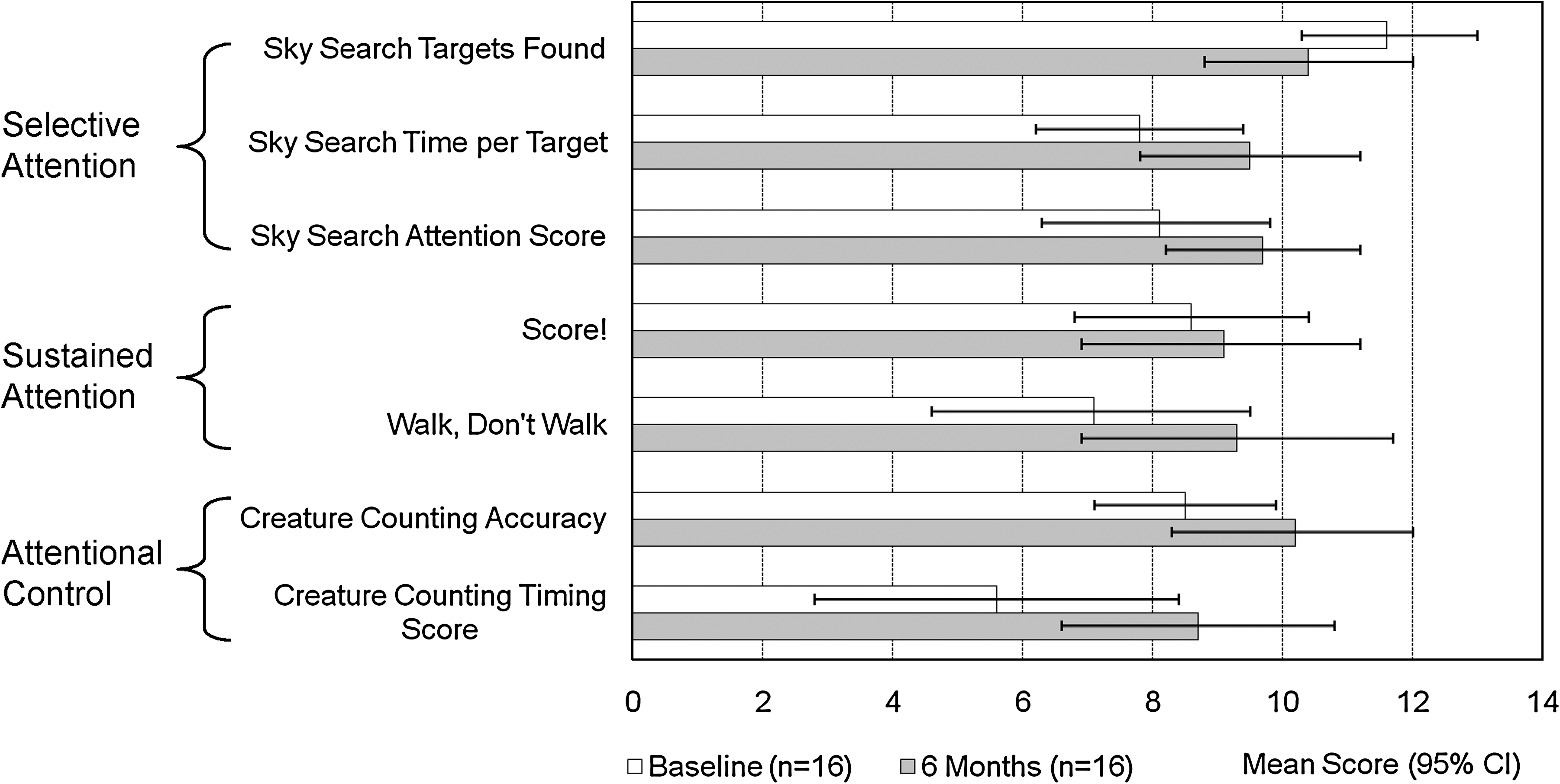
Age-scaled scores on Test of Everyday Attention (TEA-Ch) at baseline and after 6 months of atomoxetine treatment. All scores moved toward age-scaled means (norm mean = 10, standard deviation = 3). Changes from baseline to 6 months were significant for “Sky Search Time per Target” (baseline = 7.8, mean change = 1.7), “Sky Search Attention Score” (baseline = 8.1, mean change = 1.6), and “Creature Counting Accuracy” (baseline = 8.5, mean change = 1.7) (p < 0.05). CI = Confidence Interval.
At baseline, the mean parent T-score ratings of the ADHD cohort on the global composite and individual subscales of BRIEF were each more than 1 SD above the norm. Treatment with ATX was associated with a significant improvement in the global composite T score on the BRIEF–Parent version, from 71.5 at baseline to 58.8 at 6 months (mean change = −12.8, p < 0.001) (Table 3). The behavioral regulation and metacognition subscales and each of the individual clinical scales contributing to the composite and subscale scores were also significantly improved after 6 months of ATX therapy. The ratings by teachers on the BRIEF also revealed significant improvement in the global composite T score, from a mean of 65.7 at baseline to 60.1 after 6 months of ATX (mean change = −5.6, p = 0.047) (Table 3). The metacognition subscale and four of the five individual clinical scales contributing to it were also significantly improved after 6 months of ATX therapy.
The normative mean for each domain is 50 (±10). All values are mean (± standard deviation).
p < 0.05, † p < 0.01, § p < 0.001 using the Wilcoxon signed rank test.
Abbreviations: ADHD = Attention-deficit/hyperactivity disorder; BRIEF = Behavior Rating Inventory of Executive Function.
The BRIEF–Parent version was also completed for the control group. In contrast to the patient group, the baseline scores of the control group were much lower, with all mean T scores for global, subscales, and individual scales within 1.1 SD below the norm and changes from baseline to six months were not significant. The improvements seen in the ADHD cohort after 6 months of ATX therapy were significantly greater than the changes reported for children in the control group for the global executive composite score (mean change, −12.8 vs. 2.8, p < 0.001), behavioral regulation subscale (−9.8 vs. 1.6 p < 0.001) and metacognition subscale (−12.9 vs. 3.4, p < 0.001), as well as for the individual scales.
Attention-deficit/hyperactivity disorder symptoms
Treatment with ATX was associated with progressive improvement over the 6-month study period as shown on both the parent and teacher versions of the ADHDRS-IV (Fig. 2). At baseline, the score on the parent version of the ADHDRS-IV was significantly higher than that on the teacher version (35.9 vs. 28.0; p < 0.05), suggesting greater symptom impairment perceived by the parents at home than by the teachers in the school setting. However, ADHD symptoms were reduced in severity when assessed after 2 months of ATX treatment on both parent and teacher assessments, with further continuing improvement at the final assessment at 6 months (all p < 0.05). By the end of the 6-month study, mean scores on the ADHDRS-IV–Parent and–Teacher versions did not differ significantly.
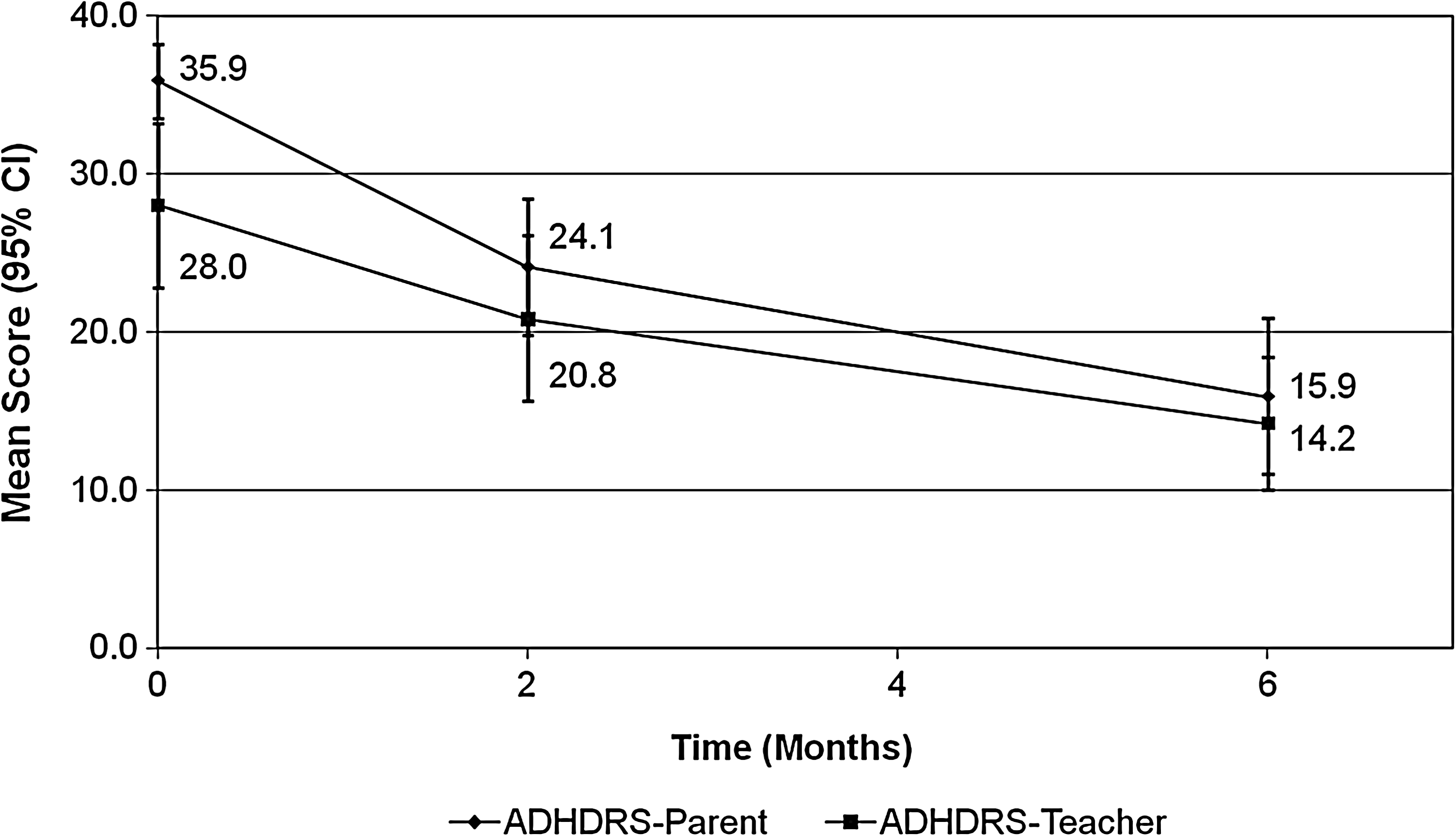
Change in total score of Attention-Deficit/Hyperactivity Disorder Rating Scale–Parent and–Teacher versions (ADHDRS-IV) after 2 and 6 months of atomoxetine treatment. Scores differed significantly at baseline between the Parent and Teacher versions (p < 0.05) and for all within-group comparisons at 2 and 6 months versus baseline (p < 0.05). CI = Confidence Interval.
Consistent with the ADHDRS-IV results, the global severity of ADHD symptoms improved progressively during the course of ATX treatment when assessed by the physician investigator using the CGI-S (Fig. 3). The mean CGI-S score at baseline was 4.9, indicating that the children, on average, were markedly affected by their ADHD symptoms. Significant reduction in CGI-S score was first evident at the clinic visit at week 3, and then the CGI-S score declined, progressively reaching 2.7 at 6 months (p < 0.001).
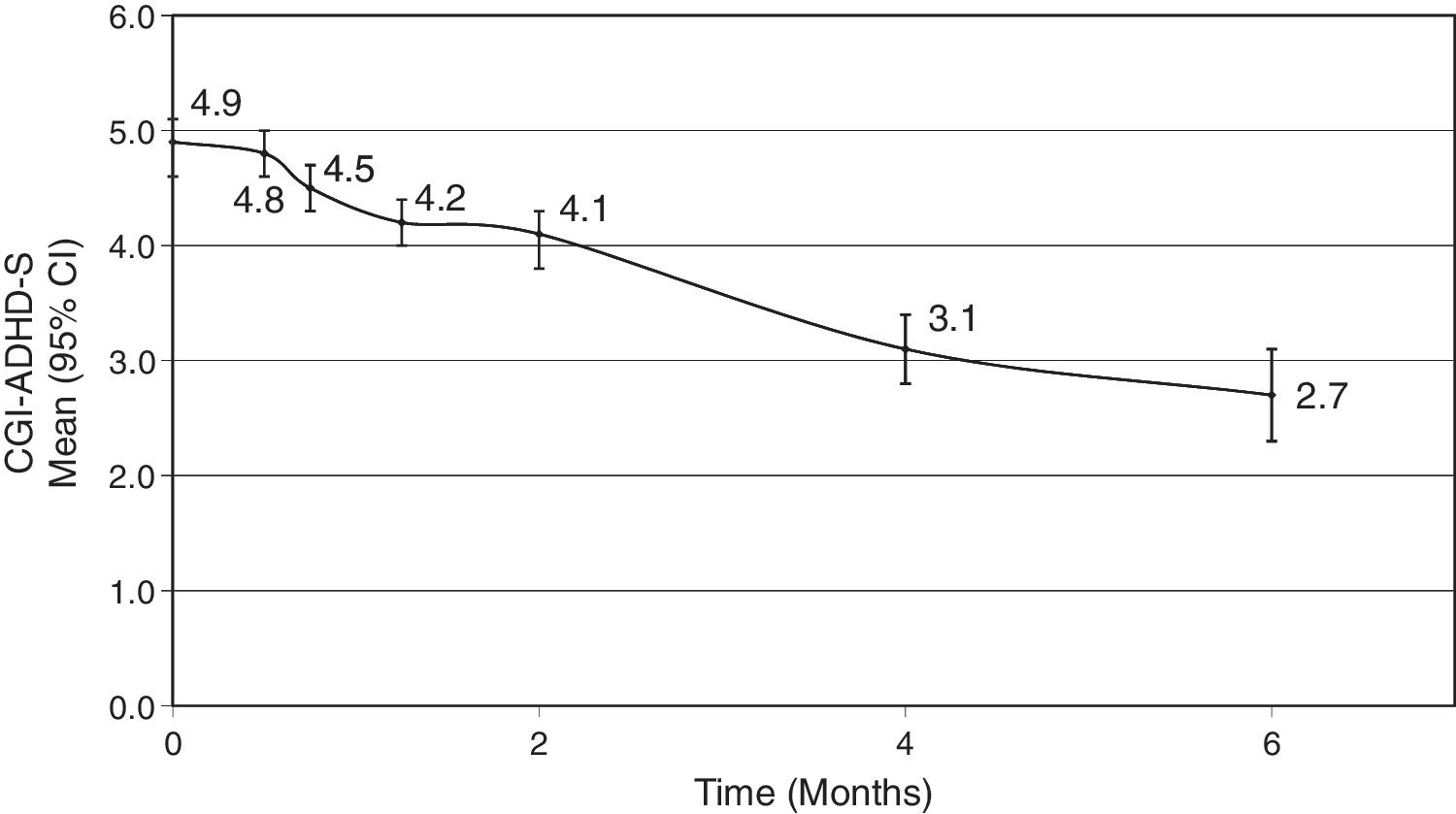
Change in Clinical Global Impressions–Severity (CGI-S) over time during atomoxetine therapy. The change from baseline was statistically significant from the week 3 visit onward (p < 0.05). The scores on the GCI-S improve: p < 0.05 for change from baseline 3 weeks, 5 weeks, 2 months, 4 months, and 6 months (baseline = 4.9 [n = 21], mean change −0.03 [n = 20], −0.6 [n = 19], −0.7 [n = 18], −1.7 [n = 16], and −2.1 [n = 16], respectively. ADHD-S = Attention-Deficit/Hyperactivity Disorder Rating Scale; CI = confidence interval.
Functional impairment
Functional improvements were seen after 2 and 6 months of ATX treatment as measured by the overall WFIRS-P score (Table 4). In the cohort that completed 6 months of ATX treatment, the overall score decreased from 0.87 at baseline to 0.61 at the final assessment, a change from baseline of −0.26 (p = 0.002). Functional improvement was evident in four of the six domains, including learning and school (p = 0.002), child self-concept (p = 0.006), family (p = 0.014), and life skills (p = 0.025). Comparable results were found in the group of 18 children who were still receiving ATX at 2 months (Table 4). In this group, the overall score decreased from 0.86 at baseline to 0.64 at 2 months, a change of −0.22 (p = 0.002), with significant improvements from baseline evident in family (p < 0.001), life skills (p = 0.007), and learning and school (p = 0.029) domains.
All values are the mean (± standard deviation).
The p values were determined using the Wilcoxon signed rank test.
Abbreviation: WFIRS-P = Weiss Functional Impairment Rating Scale–Parent-Report.
Safety
Atomoxetine was generally well tolerated; there were no serious treatment-emergent adverse events during the study. All except for 1 patient experienced treatment-emergent adverse events, most commonly abdominal pain (n = 8; 38%), somnolence (n = 8; 38%), headache (n = 7; 33%), and decreased appetite (n = 5; 24%). During the study, the children with ADHD increased in height from 129.0 ± 7.9 cm to 131.1 ± 8.2 cm (p < 0.001) and in weight from 28.3 ± 5.8 kg to 28.8 ± 5.4 kg (p = 0.112). Heart rate increased from 77.0 ± 10.4 beats per minute (bpm) at baseline to 87.0 ± 9.3 bpm at end point (p < 0.001), but blood pressure did not change significantly. Systolic blood pressure was 104.3 ± 7.4 mmHg and 103.0 ± 8.8 mmHg (p = 0.645) at baseline and end point, respectively, and diastolic blood pressure was 63.8 ± 7.4 mmHg and 66.7 ± 5.4 mmHg (p = 0.138) at these respective time points.
Discussion
This pilot longitudinal study offers preliminary evidence that ATX treatment not only reduces ADHD core symptoms but also enhances neuropsychological outcomes as well as the ability to function in daily life over a 6-month period. ATX produced a strong effect on neuropsychological function on the TEA-Ch and the BRIEF. In contrast, the global domain scores of the NEPSY did not show significant improvements from baseline beyond what was seen in the control group.
The Memory and Learning domain of the NEPSY improved significantly in the children with ADHD who were treated with ATX for 6 months, with the magnitude of the changes being comparable to those seen in age- and sex-matched controls. It is unclear why the Memory and Learning domain showed significant changes over 6 months, whereas changes in other domains of the NEPSY were not significant. The lower score on the Memory and Learning domains at baseline (vs. baseline scores on the other domains) suggests more marked impairment and hence greater room for improvement. However, this does not explain the positive change in the control group (inasmuch as NEPSY scores are standardized for age and sex), thereby raising the possibility of a practice effect. Cognitive improvements have been reported with second-generation antipsychotic drugs in patients with schizophrenia, but when a healthy control group was included, the magnitude of the improvement was consistent with the practice effects observed in healthy controls (Goldberg et al. 2007).
Gioia and colleagues (2002) reported that children with ADHD show impaired executive function on the BRIEF compared with a normative control group. In particular, a cohort of children with ADHD, inattentive type, with a mean age of 8.8 years and mean IQ of 97.1—consistent with the profile of participants in the present study—exhibited higher scores (poorer performance) than the control cohort on all BRIEF scales except for shift (which measures the ability of a subject to move freely from one situation or task to another as the situation demands). In comparison, a cohort with ADHD, combined type, with a mean age of 7.9 years and mean IQ of 96.4, exhibited higher mean scores than the control cohort on all BRIEF scales.
In the present study, significant improvements in the ATX-treated group were observed on all scales of the BRIEF when rated by parents and on four of the eight scales when rated by teachers. More importantly, significant improvements in the global executive composite score were seen on both the parent and teacher versions of the BRIEF, suggesting that this benefit of ATX extends across treatment settings. Moreover, confirmation by multiple informants increases the reliability and dimensions of the findings. This contrasts with the changes from baseline observed in the control group, which were generally small and not significantly different from zero. This can be understood, in part, by the limited possibility of the control group to show change given that the baseline values of the parents' ratings on BRIEF were already below the norm (i.e., reflecting better function than the norm).
There are several possible reasons for the discrepant findings of improvements on the TEA-Ch (from baseline to end point) and the BRIEF (from baseline to end point vs. control group but not on the functional domain scores of the NEPSY (from baseline to end point vs. control group). It is possible that additional examination of the individual subtests of the NEPSY (which is beyond the purview of this paper) might reveal specific changes that are not uncovered using summary standard domain scores. In addition, there are differences in the instruments used that may have contributed to the differences in results: (1) The TEA-Ch provides more specific assessments of attentional processes than the domain scores of the NEPSY, and (2) the BRIEF is based on observations of the child's behavior made by the parent and the teacher, in contrast to direct neuropsychological testing of the child with the TEA-Ch and the NEPSY.
The concurrent efficacy of ATX in decreasing ADHD symptoms and improving CGI-S score is consistent with findings from previous randomized, controlled trials of children and adolescents with ADHD (Michelson et al. 2001; Spencer et al. 2002; Kelsey et al. 2004; Weiss et al. 2005; Brown et al. 2006). These studies established that ATX treatment reduces ADHD symptoms when rated by parents and teachers alike, indicating that the efficacy of treatment extends across the home and school settings. The present study imparts further information about outcomes and the time course of changes from 2 to 6 months. In particular, further reductions in ADHD symptoms were achieved as treatment with ATX was continued beyond 2 months.
Findings from the WFIRS-P demonstrated that treatment with ATX was associated with reductions in the functional impairment associated with ADHD. Overall, the mean item score was reduced from 0.87 at baseline to 0.61 at the 6-month end point, with significant improvement across four of the six domains (including learning and school, life skills, self-concept, and family). These results are consistent with data from a larger study involving 209 children with ADHD in which ATX reduced the mean item score on the WFIRS-P from 1.1 ± 0.4 at baseline to 0.6 ± 0.4 at the 3-month end point (Weiss et al. 2007). When the 50 items were summed, the total score was reduced from 53.9 at baseline to 30.9 after 3 months of treatment, with reductions in all domains ranging from 40% to 47%. The only domains of the WFIRS-P that were not significantly reduced (improved) in the ATX-treated group in the present study were social activities and risky activities. Possible explanations for these findings may relate to the potential overrepresentation of the inattentive subtype of ADHD in the present study population (see below) and to the low initial scores on these domains in this relatively young cohort, who are less likely than older children, adolescents, and/or young adults to be engaged in risky activities such as smoking and drug abuse. Of interest, improvement in the child self-concept domain was not significant at 2 months but was at 6 months, suggesting that improvement in this domain may lag ADHD core symptom improvement.
The present study cohort included a high percentage of children with the inattentive subtype of ADHD (71.4%); this is noteworthy given that the combined subtype typically accounts for higher proportions of children in other studies of ATX (Michelson et al. 2001; Spencer et al. 2002; Kelsey et al. 2004; Michelson et al. 2004; Weiss et al. 2005). The present study did not specifically set out to preferentially recruit children with the inattentive subtype; rather the overproportion of this subtype is likely due to the referral patterns of the study site compared to typical practices that participate in multicenter trials. Cognitive deficits in ADHD have been related to inattentiveness but not to hyperactive-impulsive symptoms (Nigg and Casey 2005; Martel et al. 2007). Accordingly, many children with the inattentive subtype may also meet criteria for specific learning disabilities, information that was not specifically collected in the database for this pilot study. It will be interesting to explore whether treatment effects of ATX on neuropsychological function are influenced by the presence of such disabilities. The high percentage of the inattentive subtype also explains the lower ratings by teachers compared to parents on the ADHDRS-IV, although teachers may be more sensitive to disruptive behaviors than to inattentiveness. Of interest, although initial ratings of core symptoms by teachers were higher than those of parents, both parent and teacher ratings showed parallel, progressive improvements over time with ATX treatment (see Fig. 2).
The inclusion of a healthy control group without psychiatric disorders represents a considerable strength of the present study; the inclusion of controls was useful for observing the absence of a treatment effect on the NEPSY. Such results emphasize the importance of including a control group when evaluating neuropsychological outcomes. However, a control group of untreated ADHD children may be preferable for assessing treatment effects on neuropsychological functions in future studies. Such an untreated group in this study may have contributed to a better understanding of the results in part because the developmental trajectory of untreated ADHD patients in this age group over a 6-month period is not known. Furthermore given the variable impairment on each domain at baseline across the ADHD population, future research may be more illuminating if only patients with specific impairments are included at baseline (e.g., only ADHD children who meet prespecified impairment of a particular neuropsychological domain).
The present pilot study has several potential limitations as well as strengths. First, the sample size was small; therefore the p values should be interpreted with caution. Consistent with its nature as a pilot study, many statistical tests were conducted in an effort to generate hypotheses for future clinical testing; however, such multiple testing may increase the likelihood of obtaining false-positive results by random probability. Second, this was a single-arm study; hence, the effects of ATX were not compared with those of a placebo (if any). Although improvements on the various instruments may in fact be ascribed to a treatment effect of ATX, other factors, including practice effects and regression to the mean, cannot be excluded as contributors to the observed changes over time. The improvements with ATX were observed across multiple instruments and informants, as well as when compared with a healthy control group, thereby suggesting that they exceeded mere practice effects. However, because only two instruments were completed by the control group (the NEPSY and the BRIEF–Parent), the actual contributions of practice effects could not be determined conclusively by the present study. The TEA-Ch was not administered to the control group because it is not subject to practice effects, given that two parallel forms are available for serial administration (Manly et al. 1999). Finally, only children ages 6–10.5 years at entry who had normal intelligence were included, and children with certain co-morbidities were excluded. In addition, mean IQ was somewhat lower in the ADHD group than the control group so that IQ effects, if present, may be aliased with group effects. Treatment-naïve patients, nonwhite races, and individuals with the hyperactive-impulsive ADHD subtype were underrepresented in the study cohort, and, as noted above, individuals with the inattentive subtype of ADHD were overrepresented. These factors may limit the generalizability of our findings to all categories of ADHD patients. However, the strengths of our methods reside in the long-term longitudinal design, the use of controls and extensive neuropsychological assessments permitting a preliminary conclusion on practice effect, the concurrent inclusion of clinical and daily functioning outcomes, and the use of ratings from both teachers and parents.
Conclusion
In summary, our preliminary findings suggest that ATX: (1) Improves neuropsychological function as measured by the TEA-Ch data and both parent and teacher versions of the BRIEF; (2) reduces ADHD core symptoms as measured by the parent and teacher versions of the ADHDRS-IV and by the investigator-rated CGI-S; and finally, (3) ameliorates functional impairment as measured by the WFIRS-P. Notably, our findings are consistent with an earlier report of improved executive function in a pilot study of 9 children with ADHD using the Cambridge Neuropsychological Test Automated Battery (Barton et al. 2005). Correlative analyses between and among the various outcomes measured in that study were judged to be beyond the scope of the present report and are planned for a future paper. On the basis of the results of this pilot study, larger, well-controlled, longitudinal studies conducted in cognitively impaired patients, including an untreated control group, are warranted to elucidate potential mechanisms for the treatment effects as well as the complex interrelationships among core behavioral symptoms of ADHD and neuropsychological processes.
Disclosures
Drs. Maziade and Rouleau have served as paid investigators, speakers, and grant recipients for the present study and its follow up, which is an investigator-initiated trial with Dr. Maziade as the principal investigator. Dr. Maziade also has served as a paid consultant to GlaxoSmithKline (GSK) and Eli Lilly and has received research funding from GSK, Eli Lilly, and AstraZeneca. Drs. Rogers and Dickson are employees of, and minor shareholders in, the study sponsor. Ms. Lee and Dr. Davis have no financial interests to disclose.
Footnotes
Acknowledgments
Assistance in manuscript preparation was provided by Stephen W. Gutkin, Rete Biomedical Communications Corp. (Wyckoff, NJ). Marguerite Ennis, Ph.D., provided statistical review. Author contributions were as follows: Study conduct and design: Drs. Dickson, Rouleau, Maziade, Davis; oversight of study design: Drs. Dickson, Rouleau, Maziade, Davis; acquisition of data, Dr. Davis; statistical analyses, Dr. Davis, Ms. Bobbie Lee; interpretation of data, all authors; manuscript preparation, Dr. Dickson with assistance from Stephen W. Gutkin; review, revision, and approval of manuscript, all authors.
Funding for this research was provided by Eli Lilly and Company, Toronto, Canada.