
Abstract
Introduction:
This study compared two atomoxetine titration dosing schedules and two atomoxetine maintenance doses for treating adolescent attention-deficit/hyperactivity disorder (ADHD) inattention and hyperactivity/impulsivity.
Methods:
Adolescents (N = 267) were randomized to a slow or fast titration schedule. Patients who responded continued on a 40-week maintenance treatment, randomized to either 0.8 or 1.4 mg/kg/day.
Results:
During the acute period, significant benefit was demonstrated with both titration schedules on the ADHD Rating Scale total score. Although patients in both groups maintained benefit relative to week 0, statistically significant loss of benefit was found for patients maintained on 0.8 mg/kg/day but not on 1.4 mg/kg/day. A similar pattern was observed on the Clinical Global Impressions-ADHD-Severity scores and Life Participation Scale for ADHD-Child Version scores. Mean grades for most subjects improved for patients in both maintenance treatment groups although most improvements were not statistically significant.
Conclusions:
In adolescents with ADHD, treatment benefit at 8 weeks was better maintained long-term with 1.4 mg/kg/day than with 0.8 mg/kg/day. Improvement in adaptive functioning and age-appropriate developmental function was also demonstrated. Atomoxetine 0.8 and 1.4 mg/kg/day were equally well tolerated.
Clinical Trials Registry:
Maintenance of benefit with atomoxetine hydrochloride in adolescents with ADHD, NCT00191035.
Introduction
Numerous clinical trials have demonstrated the efficacy and safety of atomoxetine for treating ADHD (Michelson et al. 2001; Michelson et al. 2003; Michelson et al. 2002; Spencer et al. 2002; Kelsey et al. 2004; Allen et al. 2005). However, the cumulative benefit of atomoxetine treatment for extended periods of time beyond initial symptom reduction is not definitively known. Therefore, it was hypothesized that adolescents treated with atomoxetine will maintain significant efficacy in the reduction of ADHD symptoms over time leading to significant improvements in age-appropriate developmental function in areas such as academic achievement, social development, family dynamics, and risk behaviors in these patients. Additionally, it is important to determine the optimal dose of atomoxetine in order to achieve treatment benefits that can be maintained over an extended period of time in adolescents with ADHD.
The current study measured the effects of atomoxetine hydrochloride, a selective norepinephrine reuptake inhibitor, in adolescents with ADHD focusing on the benefits of atomoxetine in ameliorating the impairments associated with ADHD. This was a long-term study that assessed the difference in maintenance of response over 40 weeks between atomoxetine treatment at 0.8 mg/kg/day and 1.4 mg/kg/day (the maximum label dose). The primary objective for the maintenance period was to test for a difference in maintenance of response between atomoxetine therapy at a dose of 0.8 mg/kg/day versus therapy at a dose of 1.4 mg/kg/day in adolescents who responded during an acute atomoxetine treatment period. The benefit of atomoxetine maintenance treatment on adaptive functioning and age-appropriate developmental function, including academic achievement was also determined. This study also compared the efficacy and tolerability of two different dosing titrations (a slow titration schedule of 0.5/1.0/1.2 mg/kg/day and a fast titration schedule of 0.5/1.2 mg/kg/day). The hypothesis for the acute treatment period was that the slow titration schedule would have greater tolerability than the fast titration.
Methods
Patient population
Patients were recruited during routine office visits for ADHD, by referral, and by advertisement. Adolescents, 13 to ≤16 years of age, who met criteria for ADHD as defined by the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition Text Revision (DSM-IV-TR) were eligible to participate in the initial 8-week (acute treatment) period of the study. Additional eligibility criteria included ADHD diagnosis confirmed using the Kiddie Schedule for Affective Disorders and Schizophrenia for School Aged Children-Present and Lifetime Version (K-SAD-PL: Behavioral), a score of at least 1.5 standard deviations above the age and gender normative sample data for their ADHD diagnostic subtype on the ADHD Rating Scale-IV-Parent Version: Investigator Administered and Scored (ADHDRS), and a score of ≥70 on the Kaufman Brief Intelligence Test (K-BIT). Patients who responded to the study medication (based on specific criteria described in detail in the treatment section below) during the acute treatment period were eligible to continue on to an additional 40-week maintenance treatment period.
Exclusion criteria included weight less than 40 kg or greater than 70 kg at visit 1, patients taking any psychotropic medication on a regular basis or anticonvulsants for seizure control, a history of bipolar disorder, psychosis, autism, Asperger's syndrome, pervasive developmental disorder, pregnant or breastfeeding females, uncontrolled hypertension, or patients who had participated in a previous study of atomoxetine.
Informed consent was obtained from all patients' legal representatives prior to their enrollment in the study. The study protocol and the informed consent document were reviewed and approved by the Institutional Review Boards at all study sites. Patient assent was completed when it was required by the site's Review Board. The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and in consistency with Good Clinical Practices.
Study design
This was a randomized, double-blind study that investigated 2 different titration dosing schedules for atomoxetine during an acute treatment period (8 weeks) and two different maintenance doses during a subsequent 40-week maintenance treatment period. The study was conducted at 26 sites in the United States. The first patient was randomized to treatment on March 08, 2004, and the last patient completed the trial on November 20, 2006. Patients at visit 1 who were taking stimulants for ADHD treatment were required to be medication-free for at least 24 hours prior to visits 2 and 3. Patients who were taking any medication excluded by the protocol (e.g., a psychotropic medication) at visit 1 that has a half-life greater than 24 hours required a washout period at least 5 half-lives of the parent compound and any active metabolite prior to visit 2. After an initial assessment/evaluation period and the drug washout period (visits 1–3) patients were randomized to one of two different dose titration schedules of atomoxetine hydrochloride for 8 weeks. A computer algorithm generated randomization numbers to blindly assign patients to dosing groups in a 1:1 fashion at the site level. These randomization numbers were made available to the investigative site via a telephone Interactive Voice Recording System (IVRS), and the treatment assignments were not unblinded until after the database was locked. Patients were monitored at biweekly visits (14 to 18 days between visits; visits 3–7) during the treatment period. Patients who had demonstrated a response (hereafter referred to as “responders”, the criteria for which are described below) during the acute treatment period were re-randomized, double-blind, to receive one of 2 different atomoxetine doses during the 40-week maintenance period (visits 7–12).
Treatment
During the acute treatment period, patients received 2 different titration dosing schedules of atomoxetine. Patients in the fast titration group received atomoxetine at a starting dose of 0.5 mg/kg/day for a minimum of 3 days followed by 1.2 mg/kg/day for the remainder of the 8-week study period (0.5/1.2 group). Patients in the slow dose titration group received atomoxetine at a starting dose of 0.5 mg/kg/day for 7–9 days, followed by 1.0 mg/kg/day for 7–9 days, and then 1.2 mg/kg/day for the remainder of the 8-week study period (0.5/1.0/1.2 group).
During the 40-week maintenance treatment period, responders to the acute treatment, as demonstrated by a decrease of ≥1 point on the Clinical Global Impressions-Attention-Deficit/Hyperactivity Disorder-Severity (CGI-ADHD-S) scale at week 8, were re-randomized to receive either a low dose of 0.8 mg/kg/day or the maximum label dose of 1.4 mg/kg/day for the duration of treatment. The dose did not exceed 100 mg/day regardless of the patient's weight. Investigators were blind to the criterion used to determine treatment responders.
Compliance during the acute treatment period was assessed at each study visit by direct questioning of parent, guardian, and/or the patient and by monitoring the used and unused blister cards. During the maintenance treatment period, patients who missed >7 consecutive days of study medication or took <70% of the prescribed study medication during a visit interval were considered to be significantly noncompliant. Moreover, patients who intentionally or repeatedly took more than the prescribed amount (120%) of medication as judged by the investigator were also considered significantly noncompliant. Patients who were significantly noncompliant were discontinued from the study.
Assessments
Primary Efficacy Measure
The ADHDRS was used to measure primary efficacy. The 18-item scale includes 1 item for each of the 18 symptoms in the DSM-IV diagnosis of ADHD and was scored by a healthcare professional during the patient interview regarding the symptom severity over the previous week. Each item on the scale was scored on a 0 to 3 scale (0 = none, 1 = mild, 2 = moderate, 3 = severe; DuPaul et al. 1998) and the total score was computed as the sum of the scores on each of the 18 items. In addition, the subscales for inattention (the sum of the scores on the odd-numbered items on the ADHDRS scale) and hyperactivity/impulsivity (the sum of the scores on the even-numbered items) were also measured, but were considered as secondary measures. The scale was administered at pre-drug baseline (week 0), 4 and 8 weeks of the acute period and 8, 16, 24, 32, and 40 weeks of the maintenance period.
Secondary Efficacy Measures
The secondary efficacy measures included the CGI-ADHD-S, the Life Participation Scale for ADHD Child Version (LPS-C), the Family Assessment Measure Version III (FAM III), the Woodcock Johnson-III Tests of Achievement (WJ-III), the Youth Risk Behavior Survey (YRBS), and grade point average (GPA).
The CGI-ADHD-S was measured on a 7-point scale (1 = normal, 7 = extremely ill) as a single-item rating of the clinician's assessment of the severity of ADHD symptoms in relation to the clinician's total experience with ADHD patients (Guy 1976). The CGI-ADHD-S data were collected at the same times as the ADHDRS.
The LPS-C was measured on a 24-item parent-rated scale, which measured adaptive functioning related to treatment for ADHD (Saylor et al. 2007). It was completed separately by the investigator and the parent to allow for scale validation. The LPS-C measures improvements in social, emotional, cognitive, educational, and affiliative (family, friend) functioning, which indirectly reflect improvements in executive functioning. The LPS-C data were collected at pre-drug baseline, the end of the acute period, and the end of the maintenance period.
The FAM III, a self-report instrument that provides quantitative indices of family strengths and weaknesses, was measured as a general scale component that focused on the family as a system and a self-rating scale to assess the patient's perception of functioning in the family. The FAM III assesses basic concepts such as task accomplishment, role performance, communication, affective expression, involvement, control and values, and norms. The FAM III data were collected at pre-drug baseline, the end of the acute period, and the end of the maintenance period.
The WJ-III Tests of Achievement Form A were used to measure academic achievement using both the Standard and Extended batteries. The Standard battery provided a broad set of scores (included tests 1 through 12), while the Extended battery (included 10 tests) provided more in-depth diagnostic information on specific academic strengths and weaknesses. The WJ-III data were collected at pre-drug baseline, the end of the acute period, and the end of the maintenance period.
The YRBS was measured by monitoring tobacco use, unhealthy dietary behaviors, inadequate physical activity, alcohol and other drug use, sexual behaviors leading to unintended pregnancy and/or sexually transmitted diseases, and behaviors contributing to unintentional injuries and violence. The YRBS data were collected at pre-drug baseline, the end of the acute period, and the end of the maintenance period.
The baseline grade point averate (GPA), measured on a 4.0 scale (A = 4, B = 3, C = 2, D = 1, F = 0), included the following subjects: English, Math, Science, and Social Studies. Additional measurements of GPA were obtained at 32, 40, or 48 weeks, depending on the patient's school grading period. Parents were asked to bring the report cards to the visit.
Safety
Safety and tolerability measures included electrocardiogram, standard laboratory tests including chemistry, hematology, and urinalysis panels, vital signs, height and weight, concomitant medication use, and monitoring of adverse events throughout the course of the study. To assess the tolerability of the two titration dosing schedules, safety and tolerability measures were compared 4 weeks after initiating treatment, when patients in both groups had reached 1.2 mg/kg/day.
Data analysis
The main objective of this study was to assess the difference between maintenance treatment at 0.8 mg/kg/day and at 1.4 mg/kg/day at the end of 40 weeks after the initial benefit of atomoxetine treatment during the 8-week acute treatment period. The primary outcome for this study was a treatment group comparison of change from baseline to last observation carried forward (LOCF) maintenance period endpoint in ADHDRS total score using a fixed-effects analysis of covariance (ANCOVA) model with terms for baseline score, treatment, and investigator. ADHDRS and subscores and CGI-ADHD-S scores were also analyzed using a restricted maximum likelihood (REML)-based mixed models repeated measures (MMRM) technique in addition to the LOCF approach mentioned above. All secondary efficacy measures as well as continuous safety measures were analyzed using a fixed-effects ANCOVA model with terms for baseline score, treatment, and investigator. Categorical safety measures (eg, treatment response, incidence of adverse events, etc) were analyzed using Fisher's Exact Test. All tests were two-tailed. Effect sizes were calculated for most efficacy measures for both within-group changes (the absolute value of the baseline mean minus the endpoint mean, divided by the average standard deviation of the baseline and endpoint scores) and between-group changes (the absolute value of the mean change for one treatment group minus the mean change for the other treatment group, divided by the average standard deviation of the mean changes from both treatment groups).
The study was planned to randomize 520 patients to ensure approximately 160 patients per group with baseline and endpoint data during the maintenance period. This estimate assumed a 75% response rate (a decrease of ≥1 point on the CGI-ADHD-S) at the last visit of the acute period (week 8), and approximately 85% of patients would have non-missing baseline and post-baseline ADHDRS total scores during the maintenance period. This sample size would ensure more than 80% power based upon the expected results from the primary efficacy measure (ADHDRS total score) when comparing the 0.8 mg/kg/day and 1.4 mg/kg/day maintenance treatment groups. A difference of 4.4 points and a standard deviation of 14.0 was expected when comparing the change from baseline (last visit of the acute period [week 8]) to the maintenance period LOCF endpoint for the two maintenance treatment groups.
Results
Demographics
Due to issues with slow enrollment, patient recruitment ended before reaching the planned number of patients. All enrolled patients were allowed to complete the study. Despite having fewer patients than planned, the smaller than expected variability (standard deviation = 9.6) on the ADHDRS total score resulted in 83% power for the expected treatment difference of 4.4 points based upon the patients who completed the maintenance period. A total of 333 patients were screened, and 267 patients were randomized to receive atomoxetine using 2 different dose titration schedules (132 patients to 0.5/1.2 mg/kg/day and 135 patients to 0.5/1.0/1.2 mg/kg/day) during the 8-week acute treatment (Table 1). During the maintenance treatment period, a total of 178 patients were re-randomized to treatment with atomoxetine using 2 different dosing strategies (88 patients to 0.8 mg/kg/day and 90 patients to 1.4 mg/kg/day) for the duration of the study. A total of 66.7% of patients from the acute treatment period continued on to the maintenance treatment period (Figure 1). The primary reasons for not continuing on to the maintenance treatment period included not meeting response criteria (9.4%), adverse events (7.9%), lost to follow-up (4.1%), patient decision or personal conflict (3.4%), non-compliance (3.0%), or lack of efficacy (2.3%). Of the 89 patients who did not continue, 28.1% were discontinued because they did not meet the response criteria.
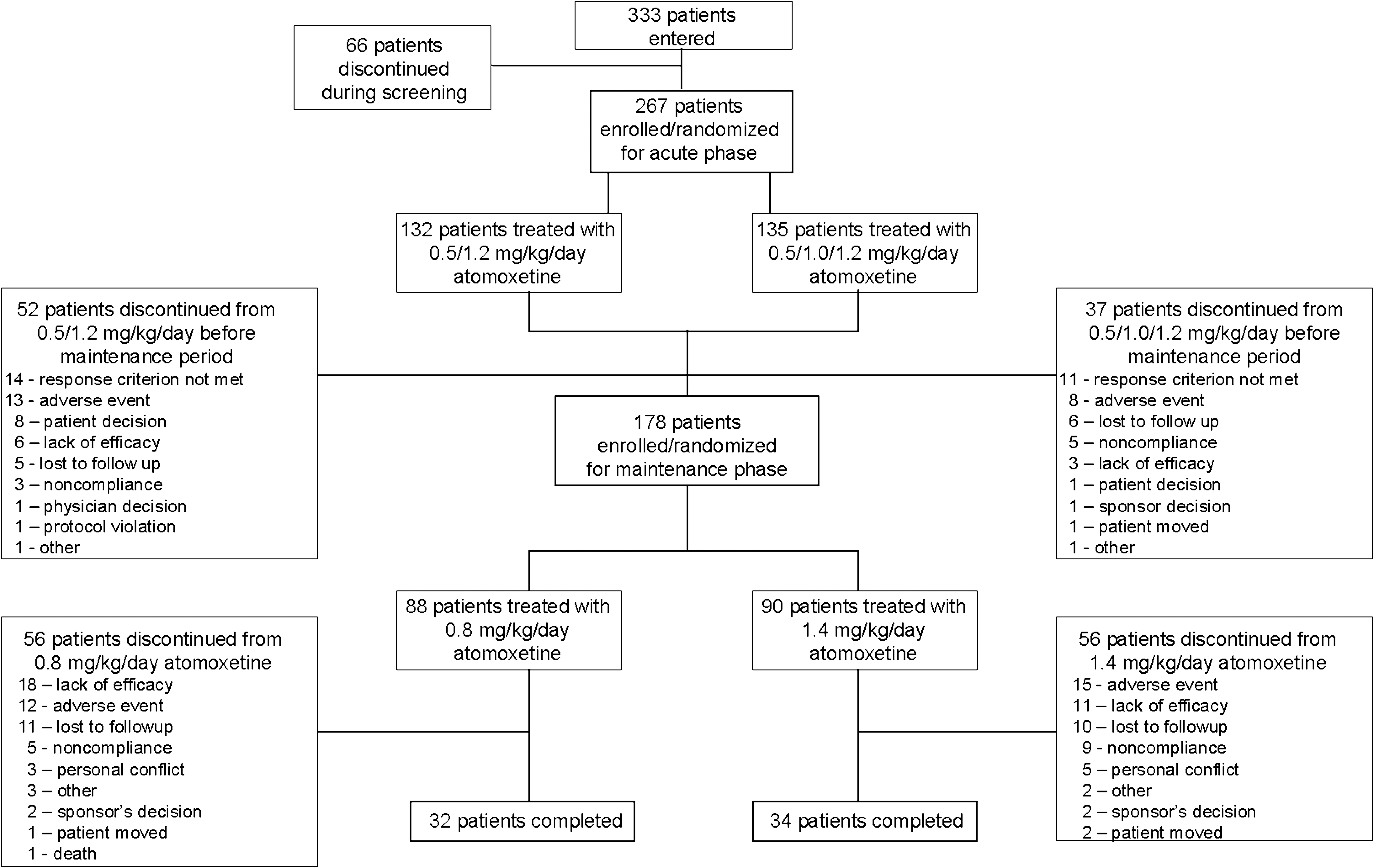
Patient disposition during the study.
No statistically significant differences were observed between treatment groups for any characteristic at baseline.
Abbreviations: SD = Standard deviation; ADHD = Attention-deficit/hyperactivity disorder.
Age and gender were similar across treatment groups in both treatment periods. Patients were primarily of Caucasian origin and there were more males than females in all treatment groups. At baseline, the majority of patients met the criteria for inattentive or combined ADHD subtypes. Furthermore, >50% of patients in all treatment groups had a history of stimulant use.
Efficacy
ADHDRS Total Scores
During the acute treatment period, atomoxetine treatment improved the mean change from baseline to LOCF endpoint in ADHDRS total score for the 0.5/1.2 and 0.5/1.0/1.2 mg/kg/day groups (Table 2). The treatment benefit achieved during the acute treatment period was maintained throughout the maintenance treatment period (i.e., scores did not return to pre-drug baseline; Figure 2). However, patients maintained on 0.8 mg/kg/day lost some of the benefit they had experienced during the acute treatment period, whereas patients maintained on 1.4 mg/kg/day did not. The increase in ADHDRS total scores, indicating a loss of benefit, was statistically significant in the 0.8 mg/kg/day group (3.80; p < .001), but was not significant in the 1.4 mg/kg/day group (1.93; p = .068) (Table 2). The difference between groups was not statistically significant (t[145] = 1.3, p = .194).
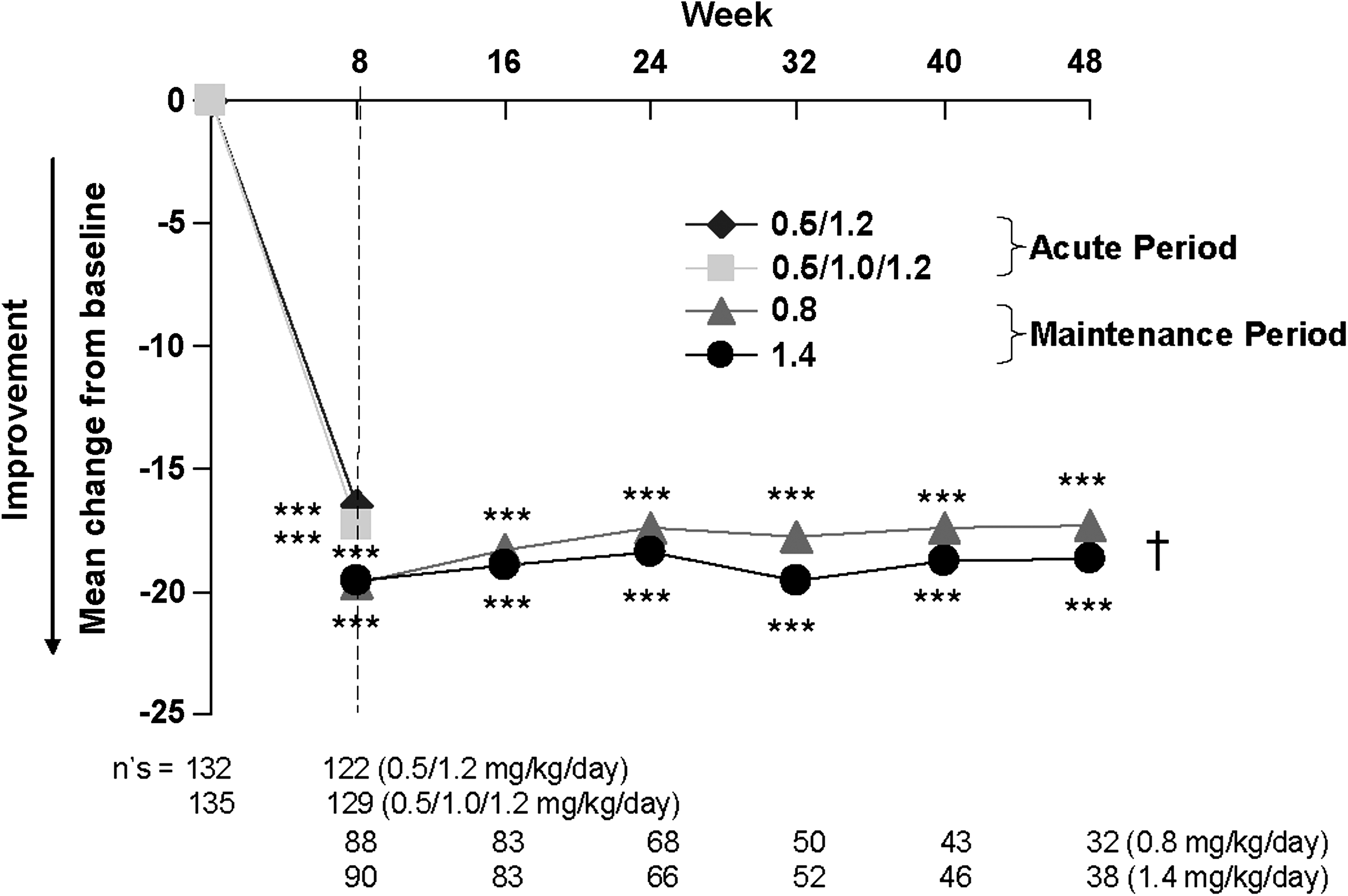
Maintenance of ADHDRS total scores during the 48-week treatment with atomoxetine. ADHDRS = Attention-Deficit/Hyperactivity Disorder Rating Scale-IV-Parent Version: Investigator Administered and Scored. ***p < .001 comparison vs. baseline; † = no between-group differences.
Abbreviations: SD = Standard deviation; LS Mean = Least squares mean; SE = Standard error; ADHDRS = Attention-Deficit/Hyperactivity Disorder Rating Scale-IV-Parent Version: Investigator Administered and Scored.
Results from the MMRM analysis (Figure 2) indicated scores from patients in either maintenance group were statistically significantly improved from pre-drug baseline at every visit (p < .001). When scores during the maintenance period were compared with the last visit of the acute period (week 8), statistically significant increases in scores, indicating loss of benefit, were seen at each week of the maintenance period for patients maintained on 0.8 mg/kg/day only (p ≤ . 035). The differences between groups were not statistically significant.
ADHDRS Subscale Scores
The mean change from baseline to LOCF endpoint in hyperactivity/impulsivity (−6.76 ± 0.39 and −6.75 ± 0.39 for the 0.5/1.2 and 0.5/1.0/1.2 mg/kg/day groups, respectively) and inattention (−9.73 ± 0.51 and −10.49 ± 0.50 for the 0.5/1.2 and 0.5/1.0/1.2 mg/kg/day groups, respectively) subscales on the ADHDRS, demonstrated significant improvement (p < .001 for both groups) with atomoxetine during the acute treatment period (Table 2). There was a small but statistically significant loss of benefit on the hyperactivity/impulsivity subscores for the 0.8 mg/kg/day group (1.16 ± 0.51; p = .025) and on the inattention subscores for both maintenance groups (2.63 ± 0.65 and 1.39 ± 0.65; p < .001 and p = .034 for the 0.8 and 1.4 mg/kg/day groups, respectively) relative to the end of acute treatment. The increase in hyperactivity/impulsivity scores was not statistically significant in the 1.4 mg/kg/day group (0.51 ± 0.51; p = .314). These results further suggest that there was some loss of benefit in both groups during the maintenance treatment compared with the benefit at the end of acute treatment, but the loss of benefit was small and lower in the 1.4 mg/kg/day group compared with the 0.8 mg/kg/day group; however, the differences between the groups were not significant (t[145] = .92, p = .357 and t[145] = 1.39, p = .167, for hyperactivity/impulsivity and inattention scores, respectively).
Results from the MMRM analysis indicated hyperactivity/impulsivity and inattention scores from patients in either maintenance group were statistically significantly improved from pre-drug baseline at every visit (p < .001). When hyperactivity/impulsivity scores during the maintenance period were compared with the last visit of the acute period (week 8), there were no statistically significant changes in scores for either maintenance groups at any visit. However, there was a statistically significant difference between groups at the last visit (week 48) resulting from a small increase in scores (1.15 ± 0.63) in the 0.8 mg/kg/day group and a small decrease in scores (−0.58 ± 0.59) in the 1.4 mg/kg/day group. Statistically significant increases, indicating loss of benefit, were seen for inattention scores at each visit of the maintenance period for patients maintained on 0.8 mg/kg/day (p ≤ .043). The differences between groups were not statistically significant.
CGI-ADHD-S Scores
During the acute treatment period, atomoxetine treatment showed significant improvement in CGI-ADHD-S scores compared with baseline in both groups. Change scores at week 4 of the acute phase were statistically significantly lower for both groups (1.05 ± 0.08 and −1.19 ± 0.08 for the 0.5/1.2 and 0.5/1.0/1.2 mg/kg/day titration groups, respectively; p < .001 for both), with no significant difference between the groups (p = .205). Change scores at week 8 were also significantly lower (−1.45 ± 0.09 and −1.53 ± 0.09 for the 0.5/1.2 and 0.5/1.0/1.2 mg/kg/day titration groups, respectively; p < .001 for both), with no significant difference between the groups (t[231] = .67, p = .504). The benefit from the acute treatment period was maintained throughout the maintenance treatment period (Figure 3). However, there was a small loss of benefit which was statistically significant only in the 0.8 mg/kg/day group (0.46 ± 0.11; p < .001) but not significant in the 1.4 mg/kg/day group (0.04 ± 0.11; p = .699). Similar to the observations with other efficacy endpoints, these results for CGI-ADHD-S scores indicate that there was some loss of benefit during the maintenance treatment period, but the loss of benefit was lower in the 1.4 mg/kg/day group compared with the 0.8 mg/kg/day group. The difference between the treatment groups was significant (t[145] = 2.7, p = .008).
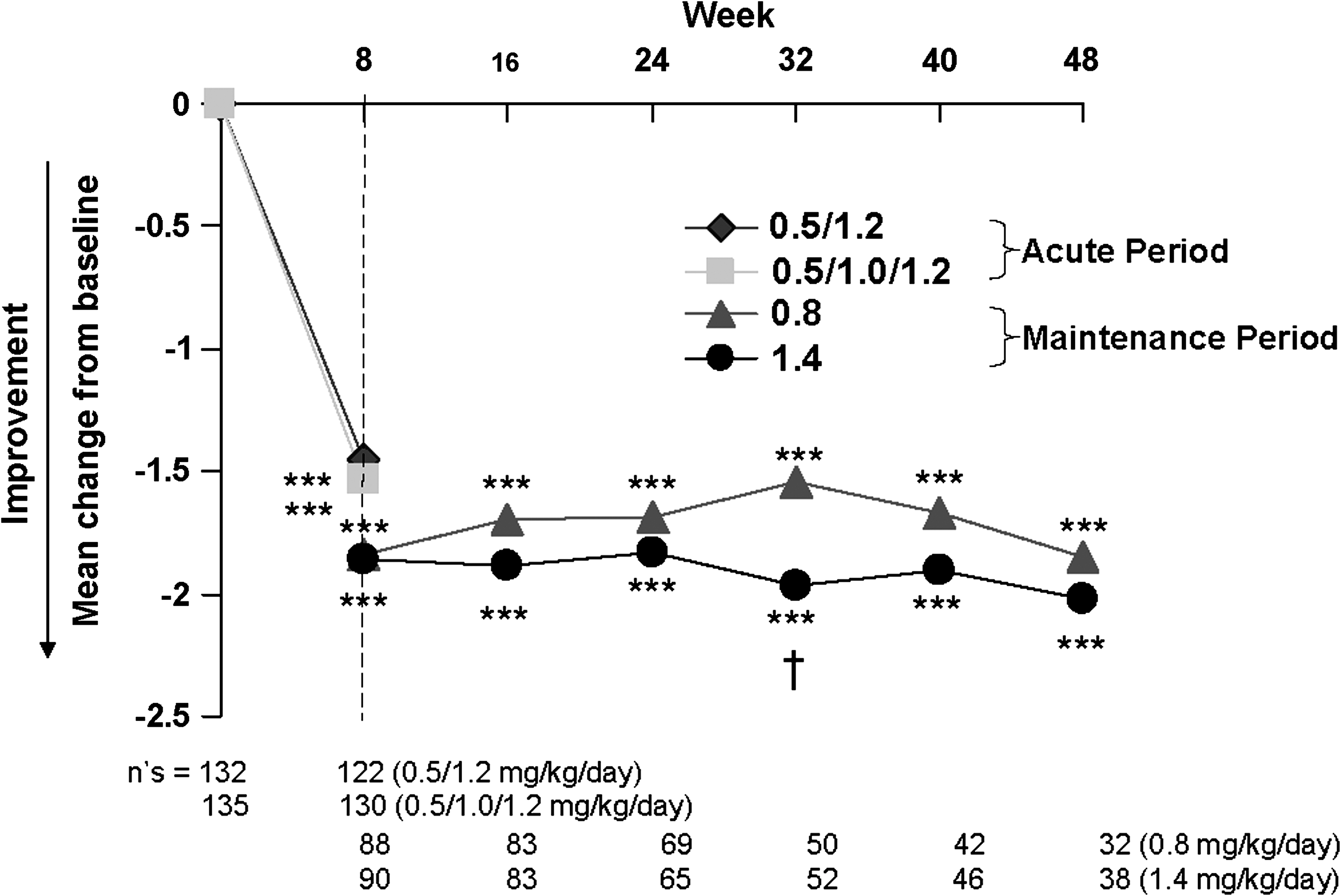
Maintenance of CGI-ADHD-S scores during the 48-week treatment with atomoxetine. CGI ADHD-S = Clinical global impressions-attention-deficit/hyperactivity disorder-severity. ***p < .001 comparison vs. baseline; † = significant between-group difference at week 32 only.
Results from the MMRM analysis (Figure 3) indicated scores from patients in either maintenance group were statistically significantly improved from pre-drug baseline at every visit (p < .001). When scores during the maintenance period were compared with the last visit of the acute period (week 8), statistically significant increases in scores, indicating loss of benefit, were seen at weeks 16, 24, and 32 of the maintenance period for patients maintained on 0.8 mg/kg/day (p ≤ .037). The difference between groups was statistically significant for week 32 only (p = .004).
Life Participation Scale for ADHD-Child Version
At the end of the acute treatment period, the LPS-C scores showed significant improvement in both treatment groups (9.7 ± 1.1 and 11.0 ± 1.0 for the 0.5/1.2 and 0.5/1.0/1.2 mg/kg/day groups, respectively; p < .001 for both); however, the difference in improvement between the treatment groups was not significant (t[195] = −.93, p = .356). During the maintenance period, there were decreases in LPS-C scores (−4.1 ± 1.5 and −2.1 ± 1.4 for the 0.8 and 1.4 mg/kg/day groups, respectively), indicating loss of benefit compared with the end of the acute treatment period. However, the loss of benefit was significant only in the 0.8 mg/kg/day group (p = .009) and not in the 1.4 mg/kg/day group (p = .138). The difference between the treatment groups was not significant (t[101] = .1.07, p = .289). The improvements in LPS-C scores from pre-drug baseline to the end of the maintenance treatment period were statistically significant (7.7 ± 1.4 and 10.5 ± 1.3 for the 0.8 and 1.4 mg/kg/day groups, respectively; p < .001 for both).
Family Assessment Measure Version III
The parent assessment of the FAM-III overall rating total t-score demonstrated significant improvement in both treatment groups at the end of the acute treatment (−0.84 ± 0.32, p = .009 for 0.5/1.2 mg/kg/day group; −1.25 ± 0.31, p < .001 for the 0.5/1.0/1.2 mg/kg/day group), with no significant difference between the treatment groups (t[161] = .99, p = .323). Moreover, these scores continued to demonstrate numerical improvement during the maintenance treatment period compared with the endpoint of the acute treatment period, although statistical significance was not demonstrated for the treatment groups or the difference between the treatment groups.
Woodcock-Johnson III Scores
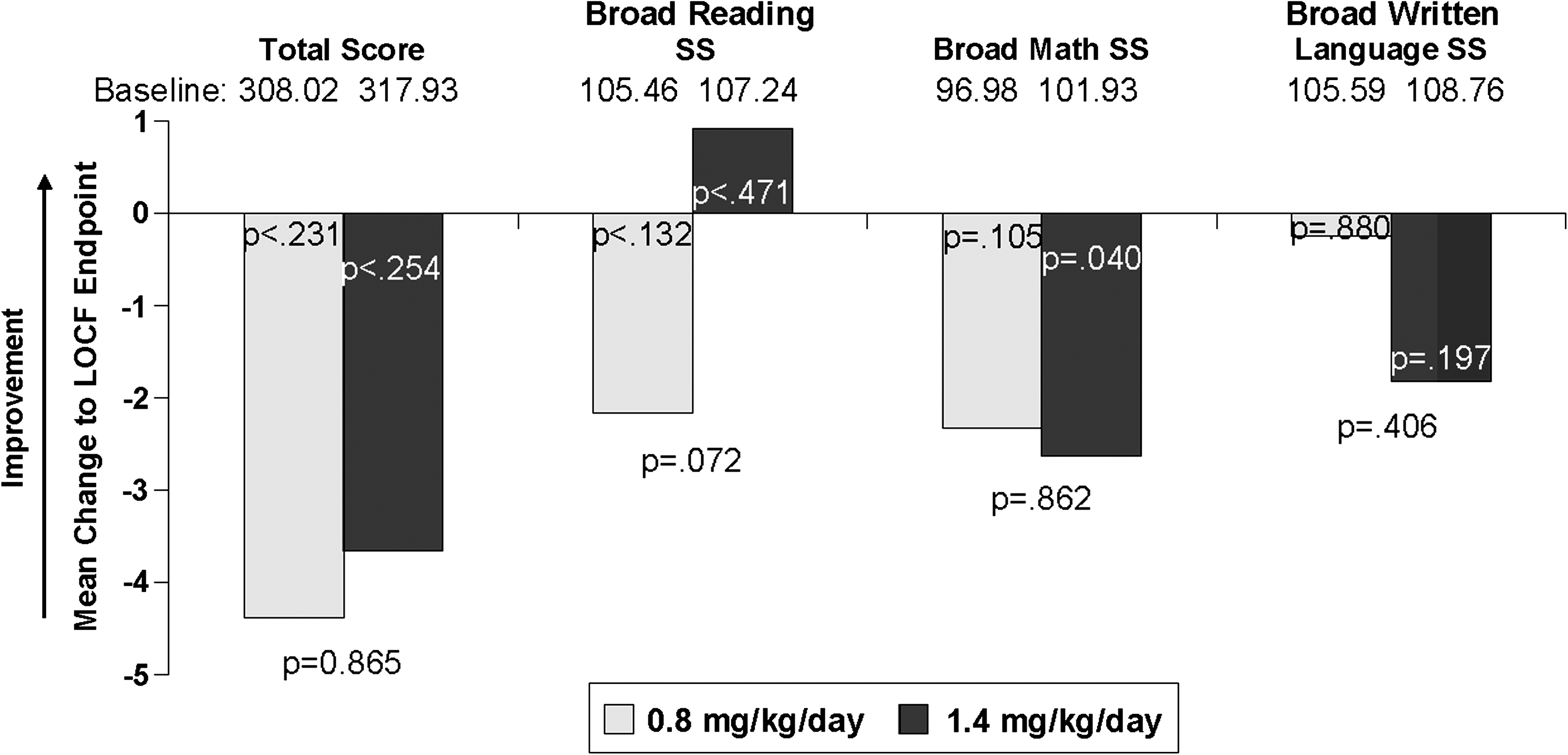
Woodcock-Johnson III Total Achievement scores, BROAD READING standard scores, and BROAD WRITTEN LANGUAGE standard scores showed significant improvement for both groups, with no significant differences between groups at the end of the acute treatment period (Figure 4). However, significant improvement was not demonstrated on the BROAD MATH standard scores. During the maintenance treatment period, WJ-III Total Achievement scores decreased, indicating loss of benefit compared with the end of the acute treatment period, but the decreases were not statistically significant (Figure 5). Similar results were demonstrated for the BROAD WRITTEN LANGUAGE standard scores. However, BROAD READING standard scores continued to improve in the 1.4 mg/kg/day group, but there was some loss in the 0.8 mg/kg/day group; neither observation was statistically significant. In contrast, there was a statistically significant decrease in BROAD MATH standard scores in the 1.4 mg/kg/day group (p = .040), but not in the 0.8 mg/kg/day group (p = .105). The differences between the treatment groups were not statistically significant for all scores.
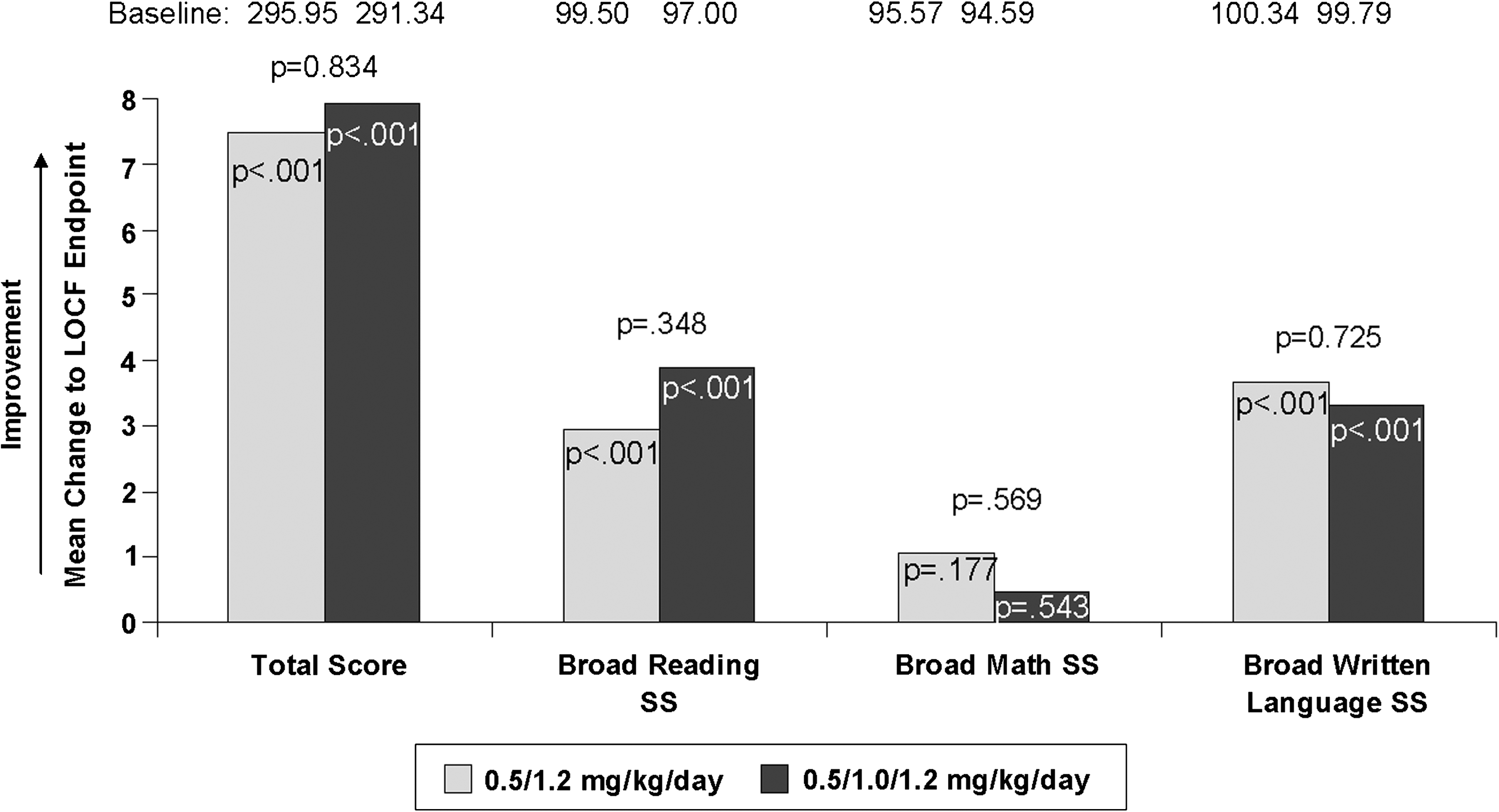
Mean change from baseline in Woodcock Johnson III scores during the 8-week acute treatment with atomoxetine. SS = Standard score; LOCF = last observation carried forward.
Mean change from baseline in Woodcock Johnson III scores during the 40-week maintenance treatment with atomoxetine. SS = Standard score; LOCF = last observation carried forward.
Youth Risk Behavior Survey (YRBS)
Improvement in the total YRBS subscores was not significant during either treatment period. However, the improvement in the unintentional injuries portion of the YRBS was statistically significant at the end of the acute treatment period (p < .001) in both groups compared with week 0. Similarly, the improvement in the unintentional injuries portion of the YRBS was significant during the maintenance treatment period in the 1.4 mg/kg/day group compared with week 0 (p < .001) and when comparing the end of the acute period with the end of the maintenance period (p = .036). Furthermore, there was a significant difference in the unintentional injuries portion of the YRBS between the 2 maintenance treatment groups (t[92] = 2.17, p = .032) when comparing the end of the acute period with the end of the maintenance period.
Grade Point Average
For most subjects (English, Math, Science, and Social Studies) numerical, but in most cases not statistically significant, improvement in GPA was demonstrated at the end of the maintenance treatment period compared with week 0 (Table 3) for both treatment groups. In the 0.8 mg/kg/day group, mean grades improved from C to B- for Math (p = .032). There were no significant differences within treatment groups for all other parameters or between treatment groups for any parameter, including the Kaufman Brief Intelligence (K-BIT) composite scores.
Abbreviations: SD = Standard deviation; LS Mean = Least squares mean; SE = Standard error; K-BIT IQ = Kaufman brief intelligence quotient.
Safety
At the 2- and 4-week time points, there were no statistically significant differences in the numbers of patients in the 2 dose titration groups who discontinued the study due to adverse events, and at the 4-week time point, there was no difference in tolerability between the 2 dose titration groups. No statistically significant differences were observed in any of the vital signs or in weight between the 0.5/1.2 mg/kg/day and 0.5/1.0/1.2 mg/kg/day groups. The most common treatment-emergent adverse events reported by ≥5% of patients during the both treatment periods are shown in Table 4. During the acute treatment period (8 weeks), the most commonly reported treatment-emergent adverse events included nausea, decreased appetite, dizziness, abdominal pain, fatigue, headache, vomiting, and somnolence (Table 4). During the long-term maintenance period nausea, nasopharyngitis, dizziness, and arthralgia were the only reported adverse events that occurred in at least 5% of patients in either treatment group. Dizziness was reported more often by patients in the 0.8 mg/kg/day group during the maintenance period than by patients in the 1.4 mg/kg/day group (p = .027).
Atomoxetine label dose was 0.5/1.2 mg/kg/day and slower dose was 0.5/1.0/1.2 mg/kg/day during the 8-week treatment period.
p = .027.
Analysis included only females.
The number of patients continuing to the maintenance period was higher in the 0.5/1.0/1.2 mg/kg/day group than in the 0.5/1.2 group (98 [72.6%] and 80 [60.6%], respectively), but failed to reach statistical significance (p = .051). Lack of efficacy leading to discontinuation during the 8-week acute treatment period was slightly (but not significantly) higher in the 0.5/1.2 mg/kg/day group compared with the 0.5/1.0/1.2 mg/kg/day group (5 [3.8%] and 1 [0.7%], respectively; p = .117). The lack of efficacy was similar in both groups during the maintenance period (5 [5.7%] and 6 [6.7%] in 0.8 mg/kg/day and the 1.4 mg/kg/day group, respectively, p > .999) in patients who were compliant.
A decrease in weight of ≥3.5% compared with baseline was reported by 16.5% of patients during the 8-week acute treatment period (15.9% and 17.2% in the 0.5/1.2 and 0.5/1.0/1.2 mg/kg/day groups, respectively; p = .868). However, weight loss occurred in only 7.9% of patients during the maintenance treatment period (7.3% and 8.4% in the 0.8 mg/kg/day and 1.4 mg/kg/day groups, respectively; p = .999). There was no significant change in vital signs between the groups.
Discussion
Several clinical studies have demonstrated the benefit of atomoxetine maintenance therapy (Buitelaar et al. 2007; Hazell et al. 2006; Michelson et al. 2004; Newcorn et al. 2006; Wilens et al. 2006). In a multicenter study in children and adolescents who responded to an initial 12-week, open-label atomoxetine treatment, randomization to continued treatment with atomoxetine or placebo for an additional 9 months demonstrated that atomoxetine was superior to placebo for maintaining the initial response (Michelson et al. 2004). Additionally, in a randomized, double-blind study in children and adolescents who completed 1 year of treatment with atomoxetine, continuation of double-blind treatment for 6 additional months demonstrated superior outcomes compared with placebo (Buitelaar et al. 2007).
In the present study, results indicated that the majority of the improvement in ADHDRS total scores was achieved during the acute treatment period. Results from the ADHDRS subscale scores demonstrated that there was a significant loss of benefit in hyperactivity/impulsivity scores during the maintenance treatment with the 0.8 mg/kg/day dose but not with 1.4 mg/kg/day dose. Inattention scores increased, indicating a loss of benefit, in both treatment groups. The CGI-ADHD-S scores were maintained in the 1.4 mg/kg/day dose group compared with a loss in the 0.8 mg/kg/day group and the difference between the groups was significant suggesting the benefit of a higher dose.
Analyses from other secondary measures such as the LPS-C score, FAM-III overall rating t-score, and WJ-III Total Achievement scores suggested that although the majority of the benefit was achieved during the acute treatment period, long-term maintenance may be necessary to maintain the treatment benefits. Importantly, poor academic performance has been demonstrated with greater frequency in adolescents with ADHD (Barkley et al. 2006). In the present study, an improvement in mean grades for English, Math, Science, and Social Studies was demonstrated at the end of the maintenance treatment period in the 0.8 mg/kg/day group, although the improvement was statistically significant for Math only. Grades improved from C's to C+'s and B-‘s. Although not statistically significant, in the 1.4 mg/kg/day group, mean grades improved from C+ to B- for English, C to B- for Math, and C+ to B- for Social Studies, and decreased from B- to C+ for science.
The results during the 8-week acute treatment period indicate that patients who received the fast titration dosing schedule did not differ from those who received the slow titration in safety and tolerability measures at the 4-week time point. The results during the maintenance period suggest that 1.4 mg/kg/day is equally tolerable and may be necessary to maintain long-term control of ADHD symptoms. Although there was a small loss in weight during the acute treatment period, there was a small gain in weight at the end of the maintenance period. Moreover, there was no statistically significant difference in change in height from baseline to the end of the study between the two treatment groups.
One of the limitations of this study is the lack of a placebo control group during the long-term maintenance period. However, because of the extended length of the maintenance period, ethical considerations prevented the inclusion of a placebo control group. The WJ-III was completed at baseline, at the end of the acute period, and at the end of the maintenance period. It is possible that some of the change in scores can be attributed to practice effect. Because of slow enrollment, patient recruitment ended before reaching the planned number of patients, but all enrolled patients were allowed to complete the study. Despite having fewer patients than expected, variability of the ADHDRS change scores was less than predicted, resulting in sufficient power. Therefore, it is unlikely that the conclusions would be different had the study enrolled the number of patients originally planned. In addition, the measurement of GPA was performed at week 0 and the end of the maintenance treatment period. Therefore, a definitive conclusion cannot be drawn as to whether most of the improvement in academic learning occurred during the acute treatment period or as a result of maintenance treatment. Despite these limitations, the results indicate that a 1.4 mg/kg/day atomoxetine maintenance dose provides better control of ADHD symptoms over the long-term compared with 0.8 mg/kg/day.
Conclusion
This study demonstrates that benefit achieved after 8-weeks of acute atomoxetine treatment was maintained with continued atomoxetine treatment for 40 additional weeks in adolescent patients with ADHD. The benefit achieved during the acute treatment period was better maintained during maintenance treatment with 1.4 mg/kg/day compared with 0.8 mg/kg/day. Moreover, improvement in adaptive functioning and age-appropriate developmental function, including academic achievement was also demonstrated. Atomoxetine 0.8 mg/kg/day and 1.4 mg/kg/day were equally well tolerated in these patients. Having a slower titration schedule did not increase tolerability or decrease efficacy compared with a faster titration schedule. Data from this study do not support using a titration schedule that is slower than the one recommended in the atomoxetine label.
Footnotes
Disclosures
Ms. Wietecha, Mr. Williams, and Dr. Schuh are employees and minor shareholders of Lilly USA, LLC, a wholly-owned subsidiary of Eli Lilly and Company. Mr. Herbert was compensated by Eli Lilly and Company for training investigators to use the Woodcock Johnson-III Tests of Achievement. Dr. Melmed receives research support from, or has been a speaker for, Shire, Eli Lilly and Company, McNeil Pharmaceutical, Bristol-Myers Squibb Company, Novartis Pharmaceuticals, Neuropharm, and BioMarin. Dr. Greenbaum serves as a clinical investigator for Eli Lilly and Company, Shire, Novartis, Pfizer, Takeda Pharmaceutical Company, AstraZeneca, Abbott Laboratories, and Johnson and Johnson, and is on the Novartis Speaker Board.
Acknowledgments
The authors thank Anoop K. Padival, Ph.D. and Charlene Potter for their assistance with this manuscript.
This research was funded by Lilly USA, LLC, a wholly-owned subsidiary of Eli Lilly and Company.