
Abstract
Objective:
The purpose of this study was to investigate the effect of sertraline (SRT) in children and adolescents with obsessive-compulsive disorder (OCD) who did not respond to two consecutive courses of cognitive-behavior therapy (CBT).
Methods:
Observational study with 11 participants (males, n=6), 7–17 years of age with Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) primary OCD. All had received 14 plus 10 sessions of CBT over the course of 218–532 days (mean=342.2, SD=85.5). Outcome measures were mean reduction of the Children's Yale-Brown Obsessive Compulsive Scale (CY-BOCS) total score and adequate clinical response (CY-BOCS<16). All participants received SRT (maximum dose 200 mg/day). The study was a part of the Nordic Long-Term OCD Treatment Study (NordLOTS).
Results:
Participants were treated with SRT over 72–300 days (mean=164.2, SD=68.3). The mean CY-BOCS score was reduced from 21.5 (SD=2.6) to 17.5 (SD=3.3). Only three participants obtained adequate clinical response (27.2%), and only two obtained >25% CY-BOCS total score reduction (close to 50%).
Conclusions:
A clinical response in approximately one third of the participants suggests that SRT treatment might be beneficial to a minority of patients who have consistently failed CBT.
Introduction
O
Expert guidelines recommend cognitive behavior therapy (CBT) as the first-line treatment for mild to moderate pediatric OCD and a combination of CBT and selective serotonin reuptake inhibitors (SSRI) for moderate to severe OCD (Geller and March 2012). A combination of CBT and SSRI is also recommended if a clinical response is not achieved after several months of CBT (Geller and March 2012). However, the sequence implicated in these guidelines is primarily based on expert consensus and not on empirical evidence. In addition, clinically useful details, for example how many sessions of CBT should be provided before it is considered failed, are lacking.
This gap in the literature was one of the reasons that led to the establishment of the Nordic Long-Term OCD Treatment Study (NordLOTS), which is based on a stepped care model with three consecutive steps (Thomsen et al. 2013). In the first step, 269 youth with OCD were included in weekly exposure-based CBT for 14 weeks (Torp et al. 2015). In the second step, those with inadequate response to the CBT, defined as a score ≥16 on the Children's Yale-Brown Obsessive Compulsive Scale (CY-BOCS), were randomized to either continued CBT or sertraline (SRT). Because both treatments for nonresponders were effective with high within-group effect, there was no between-group difference on the CY-BOCS at posttreatment (Skarphedinsson et al. 2015). Participants who had been randomized to continued CBT without obtaining adequate response (CY-BOCS<16) could be considered to be truly treatment refractory to CBT (e.g., Krebs et al. 2015), as CBT in the NordLOTS study was carefully monitored, and high treatment fidelity observed (Torp et al. 2015). To this group of CBT-refractory young patients, SRT treatment was offered using the same drug treatment protocol as for patients randomized to SRT in Step 2.
The aim of this study was to assess SRT treatment response in CBT-refractory patients who did not respond to two consecutive courses of CBT.
Methods
Design and participants
The NordLOTS is a multinational, stepwise trial designed in part to evaluate the relative efficacy of continued CBT versus SRT among children and adolescents 7–17 years of age with OCD who were nonresponders to an initial course of individual CBT. Participants were offered 14 sessions of weekly individual exposure-based CBT as the first step of clinical care (Step 1). Nonresponders were randomized to two alternative treatments (Step 2): 1) Continued CBT for an additional 16 weeks or 2) treatment with SRT. In our protocol, all patients that relapsed after an initial response to Step 1 were offered continued CBT (or SRT if they refused further CBT). All patients who did not respond adequately to continued CBT in Step 2 were offered SRT treatment. In addition, patients who relapsed after an initial response to Step 2 CBT were offered SRT.
Of the 269 participants included in the NordLOTS, the 11 participants who had not obtained an adequate response (CY-BOCS<16) after Steps 1 and 2 (14+10 sessions CBT) or relapsed during follow-up were included in this study (see Fig. 1). Further details of the NordLOTS are described elsewhere (Thomsen, et al. 2013; Torp, et al. 2015).
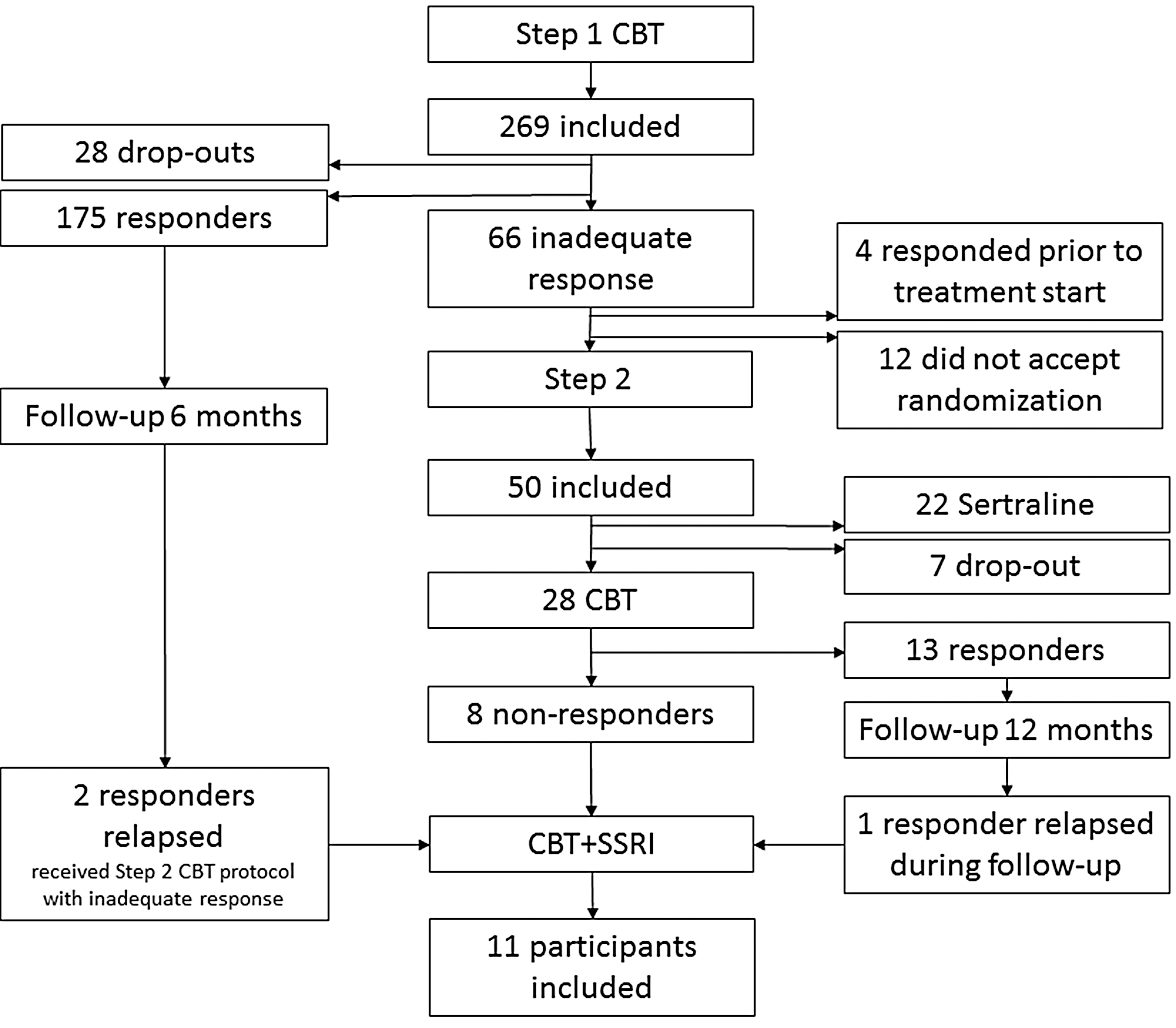
Consolidated Standards of Reporting Trials (CONSORT) flow chart.
Measures
The Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime (K-SADS-PL) (Kaufman et al. 1997) is a semistructured diagnostic interview that assesses a variety of childhood psychopathologies and demonstrates favorable psychometric properties as will be detailed subsequently. The K-SADS-PL has shown an excellent interrater reliability of 98% and a 1–5 week test–retest κ of 0.80 for any anxiety disorder diagnosis (Kaufman et al. 1997). Symptoms can be classified as “not present,” “possible,” “in remission,” or “certain.” In this study, OCD diagnoses and comorbidity were based on symptoms classified as “certain” only. The K-SADS-PL was used for diagnostic assessment at the baseline of Step 1. All interviews were conducted by experienced clinicians, trained by the NordLOTS research group.
The CY-BOCS (Goodman et al. 1989) is a widely used clinician-rated, semistructured interview assessing OCD symptomatology. It evaluates the severity of obsessions and compulsions using 10 items across five dimensions (time occupied by symptoms, interference, distress, resistance, and degree of control over symptoms). The total severity score can range from 0 to 40. The CY-BOCS shows reasonable reliability and validity (Scahill et al. 1997; Storch et al. 2004; Gallant et al. 2008), and in particular high internal consistency (0.87) for the total score and good to excellent interrater agreement (0.84, 0.91, and 0.68 for total score, obsessions, and compulsions, respectively) have been reported (Scahill et al. 1997). In the NordLOTS sample, the interrater agreement was 0.92 (95% CI 0.78–0.97), 0.94 (95% CI 0.85–0.97), and 0.87 (95% CI 0.67–0.93) for total score, obsessions, and compulsions, respectively.
Parental psychopathology was assessed by asking parents about their psychiatric symptoms and diagnosed psychiatric disorders.
Procedure
SRT was chosen because it is the only approved SSRI for OCD treatment in adolescents and children as young as 6 years of age in all three countries (Denmark, Sweden, and Norway) (Thomsen et al. 2013) and it has proved to be equally effective as the other SSRIs (Geller and March 2012). The pharmacotherapy treatment manual was adapted to Nordic conditions from the manual used in the Pediatric OCD Treatment Study (POTS) study (2004). A starting dose of 25 mg per day was titrated up to 100 mg per day by week 4; children <10 years of age with low weight could be started on a lower dose if deemed necessary. If response was considered inadequate at a dose of 100 mg, the dose was increased gradually up to a maximum of 200 mg per day by week 8. Treatment response and adverse events were monitored at every visit and the dose was reduced if necessary. The manual included guidelines for clinical support where participants were encouraged to practice exposure tasks learned during Step 1. However, introducing new exposure tasks by the therapist was not allowed. The rationale for this component was to reduce the variability of treatment effects unrelated to SRT. Pharmacotherapists were required to use a standardized script and were instructed to ask child and parent(s) 1) about resistance to compulsions, 2) about activities the child will engage in once the child improves, 3) whether the child actively uses treatment techniques learned during Step 1, 4) whether the child has engaged in exposures and the resulting outcome, 5) to encourage the child to continue to conduct exposures and to not engage in avoidance or rituals; and 6) to inquire and address any concerns related to the medication that the family may have.
Statistics
All descriptive statistical procedures were performed with SPSS, version 22.0.
Results
Patient characteristics
Eleven patients participated in the study, with eight having received 14 and 10 sessions of CBT in Steps 1 and 2, respectively, without achieving adequate response. Consequently, they were offered SRT treatment according to the protocol. Although one participant achieved adequate symptom reduction after Step 2 CBT, a 12 month follow-up revealed that he had experienced relapse. He was then offered SRT treatment as well. Two Step 1 CBT responders experienced relapse at 6 month follow-up. Consequently, they received a second course of 10 CBT sessions according to Step 2 protocol, but did not show adequate response, and were, therefore, switched to SRT (see Fig. 1).
Table 1 reports descriptive data for each patient. Six participants (55%) were boys. Mean age of the sample was 13.4 (SD=3.0). The current sample had a slightly higher mean age than the Step 1 sample (n=269, mean=12.8, SD=2.7). Only three patients (27%) lacked a comorbid disorder in comparison with 59.5% (n=160) in the Step 1 sample (n=160, 59.5%). Of the remaining eight patients, four had comorbid anxiety disorder, three had tic disorder, two had ADHD, and one had comorbid major depressive disorder (MDD). The most common OCD symptoms were cleaning compulsions and contamination obsessions (n=9).
Based on the Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime (K-SADS-PL).
OCD, obsessive-compulsive disorder; PTSD, posttraumatic stress disorder; ADHD, attention-deficit/hyperactivity disorder.
Treatment outcome
All CY-BOCS total scores before and after CBT and SRT are reported in Table 2. For the CBT effect, the mean within change of the CY-BOCS total score was 6.2 and the within-group uncontrolled effect size of CBT was 0.89, adjusted for the fact that the two means were not independent (Morris and DeShon 2002). Patients 9 and 10 were initially Step 1 responders with CY-BOCS total scores of 4 and 12, respectively. However, they experienced relapse and had CY-BOCS total scores of 26 and 22, respectively, 6 months after treatment. Therefore, they were treated with the 10 additional sessions of CBT according to Step 2 protocol without achieving adequate symptom reduction. Patient 8 had been randomized to Step 2 CBT and was a responder at posttreatment assessment. However, the patient relapsed during follow-up and was treated with SRT. Most of the patients started SRT treatment within 4 weeks after CBT termination. Four patients started SRT after >4 weeks and were reassessed with the CY-BOCS before SRT treatment. The mean within change of the CY-BOCS total score during the SRT treatment was 4.0 and the within-group uncontrolled effect size was 1.07. Only three participants (27.2%) obtained a score <16 on the CY-BOCS, with two of them (6 and 9) achieving almost 50% symptom reduction during SRT treatment. However, most of the remaining patients achieved little or no symptom reduction.
SRT baseline score same as post-CBT.
Selective serotonin reuptake inhibitor (SSRI) treatment was offered immediately after failure of the second CBT course, delay caused by patients' reluctance to start with medication or caused by time before relapse after initial response to CBT.
Based on≥28 days only.
CY-BOCS, Child Yale-Brown Obsessive Compulsive Scale; CBT, cognitive-behavior therapy; SRT, sertraline.
The most frequent adverse events were cognitive/psychiatric effects (n=4) and gastrointestinal effects (n=3). No serious adverse events were reported. One patient experienced moderate suicidal ideation in the starting phase of the SRT treatment, which he reported in one visit only. The same patient also reported behavioral activation, which caused extensive problems. Consequently, the dose of SRT was increased very carefully to a final dose of only 125 mg per day. The final mean dose of SRT for the full sample was 150 (SD=41.5) mg per day.
Discussion
Current guidelines recommend adding a SSRI (Geller and March 2012) or switching to an SSRI (National Institute for Heath and Clinical Excellence 2005), if CBT does not work. However, these recommendations are based on clinical experience and not on empirical research. In general, very little has been published about CBT-treatment-resistant patients. Although the current study is limited in terms of sample size and the observational design, it is the first study that reports on the effect of SSRI in patients who have failed two consecutive CBT trials. Our main results show that switching to SRT caused a mean improvement of 4 points on the CY-BOCS, which corresponds to a high within-group effect size (1.07). Although the uncontrolled total effect size of the SRT treatment was large, it was predominantly attributed to the two patients with close to 50% symptom reduction. Only these two and one additional patients with 18% symptom reduction achieved a score below our predefined cutoff of 16 points on the CY-BOCS. The remaining patients achieved a mean reduction of 10% with none experiencing >25% reduction. This indicates that SRT treatment might be beneficial to a small minority of patients who have consistently failed CBT. However, a larger randomized controlled trial is needed in order to generalize the results and to predict which therapy will lead to good treatment outcomes for certain patients.
The two patients (6 and 9) who achieved the highest symptom reduction had several common features. Both had a relatively low pre-CBT CY-BOCS total score of 21 and achieved no symptom reduction after CBT. During the SRT treatment, both had gastrointestinal adverse events. The patients who responded the least to SRT (numbers 1, 2, 4, and 8) all had severe OCD at CBT baseline and some improvement after CBT, leading to moderate OCD at SRT baseline. All had a comorbid disorder (anxiety or ADHD), contamination fear, and were titrated up to mean or maximum daily doses of SRT.
Our data, suggesting that some nonresponders to two CBT trials may benefit from SSRIs, are in line with current guidelines (Geller and March 2012). SSRIs should be offered to all pediatric patients who have failed CBT, although it is not clear how many sessions of CBT are needed before it is necessary to add an SSRI. The only trial on CBT nonresponders is the NordLOTS Step 2 trial, which indicated that patients with inadequate response (after 14 weeks) who still had moderate to severe OCD could expect some improvement whether they would continue their CBT with 10 additional sessions or switch to SRT (Skarphedinsson et al. 2015). One possible interpretation is that patients, who despite compliance and a certain treatment progress have not responded adequately after 14 sessions of CBT, should be given more CBT sessions before adding or switching to SSRI.
We report an outcome after a mean of 164 (SD=68) days of SRT treatment. It is possible that some of the subjects may experience additional improvement with longer SRT treatment. It does not seem to be effective to discontinue SSRI treatment after the acute treatment phase, as one can expect a high relapse rate (50% in one study [Asbahr et al. 2005]). SSRI treatment has been documented to be increasingly effective up to 1 year. One study showed substantially better response (55% remitters) in those who completed SRT treatment up to 1 year. However, as many dropped out (53%) and many others had serious adverse events, it is still not clear whether the benefit of long-term SRT treatment outweighs the risks (Cook et al. 2001; Wagner et al. 2003). In addition, no known predictors of outcome exist that can assist clinicians in evaluating which group will benefit from medication in the long term.
It is difficult to generate hypotheses based on our limited data. However, future studies may focus on neurochemical or pharmacodynamic differences among patients (Hanna et al. 1993; Rosenberg et al. 2000). Investigating genetic variation may also be beneficial. For example, allelic variation of the serotonin transporter gene and concomitant morphological changes may moderate individual response to SSRIs (e.g., Serretti, et al. 2005). Further, the synergistic effects between CBT and SSRI need to be investigated. According to the medication protocol, patients were encouraged to engage in exposure exercises they had previously learned during CBT sessions (but no new exposures were initiated by the therapists). SSRIs may have mediated better CBT outcomes, at least in some patients, by improving their tolerance for exposure and response prevention. An important goal is to develop assessment procedures identifying the likelihood of one or the other treatment response, allowing individualized treatment choices based on patient characteristics, including relevant genetic variations.
Conclusions
The strength of our study is the stepped care design. We have followed all patients for >1 year since their inclusion in Step 1 and evaluated their OCD symptoms regularly. In addition, state of the art measures were used to evaluate OCD symptoms and comorbidity. Therefore, this is the first study that reports the effect of SSRIs after two thorough CBT trials. However, the limitation is the small number of patients and the observational design used to evaluate the effect. Therefore, it is necessary to conduct a larger randomized controlled trial to generalize the results. However, that will require extensive funding and the cooperation of a plethora of sites in many countries.
Clinical Significance
The data suggest that SSRIs may be effective for a minority of patients who still have moderate to severe OCD after 24 sessions of CBT. However, further studies are needed to generalize the results.
Footnotes
Disclosures
Dr. Ivarsson is consultant and member of the speaker's bureau for Shire, Sweden. The other authors have nothing to disclose.