
Abstract
Objective:
The youngest children in a classroom have a higher risk of attention-deficit/hyperactivity disorders (ADHDs) and depression than their relatively older peers. However, there has been a lack of research on how relative age is related to second-generation antipsychotic (SGA) medication use.
Methods:
This study used the Finnish National Prescription Register data and comprised all 669,726 Finnish children and adolescents aged 7–17 in 2018. We extracted data for those who were dispensed SGAs (risperidone, quetiapine, aripiprazole, and olanzapine) and ADHD medication (methylphenidate, atomoxetine, dexamphetamine, and lisdexamfetamine). Odds ratios (OR) and 95% confidence intervals (CI) were calculated for medication dispensed to schoolchildren born from January to April (the relatively oldest), May to August, and September to December (the relatively youngest). Dispensed prescriptions were a proxy for medication use.
Results:
SGAs were dispensed to 9146 (1.4%) individuals in 2018. Their use was lower among girls aged 12–17 years born from September to December than January to April (OR 0.89; 95% CI 0.83–0.97), with no association between SGA use and birth month among boys. However, younger relative age was associated with combined SGA and ADHD medication, which was used by 2556 (0.4%) of the cohort: 2074 (0.6%) boys and 482 (0.1%) girls. The OR was 1.27 for boys aged 12–17 born from September to December (95% CI 1.10–1.46), compared with January to April. The OR for girls born from May to August was 1.35 (95% CI 1.04–1.76) and from September to December it was 1.33 (95% CI 1.02–1.74), compared with January to April.
Conclusions:
A novel discovery of this study was that using both SGA and ADHD medication at the age of 12–17 years was more common among the youngest subjects in a school year than their relatively older peers.
Introduction
Over the last decade, many studies have associated younger relative age within a school year with an increased risk of being diagnosed with, and medicated for, attention-deficit/hyperactivity disorder (ADHD) (Sayal et al. 2017; Caye et al. 2019; Whitely et al. 2019). The reported risk was about 30%–40% higher in the youngest, than oldest, children in a classroom (Caye et al. 2019; Whitely et al. 2019). Swedish and Finnish population-based studies have shown that the relative age effect was stronger in children during their early school years (Halldner et al. 2014; Brikell et al. 2016; Sayal et al. 2017; Vuori et al. 2020). Other studies have demonstrated that the effect of having a birthday late in the school year peaked in the fourth and fifth grades when the children were 10–11 years of age (Whitely et al. 2019). In general, empirical evidence has indicated that relative age plays a more important role in middle childhood in patients with ADHD (Halldner et al. 2014; Sayal et al. 2017; Whitely et al. 2019). The prevalence of ADHD medication use varies significantly across countries (Raman et al. 2018). However, studies of countries with low prevalence rates have shown that the relatively youngest children in a classroom face an increased risk of being medicated than their relatively older peers (Whitely et al. 2019).
Prescribing second-generation antipsychotic (SGA) medication to children and adolescents has been increasing in a number of countries (Hartz et al. 2016; Nesvåg et al. 2016; Sultan et al. 2019; Varimo et al. 2020). Some SGAs are prescribed to treat psychotic disorders and symptoms. However, drugs such as risperidone, quetiapine, aripiprazole, and olanzapine are frequently prescribed to pediatric patients without authorized indications (Penfold et al. 2013; Hálfdánarson et al. 2017; Varimo et al. 2020). SGAs have shown short-term efficacy in treating acute mania and extreme mood variability (Scherk et al. 2007; Zuddas et al. 2011). Risperidone and aripiprazole may reduce irritability and aggression in patients with disruptive behavior disorders or neurodevelopmental conditions (Zuddas et al. 2011; Loy et al. 2017; Fallah et al. 2019). Quetiapine monotherapy may reduce the symptoms of uncomplicated generalized anxiety disorder (LaLonde and Van Lieshout 2011).
The most common SGAs prescribed for children and adolescents are risperidone and quetiapine (Rettew et al. 2015; Nesvåg et al. 2016; Hálfdánarson et al. 2017). Studies have shown that the use of SGAs is more common among adolescents than children (Olfson et al. 2015; Edelsohn et al. 2017; Varimo et al. 2020). One study reported that the annual prevalence was also higher in adolescents than young adults (Sultan et al. 2018). Some studies have reported that SGAs were more commonly prescribed for boys than girls (Olfson et al. 2015; Hartz et al. 2016). However, other studies published during the same period reported that the prevalence of SGA use was higher in girls than boys (Hartz et al. 2016; Kloosterboer et al. 2018). A recent population-based study found that the use of SGAs increased among children and adolescents in Finland during the 2010s, with a steeper increase in girls than boys. The two most commonly used SGAs in Finland were quetiapine and risperidone (Varimo et al. 2020). Another population-based study from the same team found that the mean treatment duration of SGAs among Finnish children and adolescents was relatively long (Varimo et al. 2021). Initiating SGA treatment with risperidone was associated with a notably longer treatment duration, whereas initiating SGA treatment with quetiapine, along with older age, was associated with discontinuing the treatment earlier (Varimo et al. 2021).
ADHD has been strongly related to SGA use among boys, and anxiety and depression among girls (Olfson et al. 2015; Nesvåg et al. 2016; Edelsohn et al. 2017; Sultan et al. 2019; Rodrigues et al. 2020). Most SGAs are used with other psychotropic medication, such as those prescribed for ADHD (Kreider et al. 2015; Scholle et al. 2018). This combined use in adolescents may relate to a lack of effective strategies to treat irritability and aggression in this population (Loy et al. 2017; Faraone et al. 2019; Baker et al. 2021). The reasons for the increased use of SGAs in Finland are not well understood. In general, they are being prescribed almost exclusively for off-label indications among children and adolescents (Varimo et al. 2020, 2021). Previous studies suggest that one of the common reasons for prescribing risperidone has been aggressive behavior. Meanwhile, the increased use of quetiapine may stem from the fact that it is prescribed for short-term monotherapy of anxiety and insomnia or concurrently with an antidepressant for adolescent depression (Varimo et al. 2021).
To the best of our knowledge, no studies have been published that examined whether the relatively youngest children and adolescents in classes faced an increased risk of being prescribed SGAs. Although studies on relative age and ADHD have demonstrated stronger effects in children than adolescents (Halldner et al. 2014; Sayal et al. 2017), the phenomenon has been shown to persist into adolescence (Halldner et al. 2014; Brikell et al. 2016). One study discovered that the relatively youngest adolescents in a cohort had higher suicide rates (Matsubayashi and Ueda 2015). The relative immaturity of children has also been linked with an increased risk of being diagnosed with depression (Root et al. 2019). Depressive disorders are more likely to emerge many years after the onset of other disorders, such as ADHD. This means that relative immaturity could elicit stressful environmental exposure as children with such disorders grow older (Riglin et al. 2020). Gender differences may also occur. The association between younger relative age and the use of ADHD medication tends to be more prominent in Finnish girls than boys, despite the fact that its use is significantly more common among boys (Vuori et al. 2020). Because SGA use is more common among adolescents than children, there is also a need to examine the association between birth month and SGA medication use from childhood to adolescence.
The aim of this study was to investigate the extent to which relative age, measured using an individual's birth month, was associated with the use of SGA and ADHD medication by Finnish children and adolescents. We also examined whether this association was moderated by the concurrent use of SGAs and ADHD medication. Many studies have reported that the relatively youngest children and adolescents in cohorts had an increased risk of outcomes related to mental disorders. That is why we hypothesized that the relatively youngest subjects in school classes would have an increased risk of being prescribed SGAs and that this association would be moderated by the concurrent use of ADHD medication.
Methods
Study setting, population, and medication data
The study population comprised all 669,726 Finnish children and adolescents aged from 7 to 17 years in 2018. Permanent Finnish residents are covered under the Finnish National Health Insurance system and SGAs and ADHD medication prescribed by a doctor can be reimbursed. Drug reimbursements are recorded in the Finnish Prescription Registry, which is maintained by the Social Insurance Institution of Finland. In this study, the reimbursed prescriptions that were dispensed were used as a proxy for use.
Medication is coded in the Finnish Prescription Registry, according to the Anatomical Therapeutic Chemical (ATC) classification system. We extracted data on the individuals who received reimbursements for the most commonly used SGA and ADHD medication between January 1 and December 31, 2018. The SGAs comprised risperidone, quetiapine, aripiprazole, and olanzapine, and the ADHD medications were methylphenidate, atomoxetine, dexamphetamine, and lisdexamfetamine. Concurrent use was defined as at least one reimbursed purchase of an SGA and at least one ADHD medication during 2018. The prevalence of medication use was defined as the number of patients aged 7–17 who had at least one reimbursed purchase of SGA or ADHD medication compared with the number of children in that age group in the total population. The prescription register also included data on the patient's gender and date of birth.
Prescribing indications are not available in the Finnish Prescription Registry. In Finland, the authorized indication for prescribing risperidone is aggressive behavior in intellectually disabled people who are at least 5 years of age for no more than 6 weeks. However, SGA medication use by children younger than 7 years, when children start their 9-year compulsory basic comprehensive school education, is very rare (Varimo et al. 2020, 2021). School years are the most important developmental stage, from a relative age perspective (Whitely et al. 2019). That is why children aged 5–6 years of age were removed from the analyses. There is a specific code for special refunds due to intellectual disability in the Finnish Prescription Registry. In our data, only 225 individuals (189 boys and 36 girls) fell into this category. Aripiprazole is authorized for treating schizophrenia in adolescents aged 15 and older, but there are no authorized indications for prescribing quetiapine or olanzapine for those younger than 18.
Relative age
Finnish children start their first school grade in August in the calendar year that they celebrate their seventh birthday and the cutoff date is December 31. This means that the relatively oldest children are born in January and the relatively youngest children are born in December. We classified the subjects into three groups based on the month they were born in, in common with previous studies (Caye et al. 2019). The relatively oldest were born from January to April, the middle group was born from May to August, and the relatively youngest were born from September to December. Compulsory education in Finland ends at the age of 16, but 97.0%–97.5% of children choose to continue their studies immediately after that age (Statistics Finland). This means that most of the subjects in our study would still have been in education for the whole period covered by the data analysis.
Statistical analyses
First, we examined the descriptive statistics of the prescribing patterns for SGAs and ADHD medication by gender using 1-year age intervals from 7 to 17. The association between relative age and medication use among children and adolescents was analyzed by binary logistic regression. Due to notable differences in SGA and ADHD medication use by age and gender, we analyzed the data separately by gender using two age groups: 7–11 and 12–17 years. These age ranges were chosen because medication use, particularly among girls, increases at age 12 and when they are entering youth services. We calculated the odds ratios (OR) with 95% confidence intervals (CI). The basic model just examined the use of SGAs. The adjusted model analyzed the extent to which the association between birth month and the use of SGAs was moderated by ADHD medication within the calendar year. This means that the interaction effect was included in the adjusted model. Medication users were defined as subjects who had been dispensed at least one prescription for both SGA and ADHD medication during 2018. We carried out a sensitivity analysis, by examining the association between relative age and SGA medication use and excluding those individuals who had also used ADHD medication. All the analyses were performed using SPSS version 25 (IBM Corp, NY, USA) and the R tidyverse and ggplot2 packages (R Foundation, Vienna, Austria).
Ethical considerations
According to national regulations, our register-based study did not require ethical approval. The Social Insurance Institution approved the study protocol.
Results
Medication by gender
The study population comprised 9146 Finnish children and adolescents aged from 7 to 17 who had been dispensed at least one prescription for SGA medication in 2018. This figure represented 1.4% of the general population of 669,726 subjects aged 7–17 in that year. When it was broken down by gender, there were 4968 (1.4%) boys and 4277 (1.3%) girls. The corresponding percentages for boys aged 7–11 and 12–17 were 1.0% and 1.8% of the total cohort, respectively. Based on the 1-year age intervals, the use of SGA medication ranged from 0.4% to 1.4% for boys aged 7–11 and 1.5% to 2.2% for those aged 12–17 (Fig. 1). When it came to the girls, the prevalence of SGA use was notably lower among those aged 7–11 (0.0%–0.5%) than those aged 12–17 (0.6%–4.0%). Detailed descriptive statistics for SGA and ADHD medication use are presented in Supplementary Table S1. Overall, 2556 (0.4%) of the cohort used both SGA and ADHD medication in 2018: 2074 (0.6%) boys and 482 (0.1%) girls.
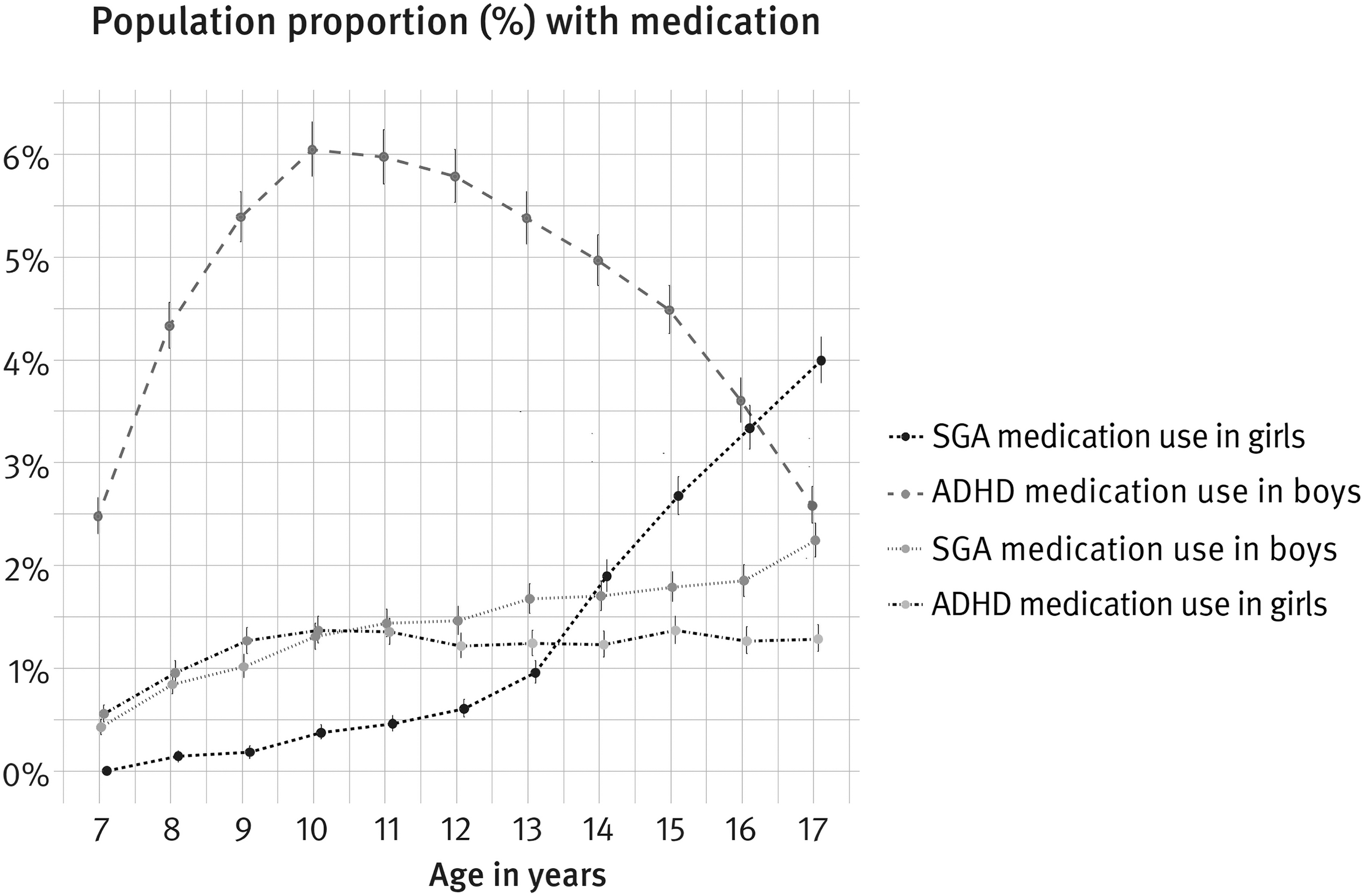
The use of SGA and ADHD medication among Finnish pediatric patients aged 7–17 years in 2018 (N = 669,726). ADHD, attention-deficit/hyperactivity disorder; SGA, second-generation antipsychotics.
The use of ADHD medication was notably more common among boys than girls as a percentage of the total cohort (4.7% vs. 1.2%) (Fig. 1). The analysis by 1-year age intervals showed a relatively large variation in ADHD medication use among boys (range 2.5%–6.0%), but less variation in ADHD medication use among girls (range 0.6%–1.4%). ADHD medication use peaked among boys aged 9–13 (range 5.4%–6.0%). Figure 1 shows that boys did not use more SGA medication than ADHD medication at any age. SGA medication use exceeded the use of ADHD medication among girls aged 14–17. Risperidone was the most commonly prescribed SGA for boys and quetiapine for girls.
Relative age and SGA medication use by age and gender
Younger relative age was not related to SGA use among boys (Table 1). However, sensitivity analyses suggested that the association was attenuated by the use of ADHD medication. When we removed boys aged 7–11 years who used ADHD medication from the analyses, the relatively younger boys, who were born from September to December, had 0.81 times the odds (95% CI 0.67–0.97) of having used SGA medication than their relatively youngest classmates, who were born from January to April. Younger relative age was not associated with the use of SGA and ADHD medication by boys aged 7–11 either. However, the relatively younger boys aged 12–17, who were born from September to December, had 1.27 times the odds (95% CI 1.10–1.46) of having used both SGA and ADHD medication than the relatively youngest boys born from January to April. The percentage of boys aged 12–17 who had at least one prescription for SGAs and ADHD medication dispensed in 2018 ranged from 0.6% to 0.7% (Table 1). Table 1 shows that ∼40% of those boys who had at least one prescription dispensed for SGAs had also used ADHD medication during 2018. All these boys had used risperidone indicating that the reasons for SGA medication use were similar in this group.
The Association Between Birth Month and the Use of Second-Generation Antipsychotics and Attention-Deficit/Hyperactivity Disorder Medication by Boys (N = 342,319)
Bold figures indicate statistical significance. Table shows SGA (aripiprazole, risperidone, olanzapine, or quetiapine) and ADHD medication (methylphenidate, atomoxetine, dexamphetamine, or lisdexamfetamine), or both, dispensed in 2018. When subjects who used ADHD medication were removed, the ORs were: a0.86 (95% CI 0.72–1.03, p = 0.096); b0.81 (95% CI 0.67–0.97, p = 0.023) for those aged 7–11 and c0.93 (95% CI 0.83–1.03, p = 0.147); d0.95 (95% CI 0.85–1.05, p = 0.297) for those aged 12–17.
ADHD, attention-deficit/hyperactivity disorder; CI, confidence interval; OR, odds ratio; ref, reference category; SGA, second-generation antipsychotics.
Younger relative age was not related to SGA use among girls aged 7–11, but the association was attenuated by the use of ADHD medication (Table 1). However, the girls aged 12–17 who were born from September to December had 0.89 times the odds (95% CI 0.83–0.97) of having used SGA medication than the girls born from January to April. However, the use of both SGA and ADHD medication was higher among girls aged 12–17 born from May to August (OR 1.35, 95% CI 1.04–1.76) and September to December (OR 1.33, 95% CI 1.02–1.74), compared with the girls born from January to April.
The percentage of girls aged 12–17 who had at least one prescription for SGAs and ADHD medication dispensed in 2018 was 0.2% (Table 2). The girls in this group were more likely to have used quetiapine (around 60%) than risperidone (around 40%). This indicated that the reasons for SGA medication use in this group were more heterogeneous among girls than boys. Results from the binary logistic regression analyses for the total cohort are presented in Supplementary Table S2.
The Association Between Birth Month and the Use of Second-Generation Antipsychotics and Attention-Deficit/Hyperactivity Disorder Medication by Girls (N = 327,407)
Bold figures indicate statistical significance. Table shows SGAs (aripiprazole, risperidone, olanzapine, or quetiapine) and ADHD medication (methylphenidate, atomoxetine, dexamphetamine, or lisdexamfetamine), or both, dispensed in 2018. When subjects who used ADHD medication were removed, the ORs were: a0.74 (95% CI 0.55–0.99, p = 0.042); b0.76 (95% CI 0.57–1.03, p = 0.080) for those aged 7–11 and c0.97 (95% CI 0.89–1.05, p = 0.386); d0.86 (95% CI 0.79–0.94, p = 0.0004) for those aged 12–17.
ADHD, attention-deficit/hyperactivity disorder; CI, confidence interval; OR, odds ratio; ref, reference category; SGA, second-generation antipsychotics.
Discussion
This population-based register study found that boys aged 12–17 born from September to December, and girls born from May to August or September to December, were more likely to use both SGA and ADHD medication than their oldest peers, born from January to April. We also observed that just using SGA medication was not more common among the relatively youngest students, across genders, compared with their relatively oldest peers. Instead, we found that the use of SGA medication was actually lower in girls aged 12–17 who were born from September to December than January to April.
In this study, the use of SGA and ADHD medication referred to subjects aged 7–17 who had at least one reimbursed purchase of both types of medication during 2018. The fact that it was more common among the relatively youngest boys and girls aged 12–17 is a novel discovery. Previous studies had not examined the concurrent use of SGA and ADHD medication, but they had demonstrated close associations between ADHD and birth month. On average, the youngest children born in the last months of the calendar year were 30%–40% more likely to be diagnosed with ADHD and be prescribed with medication for that condition than older classmates born in the first months of the year (Whitely et al. 2019). Prior studies have also shown that the association between birth month and ADHD was stronger in middle childhood, but got weaker as children grew older (Halldner et al. 2014; Brikell et al. 2016; Sayal et al. 2017). Previous Finnish population-based studies indicated that the relative age effect of ADHD was more pronounced at 6–9 years of age (Sayal et al. 2017; Vuori et al. 2020).
Our findings were consistent with previous studies that showed that the concurrent use of ADHD and SGA medication was fairly common, particularly among boys (Scholle et al. 2018; Rodrigues et al. 2020). We found that risperidone was the most common SGA used by boys who also used ADHD medication. For the girls with ADHD with medication, the most common SGAs were quetiapine or risperidone. This finding indicates that the reasons for the concurrent use of ADHD and SGA medication were more heterogeneous among girls than boys. The reasons for SGA medication use in Finland have not been adequately researched. There has been speculation that one of the most common reasons for risperidone use has been for aggressive behavior, whereas quetiapine may have been used for anxiety or depression (Varimo et al. 2021). The combination of disruptive behavior disorders and depression is more likely to emerge many years after the onset of ADHD. Our novel finding indicates that a younger relative age may elicit stressful environmental exposure and increase the emotional and behavioral difficulties among boys and girls who are susceptible to ADHD in adolescence. Consequently, our study adds to the increasing empirical evidence about ADHD and relative age, by indicating that a younger relative age is not a seasonal factor. Instead, the observed association may reflect the contribution that social contexts play in the development, and increased the risk for adverse lifetime outcomes when boys and girls have an increased risk of being prescribed SGAs, due to co-occurring problems. It is important to acknowledge that our study did not measure the lifetime risk of using SGA and ADHD medication before the age of 18. Future research on relative age should take this into consideration.
We made an important discovery when we looked SGA use on its own. That was that the relatively younger girls aged 12–17, who were born in the last months of the calendar year, were less likely to use SGA medication than older peers born from January to April. First, this empirical finding implies that gender may play an important role in the association between relative age and medication use. For example, another recent population-based study discovered that the late birth date effect on ADHD medication use was more pronounced among girls than boys (Vuori et al. 2020). Second, researchers have suggested that the relatively youngest children in a class face a higher risk of mental disorders in middle childhood, due to differences in maturity. This theory is supported by the fact that the effect that relative age has on ADHD can be reduced by delaying the age when the relatively youngest children start school (Whitely et al. 2019). On the contrary, the more mature, relatively oldest children in a class may find it easier to mask their affective and behavioral difficulties. This line of thinking further suggests that the relatively oldest individuals could be more likely to display their symptoms later in adolescence. However, studies that have examined the role of relative age on various outcomes, such as ADHD and depression, have not reported increased odds or risks for the relatively oldest, than youngest, adolescents (Halldner et al. 2014; Root et al. 2019). Therefore, our novel finding is important, because it suggests that, on average, girls aged 12–17 who were born from January to April had an increased risk of mental disorders in adolescence than relatively younger peers. Anxiety and depression have been reported to be the most common diagnoses among girls who used SGAs (Nesvåg et al. 2016; Sultan et al. 2019). Studies have also found that emotional lability is a growing burden among adolescents with ADHD traits (Faraone et al. 2018).
Finally, our study also observed a large discrepancy in the use of SGA and ADHD medication by gender. Another study reported that many adolescents with ADHD did not receive stimulant medication before SGAs were initiated (Sultan et al. 2019). We speculate that the increased use of SGA medication by adolescent girls may partially relate to under-recognition of ADHD. Furthermore, our novel finding also suggests that the season of birth may also play an important role in the use of SGAs, as another study found that it was more commonly prescribed to children born in the winter months (Asano et al. 2016). These possible explanations are beyond the scope of our study, but they do highlight the value of widening mental health outcomes in research on the impact of relative age.
Strengths and limitations
The main strength of our study was the population-based design. We used the national Finnish prescription register data covering all reimbursed purchases of outpatient SGA and ADHD medication for children aged 7–17 in 2018. However, the subjects were only followed for 1 year and the amount of combined SGA and ADHD medication that was dispensed was somewhat low among boys and remarkably low among girls. Another study suggests that the cumulative proportion of individuals who used both SGA and ADHD medication before the age of 18 was probably larger than observed in our study (Scholle et al. 2018). In addition, our study did not include more detailed information from other national registers, such as mental health diagnoses. Therefore, the study findings should be considered tentative at best. The results should be independently replicated from representative national health registers. In addition, using child and adolescent self-ratings of the symptoms of mental disorder symptoms, combined with adult ratings, and linking them with national register-based data would increase our understanding of the reasons for SGA medication use. However, large population-based data with survey and register data linkage are not currently available.
Conclusion
This national Finnish register study found a modest association between younger relative age and increased SGA medication use in boys and girls aged 12–17 who had also been dispensed ADHD medication in 2018. In addition, SGA medication use was lower among relatively younger girls aged 12–17 who were born from September to December than peers born from January to April. These novel findings need to be independently replicated by other register-based studies.
Clinical Significance
The results suggest that at 12–17 years of age relatively younger boys born from September to December, and girls born from May to August and September to December, were slightly more likely to use both SGA and ADHD medication than older peers born from January to April. Our study highlights the need to widen mental health outcomes when carrying out relative age research and to look at the impact from a lifetime perspective.
Footnotes
Disclosures
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.