
Abstract
Objective:
To evaluate the comparative efficacy of pharmacological interventions for children and adolescents with a dual diagnosis of persistent tic disorders or Tourette disorder and attention-deficit/hyperactivity disorder (TD + ADHD).
Methods:
We searched CENTRAL, Embase, PubMed, PsycInfo, Web of Sciences, ClinicalTrials.gov, and WHO ICTRP up to September 2023 to identify double-blinded randomized controlled trials (RCTs) assessing pharmacological interventions for children and adolescents with TD + ADHD. Outcomes were change in ADHD symptoms (primary) and tics (secondary) severity. Standardized mean difference (SMD) was calculated and pooled in random-effects network meta-analysis. The Confidence in Network Meta-Analysis framework was adopted to determine certainty of evidence.
Results:
We included 8 RCTs involving 575 participants. Network meta-analyses demonstrated that α2 agonists (SMD, 95% confidence interval [CI] ADHD: −0.72 [−1.13 to −0.31]; TD: −0.70 [−0.96 to −0.45]) and stimulants + α2 agonists (ADHD: −0.84 [−1.54 to −0.13]; TD: −0.60 [−1.04 to −0.17]) were more efficacious than placebo for ADHD symptoms and tics severity. Stimulants alone were more efficacious than placebo for ADHD symptoms severity only, but they did not worsen tics (ADHD: −0.54 [−1.05 to −0.03]; TD: −0.22 [−0.49 to 0.05]). There were no significant differences between any pairs of medications that were found efficacious against placebo for ADHD symptoms or tics severity. Certainty in the evidence varied from low to very low.
Conclusions:
Stimulants are efficacious for ADHD symptoms severity and do not increase tics severity in TD + ADHD. α2 agonists are efficacious for both ADHD symptoms and tics severity in TD + ADHD. These findings should inform guidelines and help guide shared decision-making to choose a medication for children with TD + ADHD.
Introduction
Persistent tic disorders and Tourette disorder (here collectively referred to as TD) are neuropsychiatric conditions characterized by childhood-onset tics that persist for longer than one year and are associated with distress, functional interference, or both (Robertson et al., 2017). Clinical practice guidelines (CPGs) from the American Academy of Neurology (AAN) (Pringsheim et al., 2019) and the European Society for the Study of Tourette’s Syndrome (ESTSS) (Roessner et al., 2022) both recommend behavioral strategies, such as Comprehensive-Behavioral Intervention for Tics (CBIT) (McGuire et al., 2014), as a first-line intervention for the treatment of TD. Pharmacological treatment for tics is increasingly reserved as a second-line intervention for those who continue to experience tic-related distress or interference after psychotherapeutic intervention, or for those who lack access to, or are not suitable candidates for, psychotherapy. Evidence-based pharmacological treatment of tics currently includes several antipsychotics, such as risperidone and aripiprazole, and α2 agonists, such as clonidine and guanfacine (Farhat et al., 2023).
However, children with TD are often prescribed psychotropic medications for indications other than the tics themselves. Children and adolescents with TD, in particular Tourette Disorder, are more likely to have coexisting psychiatric disorders, including attention-deficit/hyperactivity disorder (ADHD). ADHD may be present in more than half of individuals with TD who reach clinical attention (Hirschtritt et al., 2015; Grados and Mathews, 2008; Khalifa and von Knorring, 2006), and it has been associated with poorer psychosocial functioning and increased internalizing and externalizing problems. In addition, comorbid ADHD may be a more important predictor of associated psychosocial and behavioral problems than tics severity in TD (Gorman et al., 2010; Lebowitz et al., 2012; Eddy et al., 2011; Hoekstra et al., 2004; Sukhodolsky et al., 2003). These data resonate with routine clinical practice showing that children and adolescents often do not perceive their tics as their most impairing symptom (Bloch and Leckman, 2009). Therefore, prompt, and effective, treatment of ADHD in children and adolescents with TD is imperative (Cohen et al., 2013).
There is some agreement across international CPGs that pharmacological interventions are an important component of the multimodal treatment plan for ADHD in school-aged children (ages 5–18 years) (Coghill et al., 2021; Cortese 2020). These recommendations are supported by robust evidence from ADHD randomized controlled trials (RCTs). Cortese et al. (2018) conducted a rigorous network meta-analysis with data from 81 double-blinded RCTs involving 14,346 children and adolescents with ADHD irrespective of comorbidity status and reported that methylphenidate and amphetamines led to the greatest reductions in total ADHD symptoms considering clinician, parent, or teacher reports. In children and adolescents, amphetamines were worse than placebo in terms of tolerability (defined as dropout rates due to side effects), whereas methylphenidate was not significantly different from placebo and was the only intervention to have better acceptability (defined as dropout rates due to any cause) than placebo. When treating an individual with ADHD in the context of TD, some practitioners may generalize from this larger literature that is less specific to patients with TD. However, others may prefer to rely on the available evidence that is directly related to this clinical subpopulation (Farhat and Bloch, 2021).
To date, there has been only one study investigating the effects of pharmacological treatments for ADHD in the context of TD (henceforth TD + ADHD) through meta-analyses of RCTs. In 2009, Bloch et al. (2009) included data from nine RCTs involving 477 individuals and reported that α2 agonists provided the best combined improvement in both ADHD symptoms and tics severity. Since then, the field has moved to recognize that network meta-analyses are essential to inform treatment guidelines as they provide estimates of the comparative effects of two or more interventions even when they have not been investigated in head-to-head RCTs (Leucht et al., 2016). Nevertheless, there are no network meta-analyses investigating the comparative effects of pharmacological interventions on ADHD symptoms and tics severity in individuals with TD + ADHD.
Our study aimed at addressing this gap by conducting a systematic review and network meta-analyses of pharmacological interventions evaluated for the treatment of TD + ADHD in double-blinded RCTs. We aimed to compare medications against placebo and each other in terms of change in ADHD symptoms and tics severity.
Materials and Methods
The procedures adopted in this study followed recommendations from the Cochrane Handbook. The study was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Network Meta-Analyses (PRISMA-NMA) (Hutton et al., 2015), and the checklist is provided in Supplementary Data S1 (Supplement 1). The protocol for this study was preregistered in PROSPERO (CRD42022370547).
Eligibility criteria and information sources
We included double-blinded RCTs that recruited children and adolescents (≤17 years) with a dual diagnosis of ADHD and TD according to any standardized criteria, including the Diagnostic and Statistical Manual (DSM), and that administered any pharmacological intervention at any dose for at least 1 week. We opted to exclude data about desipramine (Spencer et al., 2002; Singer et al., 1995) post hoc because of concerns with its safety in children and young people (e.g., cardiac arrest) (Werry et al., 1995) and hence their poor clinical applicability. We did not restrict eligibility based on RCT design (i.e., parallel or crossover), language, or publication year. We considered both published (including any type of publication) and unpublished studies eligible.
We searched five online databases (Cochrane Central Register of Controlled Trials, Embase, PsycInfo, PubMed, Web of Science) and two clinical trial registries (World Health Organization International Clinical Trials Registry Platform, ClinicalTrials.gov) from date of inception to September 29, 2023. Whenever possible, we adopted search filters from the Cochrane Handbook to identify RCTs. Search terms were tailored to each database and are provided in Supplementary Data S1 (Supplement S2). We also hand-searched the US Food and Drug Administration (FDA), European Medicines Agency, and relevant drug manufacturer’s websites, as well as references of previous systematic reviews and guidelines, to look for additional studies. On July 27, 2024, we also searched Google Scholar to identify additional eligible studies.
We contacted study authors to gather unpublished information and data, such as additional information to confirm eligibility, missing data from published reports (including from conference proceedings and posters), and enquiry about additional potentially eligible studies that were unpublished or just completed.
Study selection, data collection, and data items
Two independent researchers (E.B., J.L.S.L., L.C.F., P.M.F.B.) reviewed the records to select studies. Disagreements were double-checked and resolved through discussion with a third independent reviewer (M.H.B.). Initially, researchers inspected titles and abstracts, and then the full text and other data sources to fully assess eligibility. Multiple reports from the same study were linked together.
Summary data were extracted in a spreadsheet by one researcher (L.C.F.) and independently checked by another (P.M.F.B.). For each study, potential sources of information were at least one of the following: journal articles, clinical study reports, and unpublished data provided by the study author.
We coded characteristics of the study (year of start; recruiting area; sponsorship and sponsors; parallel versus crossover), participants (age; proportion of males; proportion of Asian, Black, or White; proportion of Hispanics; diagnostic criteria and diagnosed conditions) and treatment (drug administered; treatment duration; doses). We also coded patient disposition (number of randomized, number of total discontinuations) and outcome measures.
Change in ADHD symptom severity was the primary outcome. Total ADHD symptoms were preferred over inattentive or hyperactive-impulsive symptoms. When multiple rating scales were provided, we adopted the following prespecified hierarchy: ADHD rating scale (DuPaul et al., 1998), Swanson, Nolan, and Pelham ADHD rating scale (Bussing et al., 2008), and Conners rating scales (Conners et al., 1998a; Conners et al., 1998b). However, data from other validated or unvalidated instruments were extracted if necessary. When data from multiple informants were reported, we adopted the following prespecified hierarchy: clinicians, teachers, and parents.
Change in tics severity was the secondary outcome. The Yale Global Tic Severity Scale (Leckman et al., 1989) was the preferred rating scale, but we also extracted data from other validated or unvalidated instruments if necessary.
We preferentially extracted data based on intention-to-treat (ITT) analyses irrespective of the method used to handle missing data, for example, last observation carried forward or mixed model repeated measures. However, we also extracted data based on completers (modified ITT) if those were the only data reported to avoid excluding data from otherwise eligible studies. This procedure is in line with the proposed order of preference established in the Cochrane Handbook. For studies that randomized participants to multiple doses of the same medication, we combined arms utilizing the formula from the Cochrane Handbook because we considered that all administered doses were therapeutic. We did not have to impute missing standard deviations.
We evaluated the risk of bias for each outcome with the Cochrane Risk of Bias tool, version 2 (Sterne et al., 2019). We followed usual recommendations to rate risk of bias in five domains: randomization process; deviations from intended interventions; missing data; outcome measurement; and selection of reported results. A detailed description of the methods used to rate each domain is provided in Supplementary Data S1 (Supplement S3).
Statistical analysis and assessment of certainty of evidence
Because most pharmacological interventions were examined in single, or few, RCTs, we examined pharmacological interventions considering medication categories when pertinent and following the prespecified protocol. The following groups of medications were evaluated: α2 agonists (clonidine; guanfacine) and stimulants (methylphenidate; amphetamines). We also evaluated individual medications separately to provide data for each individual agent.
We calculated standardized mean difference (SMD) with 95% confidence interval (CI) for both outcomes. For each pair of interventions, we initially conducted random-effects pairwise meta-analysis. We drew network plots to graphically represent direct comparisons and considered the transitivity assumption (Salanti, 2012) plausible given the stringency of the eligibility criteria (i.e., all included studies were similarly designed double-blinded RCTs recruiting children/adolescents and a dual diagnosis of TD + ADHD according to DSM).
We then proceeded with a random-effects network meta-analysis in a frequentist framework. Pharmacological interventions were ranked considering P-scores (Rücker and Schwarzer, 2015). Heterogeneity was evaluated by comparing τ2 with its empirical distribution (Rhodes et al., 2015, Turner et al., 2012) and the I 2 statistic. Incoherence was evaluated globally (design-by-treatment interaction test) and locally (separate indirect from direct evidence [SIDE]) (Krahn et al., 2013).
Certainty of evidence was evaluated with the Confidence In Network Meta-Analysis (CINeMA) framework (Nikolakopoulou et al., 2020). We followed usual recommendations to rate certainty of evidence in six domains: within-study bias, reporting bias, indirectness, imprecision, heterogeneity, and incoherence. To investigate reporting bias/publication bias, we also plotted comparison-adjusted funnel plots (Chaimani and Salanti, 2012). A detailed description of the methods used to rate certainty of evidence is provided in Supplementary Data S1 (Supplement S3).
All statistical analyses were conducted in R (R Development Core Team, 2010) with packages netmeta (Rücker et al., 2021) and meta (Balduzzi et al., 2019). A p < 0.05 was adopted as the threshold for statistical significance.
Results
We identified 13,218 records in database search and 557 records in clinical trial registries. Of these records, 1107 references were inspected in detail, and 29 references reporting on seven unique RCTs met eligibility criteria and were included in our study (Fig. 1). Our search in Google Scholar identified one additional study that was considered eligible for inclusion. The final list of included and excluded records, with reasons, is provided in Supplementary Data S1 (Supplements S4 and S5).
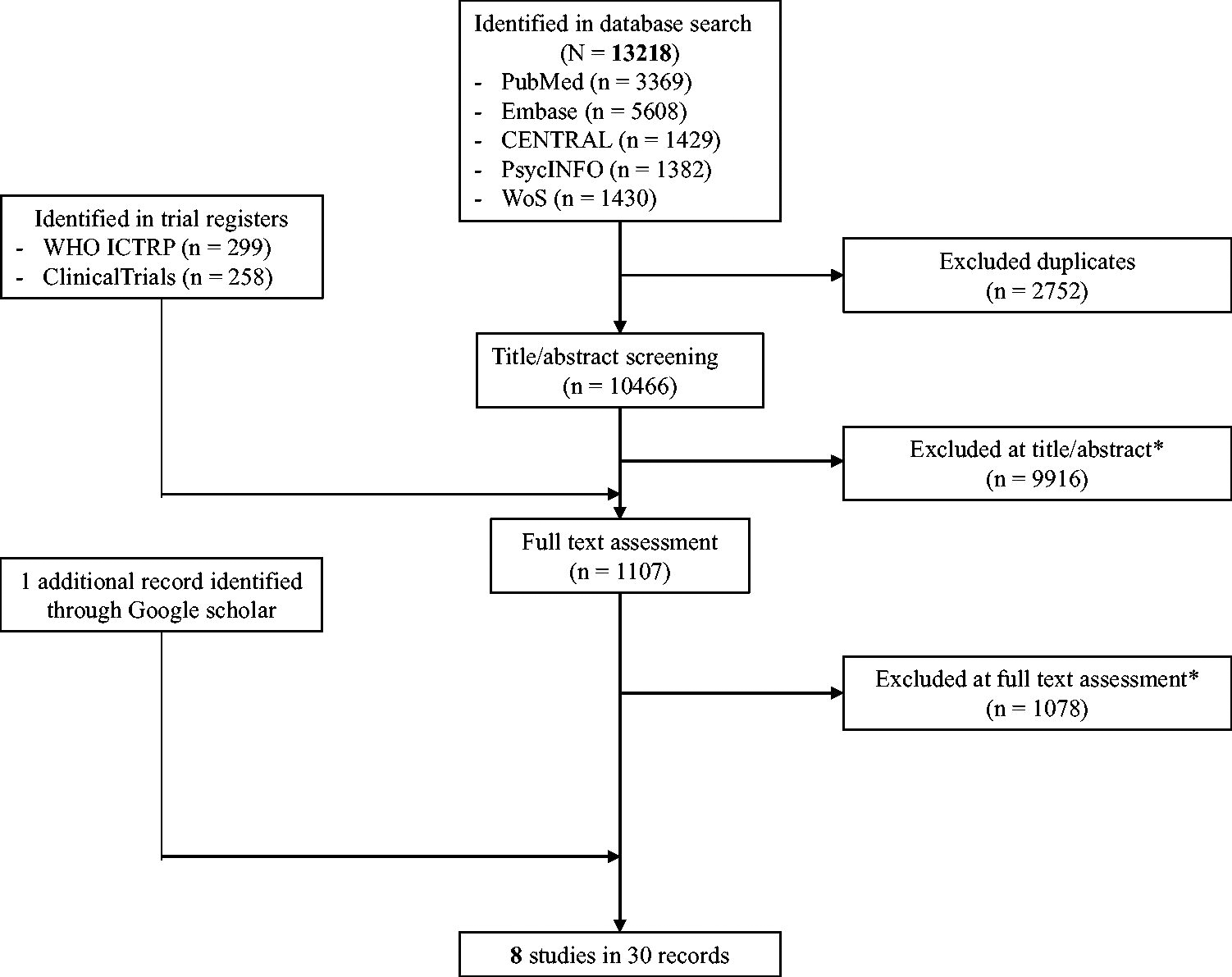
Study selection. *List of excluded studies provided in Supplementary Data S1.
The eight RCTs (Allen et al., 2005; Castellanos et al., 1997; Chen et al., 2024; Feigin et al., 1996; Gadow et al., 2007; Tourette’s Syndrome Study Group, 2002; Scahill et al., 2001; Singer et al., 1995) involved 575 children and adolescents who had a mean age 10 (SD: 2) and of which 504 (88%) were boys and 381 (85% of those with race information reported) were White. All studies were conducted in the United States before 2002 (median: 1995; IQR: 1993, 1997), except for one study that was conducted in China in 2012. Most of them were not sponsored by pharmaceutical companies (5, 63%). The following pharmacological interventions were administered for a median duration of 8 weeks (IQR: 4, 12): stimulants (dextroamphetamine, methylphenidate), α2 agonists (clonidine, guanfacine), atomoxetine, and selegiline. Only one study did not provide data that could be used for the ADHD symptoms meta-analysis (Castellanos et al., 1997) (Table 1). One (13%) and seven (87%) studies were rated at overall high and some concerns of risk of bias, respectively. Domain-level ratings of risk of bias for each study are provided in the Supplementary Data S1 (Supplement S6).
Characteristics of Included Studies
ADHD, attention-deficit/hyperactivity disorder; ADHD-RS, ADHD rating scale; ASQ, Conners Abbreviated Symptom Questionnaire; DSM, Diagnostic and Statistical Manual; VAS, Visual Analog Scale; NR, Not reported; YGTSS, Yale Global Tic Severity Scale; YGTSS-TTS, Yale Global Tic Severity Scale Total Tic Score.
Pairwise meta-analysis results for the placebo-controlled comparisons (Supplement S7), treatment rankings according to P-scores (Supplement S8), detailed statistics for the SIDE test (Supplement S9), comparison-adjusted funnel plots (Supplement S10), and domain-level certainty of evidence for each comparison (Supplement S11) are provided in the Supplementary Data S1.
In terms of network geometry, there were several direct comparisons, as atomoxetine and selegiline were the only interventions exclusively evaluated in placebo-controlled trials (Fig. 2).
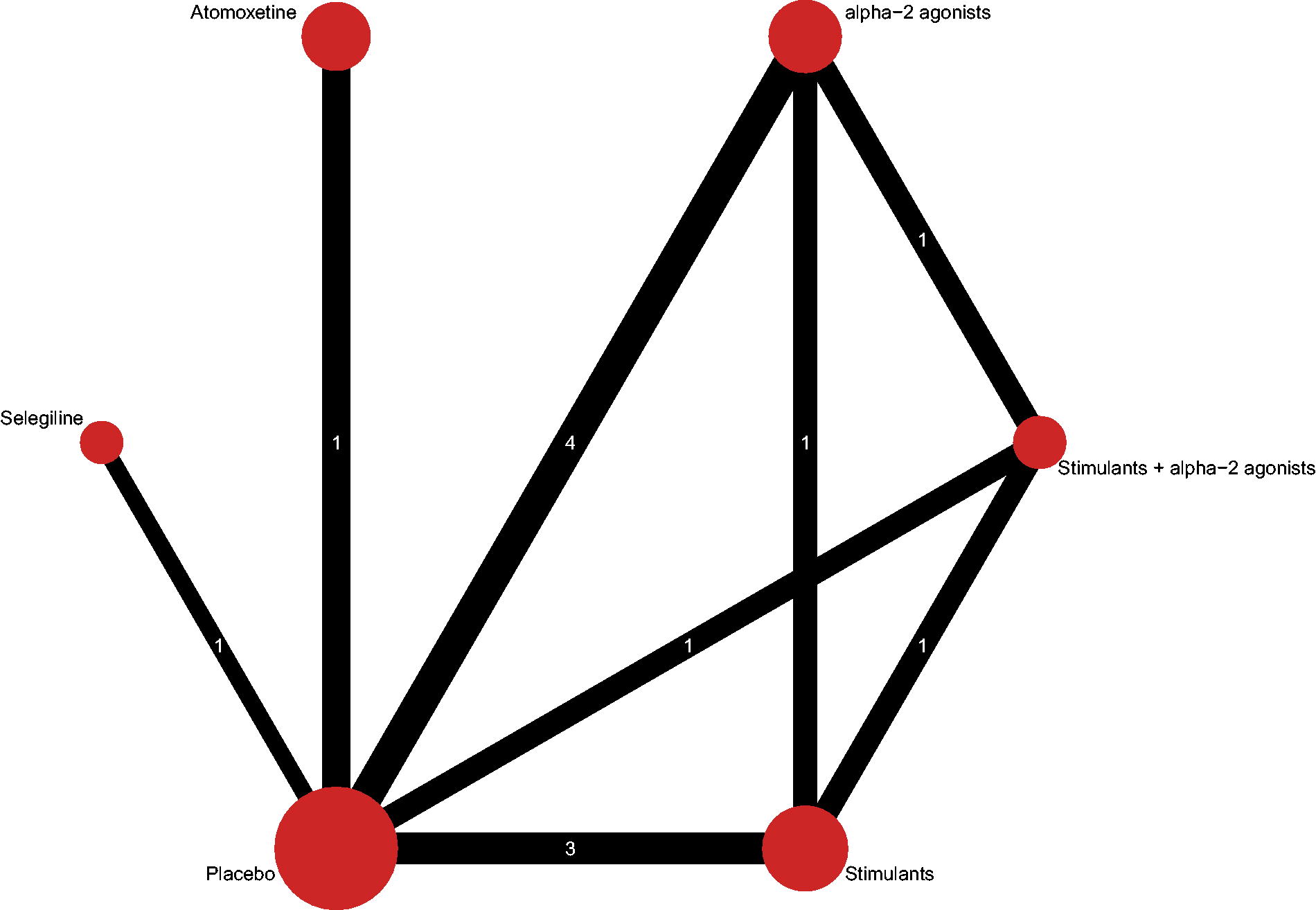
Network plot for tics severity. The size of nodes is proportional to the number of participants that received that treatment. The number of studies for each comparison is illustrated in the line, and its thickness is proportional to the precision of the direct estimate for that comparison. The network plot for ADHD symptoms severity is identical, although there are two (instead of three) RCTs for the comparison between stimulants and placebo. ADHD, attention-deficit/hyperactivity disorder; RCTs, randomized controlled trials.
Network meta-analysis demonstrated that α2 agonists (SMD [95% CI] −0.72 [−1.13 to −0.31]; very low certainty of evidence), stimulants + α2 agonists (−0.84 [−1.54 to −0.13]; very low), and stimulants (−0.54 [−1.05 to −0.03]; very low) were more efficacious than placebo in reducing ADHD symptoms severity in individuals with TD + ADHD (Fig. 3). Regarding comparisons between pairs of pharmacological interventions, no medication was more efficacious than another (very low) (Table 2).
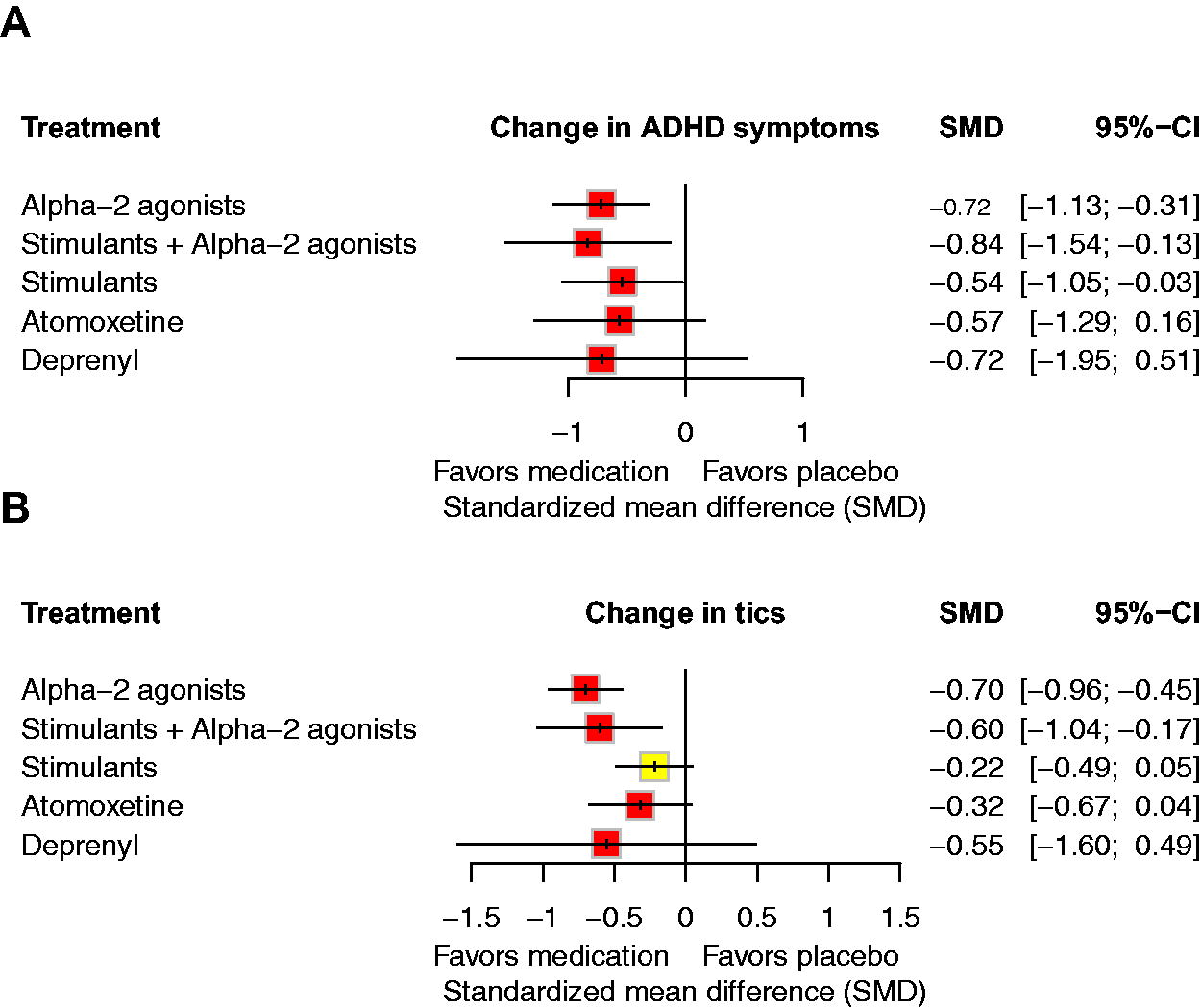
Forest plots for ADHD symptoms
League Table of Standardized Mean Difference for ADHD Symptom Severity (Lower Triangle) and Tic Symptom Severity (Upper Triangle) in Network Meta-Analysis with 95% Confidence Intervals
Standardized mean difference below 0 favors the column-defining treatment. Boldface indicates findings for which 95% confidence intervals exclude the possibility of no difference between interventions. Superscript symbols indicate certainty of evidence: low (*), very low (†).
Network meta-analysis demonstrated that α2 agonists (−0.70 [−0.96 to −0.45]; very low) and stimulants + α2 agonists (−0.60 [−1.05 to −0.17]; very low) were more efficacious than placebo in reducing tics severity in individuals with TD + ADHD (Fig. 3). Stimulants (−0.22 [−0.49 to 0.05]; low) were not associated with worsening of tics severity (Fig. 3). There were no significant differences between pairs of medications that were efficacious against placebo in reducing tics severity (low to very low) (Table 2).
Heterogeneity was moderate-high (τ2 = 0.11, I 2 = 65%) and low (τ2 = 0, I 2 = 34%) for the ADHD symptoms and tics meta-analyses. There was no evidence of global incoherence in the ADHD symptoms meta-analysis (Q = 0.43, p = 0.80), but for tics, there was evidence of global incoherence (Q = 6, p = 0.05). Assessments of local incoherence in the tics meta-analysis demonstrated disagreement between direct and indirect evidence for the comparisons involving α2 agonists versus placebo (Δ = −1.25, z = −2.32, p = 0.02), stimulants versus stimulants + α2 agonists (Δ = −1.39, z = −2.32, p = 0.02), and α2 agonists versus stimulants (Δ = 0.71, z = 2.11, p = 0.04).
Findings from network meta-analyses considering individual medications were similar for both outcomes (Supplement S12). However, only clonidine (−0.95 [−1.58 to −0.32]) and not guanfacine (−0.65 [−1.69 to 0.39]) separated from placebo in terms of ADHD symptoms.
Discussion
In this study, we reported the first network meta-analysis investigating the comparative efficacy of pharmacological interventions for ADHD symptoms and tics severity in children with TD + ADHD. We expanded and updated, to the best of our knowledge, the only previous meta-analysis examining pharmacological interventions for TD + ADHD (Bloch et al., 2009). Our findings indicated that α2 agonists and stimulants + α2 agonists were efficacious for both ADHD symptoms and tics severity. Stimulants were efficacious for ADHD symptoms only but were not associated with the worsening of tics. The certainty in the evidence from the network meta-analyses across all comparisons was low or very low. Taken together with our previous network meta-analyses in ADHD (Cortese et al., 2018) and TD (Farhat et al., 2023), the current study reinforces the challenging problem that practitioners often face when treating children and young people with mental health conditions: because comorbidity is common, practitioners must decide whether to rely on imprecise and inconsistent data within a population that closely resembles their patients or generalize larger and more reliable evidence that is less specific to their patients (Farhat and Bloch, 2021).
For ADHD symptoms severity, the larger body of evidence indicates that stimulants are the best pharmacological intervention for children and young people with ADHD. Stimulants have been demonstrated to have greater treatment benefits compared with other medications such as atomoxetine, clonidine, and guanfacine in RCTs of ADHD (Cortese et al., 2018). These medications also have a quicker time to effect than other available medications for ADHD, so patients and their families may perceive benefits early during treatment. While stimulants are associated with some adverse events, such as sleep disturbance and loss of appetite, there are strategies to manage them (Cortese et al., 2013), and recent evidence from observational studies corroborated the safety of these medications in the long term (Man et al., 2023). Consistent with these data, CPGs generally recommend that stimulants should be used as first-line therapeutic interventions in school-aged children and adolescents with ADHD (Coghill et al., 2021; Cortese 2020), including in the context of co-occurring conditions such as TD (National Institute for Health and Care Excellence, 2018). Contrary to the larger body of evidence, our study did not identify stimulants as having the largest effects in reducing ADHD symptoms severity compared with placebo. Specifically, both α2 agonists and the combination of α2 agonists and stimulants had larger effects in reducing ADHD symptoms severity than stimulants when compared with placebo. However, we also did not find statistically significant differences between stimulants and either α2 agonists or the combination of α2 agonists and stimulants (Table 2). Therefore, to some extent, our findings support the use of stimulants as first-line pharmacological interventions for ADHD in the context of TD.
Concerns that stimulants may cause or worsen tics remain, and medication labels indicate that stimulants should not be used if a child has a personal or familial history of TD. However, a previous meta-analysis did not indicate that there was evidence in ADHD RCTs that stimulants would cause or worsen tics at a greater rate than placebo (Cohen et al., 2013). The current study confirmed that stimulants did not worsen tics severity in children and adolescents with a dual diagnosis. Estimates from group-level meta-analyses such as the ones generated in this study and previous research (Cohen et al., 2013) may not apply directly at the level of the individual patient, and it is possible that some individuals may experience worsening of tics with stimulants. However, in the absence of personalized treatment recommendations, decision-making should consider evidence from all similar patients treated with a given intervention, which is in accordance with the ITT principle. These group-level data reinforce that, on average, stimulants do not cause or worsen tics.
For tics severity, the larger body of evidence in the field indicates that antipsychotics are the most efficacious pharmacological intervention, whereas α2 agonists would only lead to relatively small, and possibly nonclinically meaningful, effects (Farhat et al., 2023). Strikingly, we did not identify any RCTs that investigated antipsychotics for tics severity in TD + ADHD. However, half (4, 50%) of the RCTs investigated α2 agonists. We found a substantially greater effect of α2 agonists for tics in TD + ADHD than Farhat et al. (2023) previously found in TD without the requirement of comorbid ADHD (SMD [95% CI −0.21 [−0.39 to −0.03]). This difference indicates that ADHD status may moderate the effects of α2 agonists on tics severity. Consistently, recently published CPGs from the AAN and ESTSS both recommend that α2 agonists should be adopted as first-line pharmacological intervention for tics severity in TD + ADHD (Pringsheim et al., 2019; Roessner et al., 2022). The underlying rationale behind this potential moderator effect is unclear, but some hypothesize that increased cognitive control (i.e., from treating ADHD symptoms) could contribute to greater control of tic symptoms (Morand-Beaulieu et al., 2017). Future studies should examine directly the moderator effects of ADHD in the α2 agonists response in TD.
Clinical relevance
From a practical standpoint, the choice of the optimal medication in TD + ADHD may be guided by the chief health need as well as the therapeutic plan for a given patient (Jaffe and Coffey, 2022). Transparent, evidence-based communications with the child and their family about risk-benefits and shared decision-making should be at the center of this process.
Practitioners may consider prioritizing the reduction of ADHD symptoms severity in the first moment before addressing tics. Patients with TD often perceive their ADHD symptoms as more impairing than their tics. Besides, tics typically wax and wane across periods of weeks and months (Leckman et al., 2014), and several months of follow-up may be required to determine whether a medication is effective or not in the real world. In contrast, stimulants work fast and have the largest effects in child and adolescent psychiatry (Correll et al., 2021), so that practitioners, patients, and their families may rapidly assess improvement in ADHD symptoms severity. Last, CBIT is recommended as a first-line treatment for tics, and if available, it should be initiated first prior to pharmacotherapy. Relatedly, although the available evidence base does not indicate that ADHD status moderates the effects of CBIT (Sukhodolsky et al., 2017), children may be more likely to be successful in perceiving premonitory urges and implementing competing responses if their ADHD symptoms levels are reduced.
In cases where tics are also perceived as bothersome and behavioral treatments are not available, risk-benefits between antipsychotics, the most efficacious pharmacological intervention for tics (Farhat et al., 2023), and α2 agonists should be considered. Antipsychotics may be preferred for more severe cases of tics considering their worse adverse event profile. In the context of TD + ADHD specifically, stronger consideration should be given to α2 agonists given that ADHD may moderate the effects of these medications on tics severity. Notably, α2 agonists are also efficacious for ADHD symptoms severity, which represents another therapeutic benefit of α2 agonists in the context of dual diagnoses.
There is also evidence corroborating that the combination of α2 agonists and stimulants is efficacious for both ADHD symptoms and tics severity compared with placebo. However, our analyses did not demonstrate significant differences between α2 agonists alone and their combination for either ADHD symptoms or tics severity. Therefore, without clear evidence of additional benefits, it may be more sensible to favor monotherapy rather than starting two medications simultaneously when initiating treatment.
Unfortunately, there has been no RCT investigating the sequential application of α2 agonists and stimulants for children and adolescents with TD + ADHD. The lack of any data creates uncertainties with regards to how to use these medications in a treatment algorithm. Some practitioners may consider adding α2 agonists after starting treatment with stimulants to avoid optimizing doses of the latter because of possible concerns that tics may worsen at higher doses of stimulants. Indeed, in our analyses stratified by medications, dextroamphetamine, which was administered in supratherapeutic doses, was associated with worsening of tics severity compared with methylphenidate, which was administered in therapeutic doses. However, there are no studies specifically investigating whether there is a dose–response association between (worsening of) tics and stimulant doses in ADHD RCTs. In contrast, recent meta-analytical evidence indicated that ADHD RCTs adopting flexible-dose titration to maximum FDA-licensed doses were associated with increased efficacy and acceptability compared with ADHD RCTs prescribing stimulants at lower doses (Farhat et al., 2022). Therefore, in general, practitioners may give stronger consideration to optimizing stimulant doses toward the maximum FDA-licensed range, as needed and tolerated. The addition of α2 agonists in combined treatment may be considered for cases in which tolerability limits stimulant dose escalation. This may represent a useful strategy as some adverse events associated with these medications are opposite (e.g., insomnia with stimulants and somnolence with α2 agonists).
Limitations
The current study is not without its limitations. We cannot discard having missed relevant studies, although we did our best efforts to identify all available RCTs. Strikingly, we only identified one additional double-blinded RCT evaluating pharmacological interventions for TD + ADHD even though the searches from the current and the original study are separated by at least ∼15 years. In addition, most of the available RCTs had methodological shortcomings, and there were no RCTs classified at low risk of bias. Additional RCTs are needed to confirm these observations based on the extant studies. In this regard, it is worth citing the ongoing SATURN trial (ISRCTN14910154), a UK-based RCT that is examining whether stimulants are superior for ADHD symptoms and non-inferior for tics in children and young people with TD + ADHD. Besides, most studies had a crossover design. The inclusion of crossover studies in meta-analysis is challenging because, in most cases, the reporting is not ideal. Specifically, participants from crossover RCTs are usually double-counted, which introduces a unit-of-analysis problem. Although we attempted at acquiring individual participant data or aggregated pre-crossover data to deal with this limitation, we were only successful in one of four (25%) RCTs, as all were published at least 16 years ago and datasets were often not available. Some of our findings regarding individual medications may have been influenced by limited data availability. For instance, statistically significant effects for clonidine and not guanfacine may be attributed to the larger number of RCTs (3 versus 1) and participants (103 versus 17) evaluating the former compared with the latter. When considering TD RCTs irrespective of comorbid ADHD status, there are also few RCTs for guanfacine compared with clonidine and a similar pattern of effects against placebo (Farhat et al., 2023). While we cannot discard there may exist differences across these medications in terms of their effects in reducing tics severity, clonidine and guanfacine share pharmacodynamic properties, and it is likely that the lack of significant findings is only related to limited data availability as indexed by very low certainty in the estimates from the network meta-analyses. Relatedly, because of limited data availability, we were also not capable of examining other outcomes (e.g., adverse event profile), which are important when deciding between different medications given the limited number of studies and the fact that those adverse events are relatively rare events. Last, our analyses included data from group-level summaries, which may not be generalized at the individual level.
Conclusion and Future Perspectives
Our network meta-analysis corroborated findings previously reported in the literature. Stimulants are efficacious for ADHD symptom severity and do not increase tics severity in TD + ADHD. α2 agonists are efficacious for both ADHD symptoms and tics severity in TD + ADHD. Additionally, the effects of α2 agonists on tics severity may be moderated by ADHD status. These findings should help guide practitioners and families in the choice of medication for children and young people with TD + ADHD through shared decision-making. As these conclusions are based on weak evidence base, additional studies, for instance, examinations of electronic health records and in particular RCTs, are needed to confirm these observations based on the extant studies.
Footnotes
Acknowledgments
The authors thank the authors and participants from the included studies. The authors also thank authors who provided additional unpublished information for this article. The authors thank Jessica L.S. Levine and Ziyu Wang for their role in study selection for this project.
Authors’ Contributions
Conceptualization: L.C.F., S.C., G.V.P., and M.H.B.; Data curation: L.C.F., E.B., and M.F.B.; Methodology: L.C.F., E.B., M.F.B., A.L.-W., and M.H.B.; Formal analysis: L.C.F. Writing—original draft: L.C.F. and M.H.B.; Writing—review and editing: E.B., A.L.-W., M.F.B., S.C., and G.V.P.; Supervision: M.H.B..
Disclaimer
The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR, NHS, or the UK Department of Health and Social Care.
Disclosures
S.C., NIHR Research Professor (NIHR303122), is funded by the NIHR for this research project. S.C. is also supported by NIHR grants NIHR203684, NIHR203035, NIHR130077, NIHR128472, RP-PG-0618-20003 and by grant 101095568-HORIZONHLTH-2022-DISEASE-07-03 from the European Research Executive Agency. S.C. has declared reimbursement for travel and accommodation expenses from the Association for Child and Adolescent Central Health (ACAMH) in relation to lectures delivered for ACAMH, the Canadian AADHD Alliance Resource, the British Association of Psychopharmacology, and from Healthcare Convention for educational activity on ADHD, and has received honoraria from Medice. G.V.P. has been a consultant, advisory board member, and/or speaker for Aché, Abbott, Apsen, Medice, Novo Nordisk, Pfizer, and Takeda. G.V.P. also receives royalties from Editora Manole. M.H.B. has received grant or research support from Therapix Biosciences, Emalex Biosciences, Janssen Pharmaceuticals, Biohaven Pharmaceuticals, NIH, Lesbian Health Fund, and the Yale Foundation for Lesbian and Gay Studies (FLAGS), and Patterson Foundation. He has also served on the advisory board/data monitoring and safety board of Therapix Biosciences. He also serves as associate editor of Journal of Child Psychology and Psychiatry and on the editorial board of Journal of Child and Adolescent Psychopharmacology. He has received royalties from Wolters Kluwer for Lewis’s Child and Adolescent Psychiatry: A Comprehensive Textbook, Fifth Edition. He has received moonlighting pay from the Veteran’s Administration. The other authors report no disclosures.
Supplementary Material
Supplementary Data S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.