
Abstract
We conducted a phase I-II clinical trial to assess the safety and efficacy of combining lutetium-177 (177Lu)-octreotate with capecitabine and temozolomide in treating advanced low-grade neuroendocrine tumors (NETs). All 35 patients received fixed activities of 7.8 GBq 177Lu-octreotate each 8 weeks, with 14 days of capecitabine 1500 mg/m2 for 4 cycles. In phase I, successive cohorts of patients received escalating doses of temozolomide in groupings of 100, 150, and 200 mg/m2 in the last 5 days of each capecitabine cycle. In phase II, patients were treated with 200 mg/m2 temozolomide. Treatment was well tolerated in all dosage groups. No dose-limiting grade 2, 3, or 4 toxicities were seen in cohorts 1 (100 mg/m2) or 2 (150 mg/m2). Twenty-eight patients completed treatment at the 200 mg/m2 temozolomide level. Adverse events were mild to moderate. The commonest toxicities were transient nausea grade 2 (18%), grade 3 (3%), thrombocytopenia grade 2 (24%), and neutropenia grade 3 (6%). There were no grade 4 events. Thirty-four patients were evaluable for tumor response. Overall, complete response (CR) was achieved in 15% (95% CI 3–27); partial response (PR), in 38% (95% CI 22–55); stable disease (SD), in 38% (95% CI 22–55); and 3 patients failed to respond to treatment. Median progression free survival (PFS) was 31 months (95% CI 21–33), and median overall survival (OS) has not been reached with 90% surviving at 24 months follow-up (range 21–30). Overall objective response rate (ORR) in patients with gastroenteropancreatic NETs showed CR 16% (95% CI 3–28), PR 41% (95% CI 24–58), SD 37% (95% CI 21–54), and PD 6% (95% CI 0–15). Response rates were higher in patients with gastropancreatic NETs than in those with bowel primaries (enteric-NETs); CR 18% versus 13%, PR 64% versus 13%, SD 12% versus 67%. 177Lu-octreotate, in combination with capecitabine and temozolomide, is well tolerated in patients with advanced low-grade NETs, and shows substantial tumor control rates.
Introduction
Low-grade neuroendocrine tumors (NETs) arise in many body areas and particularly in gastropancreatic (GP) tissues and the small bowel. The primary treatment of NETs such as carcinoid and islet cell tumors is surgery, with curative intent, or to debulk the tumor mass. Unfortunately, for 80% of presentations, this is impossible. 1 Most of these tumors express somatostatin receptors, subtype 2, in high abundance. Somatostatin derivatives, such as octreotide, can be used to treat symptoms of hormonal overproduction. Recent studies have also demonstrated substantial effects on tumor growth characteristics and the prolongation of survival. 2 The rationale for the use of radiolabeled somatostatin analogs is based on evidence that they accumulate in somatostatin receptor-containing tissue or tumors. Receptors remain present and are able to bind radiolabeled somatostatin analogs during the treatment of NETs. 3 Somatostatin peptide analogs, coupled with a complexing moiety (DOTA), can be labeled with the beta-emitter lutetium-177 (177Lu) and may deliver a tumoricidal radiation dose. 177Lu is a medium-energy beta-emitter with a maximum tissue penetration of 2 mm and a physical half-life of 6.7 days, and it also emits medium- and low-energy gamma radiation of modest abundance that can be used for imaging and dosimetry. Octreotate binds with a high affinity to somatostatin receptors and retains both binding properties and physiological function when labeled with 177Lu. Uptake in somatostatin receptor subtype-2 expressing NETs is 3–4 times higher for 177Lu-octreotate than the standard diagnostic imaging agent 111In-octreotide. 4 Tumor-targeted peptide radionuclide radiation therapy (PRRT) is now under experimental and clinical evaluation. Initial promising results have been obtained with 177Lu-octreotate with impressive control in a high percentage of NETs patients, with little toxicity. 5
We have recently completed a study of radiosensitizing chemotherapy using capecitabine in combination with 177Lu-octreotate. 6 Tumor control and stabilization was obtained in 94% of patients with previously progressive NETs. Control consisted predominantly of stabilization, with true partial responses (PR) in only 24% of patients. However, in these slowly developing tumors, stabilization is often a highly meaningful outcome, both in terms of patient quality of life and in progression-free survival (PFS), which was 88% at 2 years in our study. 6
Several reports have pointed to high response rates in patients with advanced pancreatic neuroendocrine tumors (PNETs) using the combination of capecitabine and temozolomide chemotherapy. 7,8 These preliminary results have latterly been confirmed by Strosberg et al. 9 in 30 patients with advanced PNETs, achieving an excellent response of more than 70% with the combination of temozolomide and capecitabine. 9 Our previous experience with capecitabine chemosensitization led us to extend our study with 177Lu-octreotate by incorporating temozolomide with capecitabine in a phase I-II trial.
Materials and Methods
Patients
Eligible patients had histologically proven NETs that were inoperable, and progressive on serial CT/MRI scans at least 6 months apart; or patients presenting with highly advanced metastatic disease and substantial symptoms. Patients had a Karnofsky performance status of >60% and a life expectancy of at least 12 weeks, adequate renal function (serum creatinine <150 μmol/L or measured creatinine clearance of >50 mL/min.), adequate hepatic function (bilirubin <3×ULN, serum transaminases <3×ULN), and adequate bone marrow function (neutrophil count >1.5×109/L, platelets >100×109/L). Previous chemotherapy or radiotherapy must have finished a least 6 weeks before initiating radiopeptide therapy. Long-acting somatostatin analogs were ceased a minimum of 6 weeks before radiopeptide therapy. At least one measurable lesion was required for response evaluation on CT/MRI scans. The presence of somatostatin receptors was required in the majority of the known tumor deposits, as demonstrated by 177Lu-octreotate SPECT/CT or 68Ga-octreotate PET/CT scan. All patients provided written informed consent to participate in the clinical trial. The protocol was approved by the institutional ethics committee governed by the Australian National Health and Medical Research Council guidelines for human experimentation in accordance with the declaration of Helsinki.
Radiopeptide therapy
177Lu-octreotate was prepared in house from [DOTA,Tyr3] octreotate: 240 mcg of peptide was labeled with 9.3 GBq 177LuCl3 using an automated module (Synthera® IBA Belgium). 10 Each patient received an infusion of amino acids (Synthamin; Baxter Healthcare) comprising 11.6 g/L lysine and 23 g/L arginine at 240 mL/h for 4 hours. After 30 minutes, 7.8 GBq 177Lu[DOTA, Tyr3] octreotate was co-infused with the amino acids. Routine antiemetics were given in the form of IV tropisetron and oral lorazepam. All patients were treated on an outpatient basis. 11
Dosimetry
Quantitative whole-body gamma imaging was performed at 4 hours, 24 hours, 48 hours, and 5 days after each of the 4 cycles of 177Lu-octreotate. Dynamic and early serial whole-body imaging was also performed at 30 minutes, 1 hour, and 2 hours in one of the treatment cycles to define pharmacokinetics. Critical organ and tumor dosimetry was performed by an analysis of attenuation-corrected quantitative SPECT/CT imaging. Estimates of radiation-absorbed dose (Gy) to the kidneys and liver were calculated by voxel-based methodology using cumulative activity maps convolved with a 4 mm 177Lu voxel dose kernel generated by the MCNPX Monte Carlo code. 12,13
Chemotherapy
Radiopeptide was given each 8 weeks for 4 treatment cycles at a fixed activity of 7.8 GBq 177Lu-octreotate. Chemotherapy commenced 5 days before radiopeptide administration with oral capecitabine 1500 mg/m2 for 14 days in all patients. Oral temozolomide was given in the last 5 days of each 14 day capecitabine period. In phase I, successive cohorts of patients received escalating doses of temozolomide in groupings of 100, 150, and 200 mg/m2. In phase II, all patients were treated with 200 mg/m2 temozolomide with dosage adjustments for toxicity.
Evaluation of response and toxicity
The primary objective of this study was to establish the optimal, safe, cytotoxic, and radiosensitizing dose of temozolomide in combination with 177Lu-octreotate and capecitabine. The secondary objectives of our study comprised measurement of tumor responsiveness and patient survival parameters, including PFS and overall survival (OS) wherever possible. Toxicities were graded according to standard National Cancer Institutes Common Terminology Criteria for adverse events version 4.03. 14 The objective response evaluation was measured according to Response Evaluation Criteria in Solid Tumors (revised RECIST guideline, version 1.1). 15 Triple-phase CT or MRI was performed at baseline and then every 4 months. The absence of any detectable abnormality on follow-up CT/MRI was interpreted as complete response (CR). The metabolic response was assessed by tumor uptake on 24-h whole-body scans after each cycle of 177Lu-octreotate referenced to the standard activity of a 10 MBq 177Lu source included in the field of view (Fig. 1). Gallium-68 octreotate PET/CT imaging was performed 6 months after the completion of radiopeptide therapy to define delayed metabolic response.
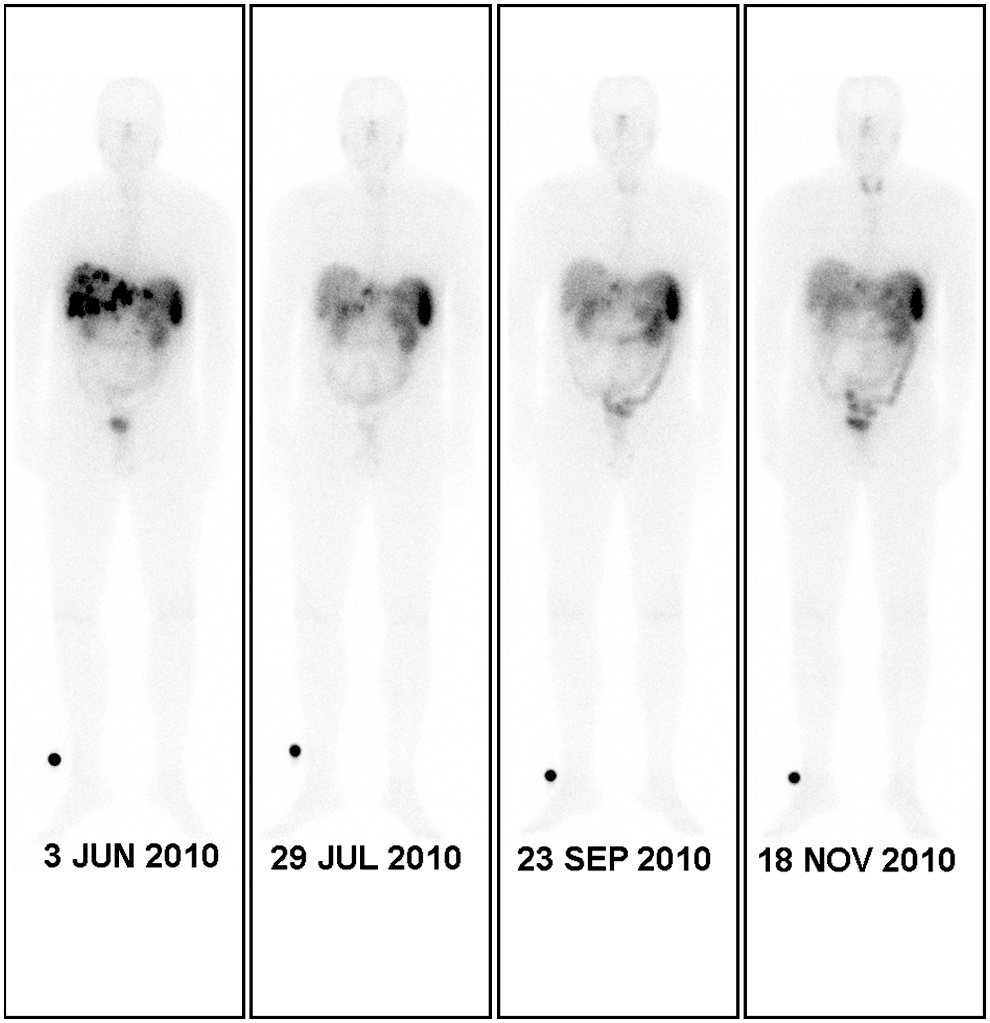
Serial whole-body gamma images at 24 hours after every 4 cycles of 7.8 GBq lutetium-177 (177Lu)-octreotate at 8 week intervals with concomitant capecitabine and temozolomide in a 48 year-old man with pancreatic neuroendocrine tumor (NET). The images are normalized for intensity by a 10 MBq 177Lu standard on the leg and show progressive interval reduction in radiopeptide tumor uptake in hepatic metastases, indicative of metabolic response.
Statistical analysis
Safety and efficacy data were evaluated using descriptive statistics. The 95% confidence interval for response was calculated by the exact (binomial) method. The Kaplan–Meier method was used to estimate time to progression, PFS, and OS. The time intervals were calculated from the date of first treatment until documentation of tumor progression or until death from any cause. The lower and upper limits of the 95% CI were calculated according to the efficient-score method. 16,17
Results
Patient characteristics
Thirty-five patients (24 men and 11 women) with progressive low-grade NETs were enrolled: 34 evaluable patients completed therapy and were analyzed for toxicity and response. Their median age was 63 years (range 33–81). Clinical and pathological characteristics are listed in Table 1. All the tumors were well differentiated, being predominantly Grade 1 according to WHO 2010. 18 The primary sites were GP 17 (50%), bowel 15 (44%), and lung 2 (6%). Sixteen patients (46%) had nonfunctional tumors, 13 (37%) had functional carcinoids, 4 (11%) had gastrinomas, 1 had insulinoma, and 1 had glucagonoma. The principal metastatic sites were liver, 33 patients (94%); nodal, 18 (51%); and other (4 bone, 2 lung, and 5 peritoneum) (Table 1). Hepatic metastatic tumor burden for each patient at baseline is defined in Table 2, being the sum of the diameters of 4 tumors in each patient, measured according to RECIST 1.1 criteria.
Tumor response in each NET patient (n=34) is correlated with tumor site and hepatic metastatic burden, measured as the sum of the diameters of 4 tumors according to RECIST 1.1 criteria, to determine objective response. Corresponding metabolic response on 177Lu-octreotate and 68Ga-octreotate imaging, and with biochemical response measured by baseline and 6 month follow-up CgA, are also shown. Objective response is greater for gastropancreatic NETs than for E-NETs. All NETs were well differentiated (WD) on histopathology.
Lu, lutetium-177; CR, complete response; PR, partial response; SD, stable disease; NET, neuroendocrine tumors; GFP, gastroenteropancreatic; GP, gastropancreatic; E-NET, enteric NET.
Twelve patients had earlier received octreotide for the control of symptoms, while 13 had undergone neither surgical nor medical interventions. Six patients had received previous chemotherapies or targeted agents, such as sunitinib. Twenty patients had undergone not only surgical resections of various types, predominantly bowel resections of primary gut carcinoids, but also some cytoreductive liver resections. Only 2 patients had trans-arterial hepatic embolizations, and 2 had received 90Y microsphere treatment.
Toxicities
Thirty-five patients were enrolled in this study between March 2009 and May 2011. All patients were assessed for toxicity; however, 1 patient failed to complete the first treatment cycle due to early-onset capecitabine-induced angina and was excluded from outcomes analysis. The remaining 34 patients completed the phase I-II treatment program, and an intention-to-treat analysis of safety and efficacy is presented.
In cohorts 1 and 2, receiving 100 and 150 mg/m2 of temozolomide respectively, all patients (3 in each group) completed 4 full cycles of the allotted chemotherapy and radiopeptide. No dose-limiting grade 2, 3, or 4 toxicities were seen. Twenty-eight patients were treated in the temozolomide 200 mg/m2 group. Twenty-five (89%) of these patients received all 4 cycles of 177Lu-octreotate, 1 patient ceased treatment after 2 cycles, one ceased treatment after 3 cycles due to tumor progression, and 1 patient had their final treatment deleted due to persistent thrombocytopenia. Overall, 108 out of the total 112 planned doses of 7.8 GBq 177Lu-octreotate were given.
Dosage adjustments of the chemotherapy were necessary because of toxicity in a small number of patients. In all, 92% of the planned capecitabine and 87% of the temozolomide dosage was given across the 4 treatment cycles. The most common reason for dose reduction was thrombocytopenia (Table 3). Two patients had grade 3 capecitabine-induced angina, which resolved without sequelae with cessation of the drug. Otherwise, overall toxicity was mild. The most common adverse events were grade 1 or 2 nausea that was associated with the amino acid infusions and the chemotherapy. Hematological toxicity was mild with 8 patients experiencing grade 2 reversible thrombocytopenia, which occurred more commonly in patients who had received previous chemotherapy, targeted agents, or hepatic intra-arterial 90Y microspheres. There were no episodes of febrile neutropenia or renal impairment. Two patients died of progressive disease. There were no toxic deaths.
NCI Common Terminology Criteria for Adverse Events (CTCAE) version 4.03 June 14, 2010. 14
The median radiation absorbed dose per cycle for critical organs was computed to be 2.4 Gy (range 1.1–3.6 Gy) for kidneys and 4.8 Gy (1.1–11.8 Gy) for the liver. In patients receiving the full 4 courses of radiopeptide, the cumulative doses were 9.6 Gy (4.5–14.6 Gy) for the kidneys and 19.2 Gy (4.4–47.3 Gy) for the liver, which were well below toxic thresholds. No scintigraphic uptake was seen in the bone marrow.
Treatment response
The overall radiographic objective response, as defined by RECIST guidelines, was assessed every 4 months by CT or MRI scans (Figs. 1 –4). All patients were also assessed by 177Lu-octreotate gamma imaging for metabolic response in each treatment cycle. In general, reductions in gamma tumor uptake measurements corresponded well with RECIST responses (Table 2). At a median follow-up of 18 months (range 12–33 months), the overall objective response rate (ORR) was 56% (95% CI 39–73%). Among the entire group of 34 patients, 5 (15%) (95% CI 3–27) patients achieved a CR, 13 patients (38%) (95% CI 22–55), PR, and 13 patients (38%) (95% CI 22–55) stable disease (SD) for an overall tumor control rate of 91%. The evaluable patient response for gastroenteropancreatic (GEP)-NETs, illustrated in a waterfall plot (Fig. 5) demonstrated that GP-NETs responded significantly better than enteric NETs (E-NETs). Lung NETs are not included.
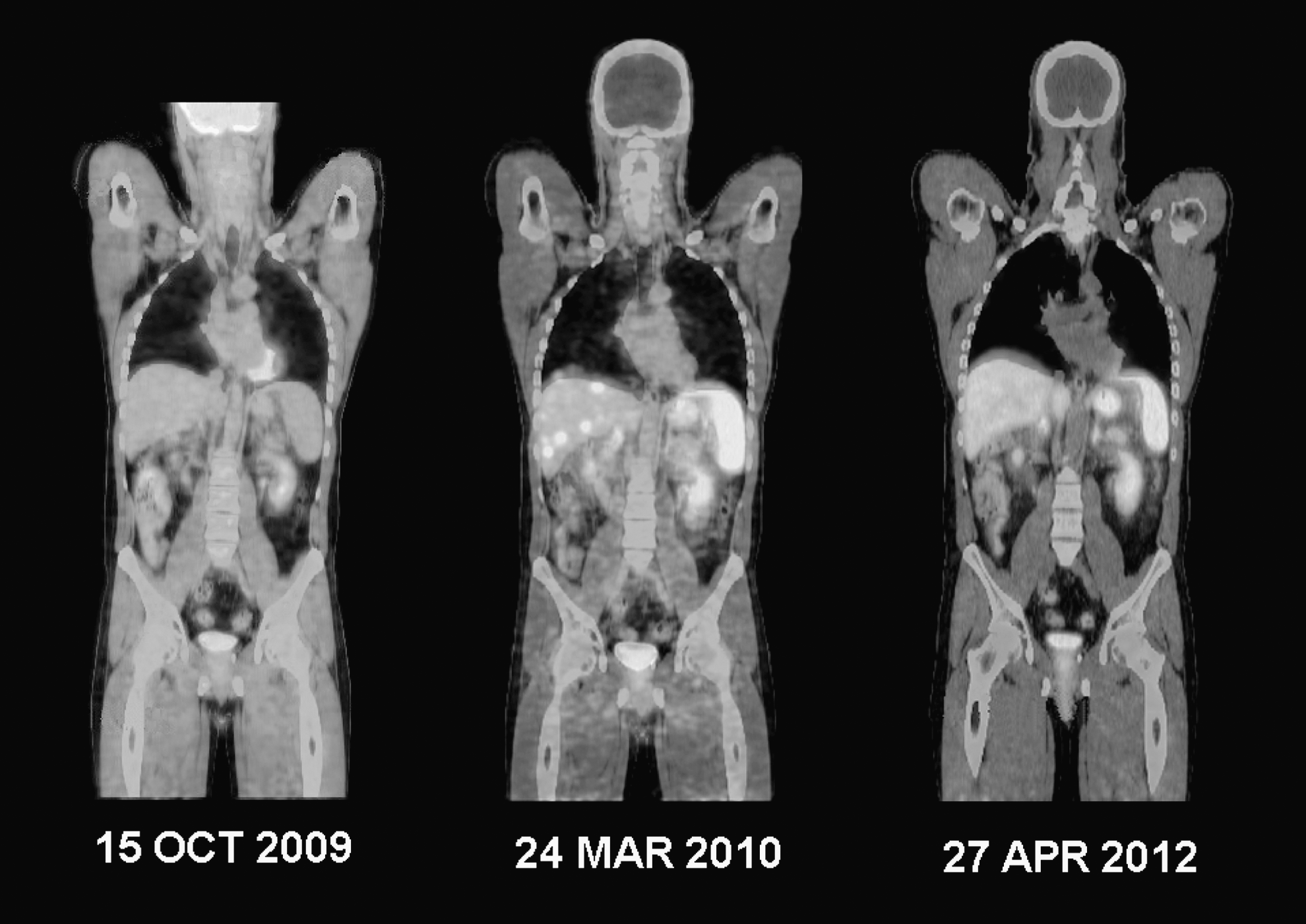
Initial 18F-FDG PET/CT shows minimal hepatic abnormality, but subsequent 68Ga-octreotate PET/CT demonstrates high radiopeptide uptake in multiple liver metastases, which is resolved on follow-up 68Ga-octreotate PET after 4 cycles of 177Lu-octreotate, capecitabine, and temozolomide therapy, indicative of a complete metabolic response.
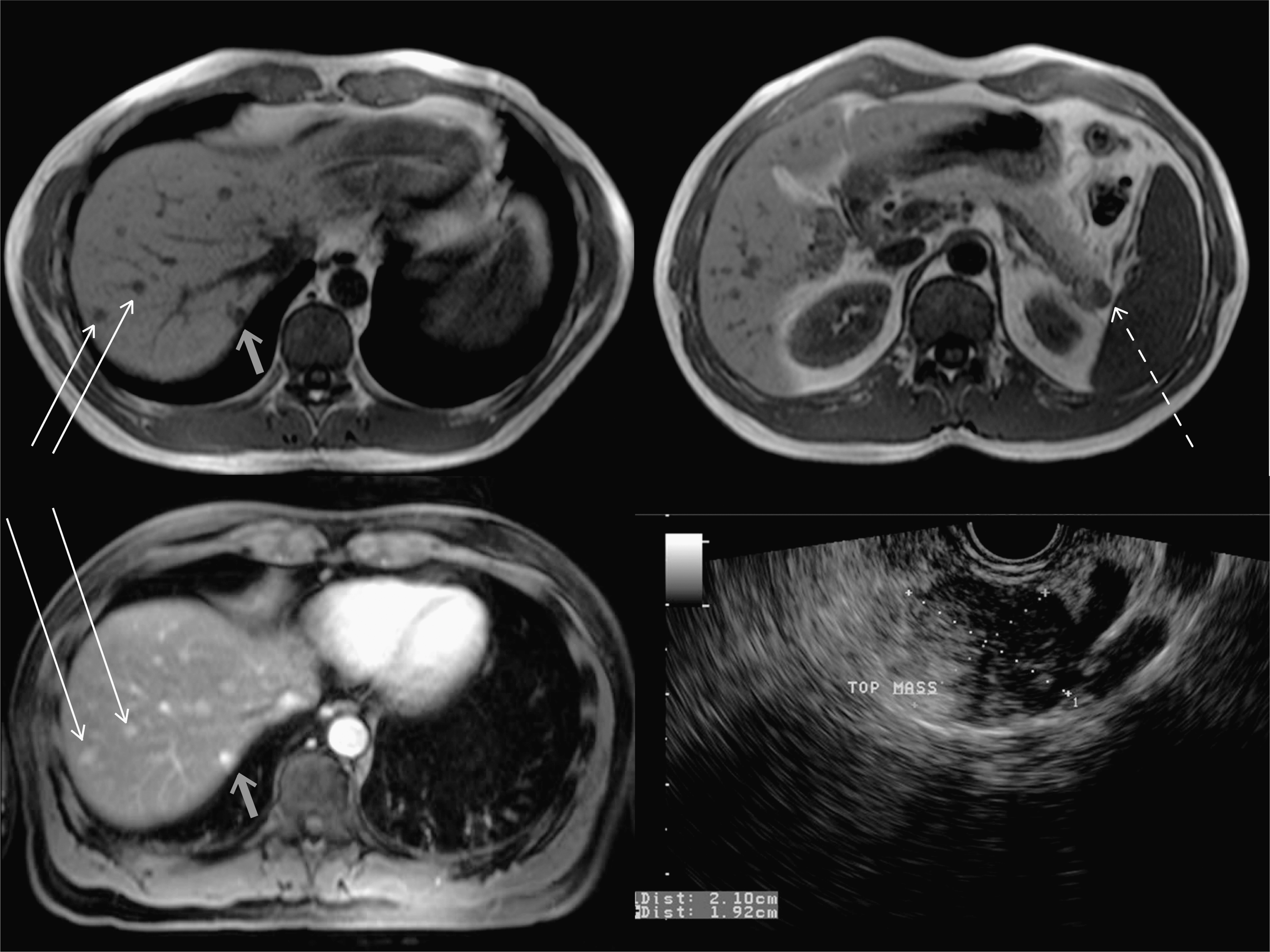
Baseline MRI May 2010 Axial T1w slices demonstrate multiple low-signal hepatic metastases in the right lobe of the liver (long arrows) and pancreatic tail (interrupted arrow). Post-Gadolinium T1w MRI at 30 seconds demonstrates avid enhancement of liver metastases (long arrows) in this pretreatment baseline study. The subcapsular lesion within segment 7 is a hemangioma (short arrow). Endoscopic ultrasound delineates the primary NET in the pancreatic tail.
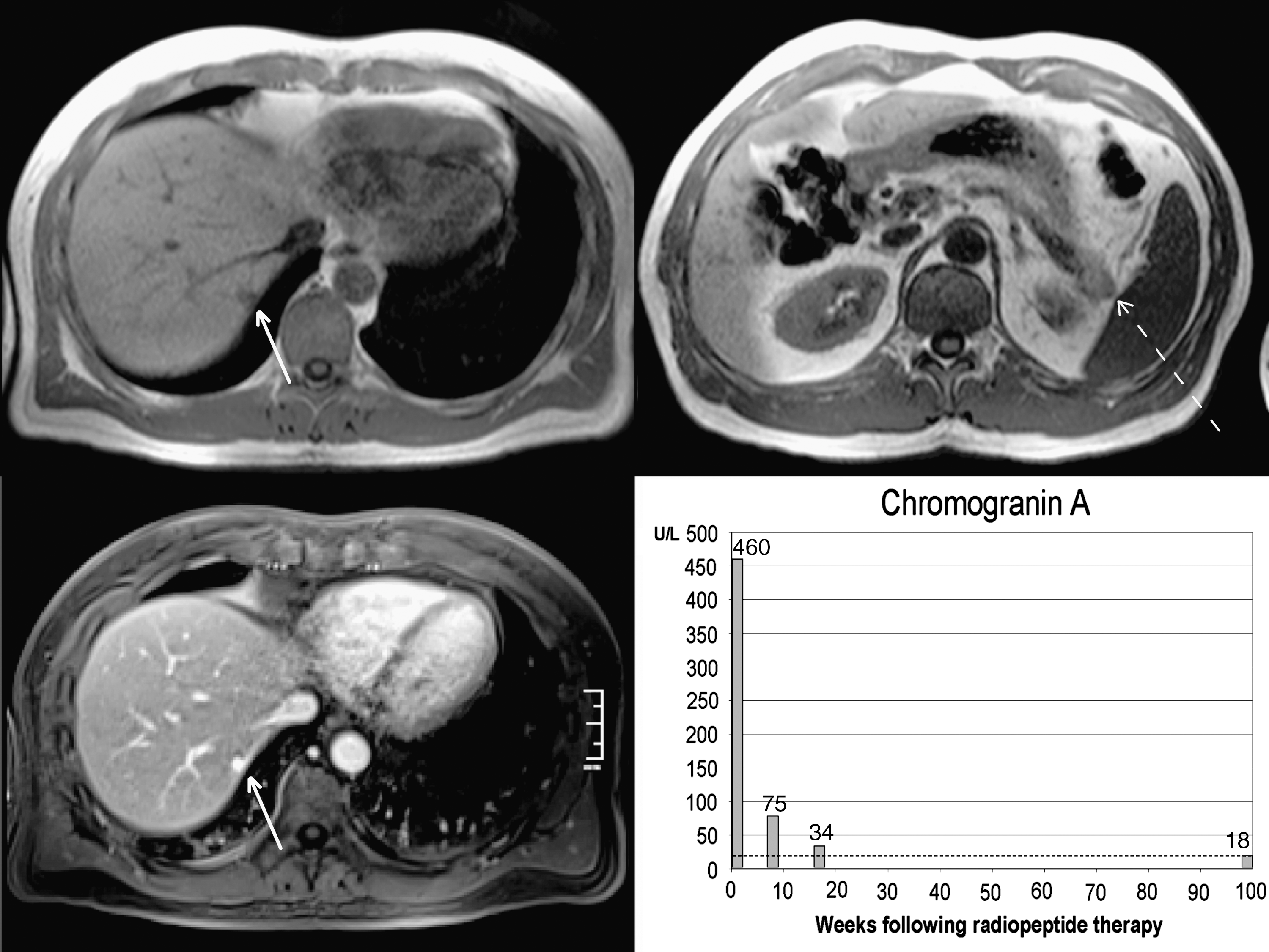
Follow-up MRI May 2012 18 months after 4 cycles of 177Lu-octreotate, capecitabine, and temozolomide radiopeptide therapy demonstrated the disappearance of hepatic metastases, which is consistent with a complete objective response. The hemangioma (short arrow) remains. A small residual region of low T1 signal persists in the tail of the pancreas at the site of the primary tumor (interrupted arrow). Chromogranin A level fell promptly after radiopeptide therapy and remains normal after 18 months, indicative of a complete biochemical response.
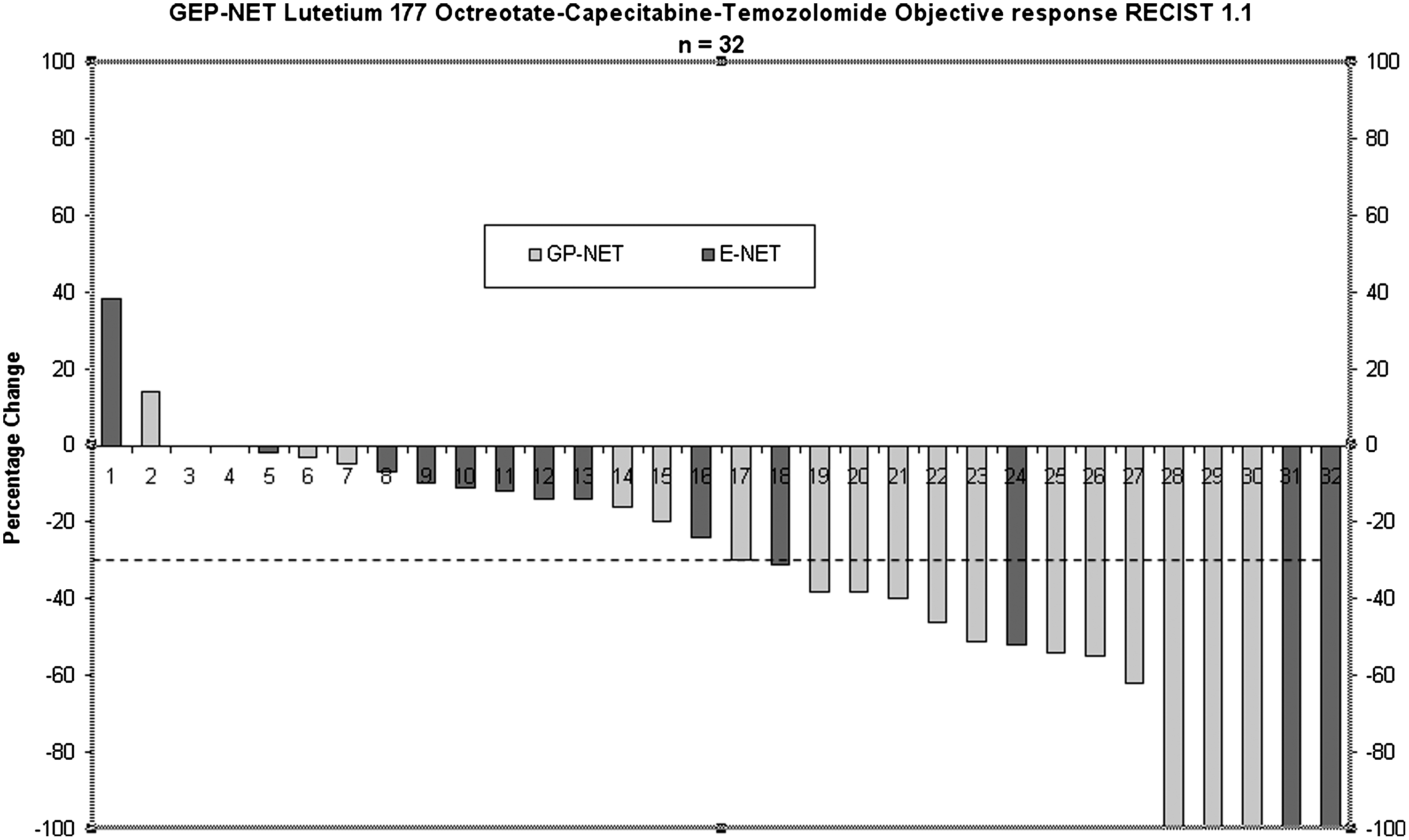
Waterfall plot of gastroenteropancreatic (GEP)-NETs (grey: gastro-pancreatic; black; enteric) showing reduction in the size of primary and metastatic tumors 6–12 months after 177Lu-octreotate, capecitabine, and temozolomide radiopeptide therapy. Objective response measured on CT/MRI according to RECIST 1.1 shows partial response (PR) as ≥30% tumor shrinkage. PR was achieved predominantly in gastro-pancreatic NETs. Five out of the 32 GEP NET patients achieved complete remission (CR) on RECIST criteria.
An example of CR in a patient with PNET is illustrated in Figures 2, 3, and 4.
Five patients had no detectable disease on follow-up CT/MRI and, thus, achieved CR on objective response RECIST criteria. However, 3 of these patients had residual metabolic activity at the tumor site on 68Ga-octreotate PET or 177Lu-octreotate SPECT imaging (Table 2). Discordant objective response and metabolic response assessment occurred in 3 other patients, in 2 of whom 177Lu-octreotate was graded PR; while RECIST was SD, and vice versa in the other patient (Table 2). Biochemical response evaluation with CgA was generally concordant with the RECIST objective response (Table 2). Subset analysis suggested a marked difference in response rates between GP-NETs and those arising from the bowel (E-NETs). Response rates were higher in patients with GP-NETs than in those with bowel primaries (E-NETs); CR 18% versus 13%, PR 64% versus 13%, SD 12% versus 67%, and GP-NETs versus E-NETs, respectively. Confidence intervals were calculated as follows: GP-NET CR 18% (95% CI 0–36), PR 64% (95% CI 42–87), SD 12% (95% CI 0–27), and PD 6% (95% CI 0–17). For E-NETs, the confidence intervals were CR 13% (95% CI 0–31), PR 13% (95% CI 0–31), SD 67% (95% CI 43–91), and PD 7% (95% CI 0–19). No significant difference was observed in median PFS. Biochemical response (CgA), metabolic response (68Ga-octreotate PET), and objective response (CT/MR RECIST) were concordant (Table 2) but not identical. However, it should be remarked that the trial was not designed or powered to make a reliable comparison between these subgroups.
At the time of the analysis, 3 deaths (9%) had occurred, all due to disease progression; consequently, median survival has not been reached. The remaining 31 patients are alive, with 90% surviving at 24 months follow-up (range 21–30 months) The median PFS was 31 months (95% CI 21–33 months) with an estimated PFS at 24 months of 77% (95% CI 49–91%) (Fig. 6).
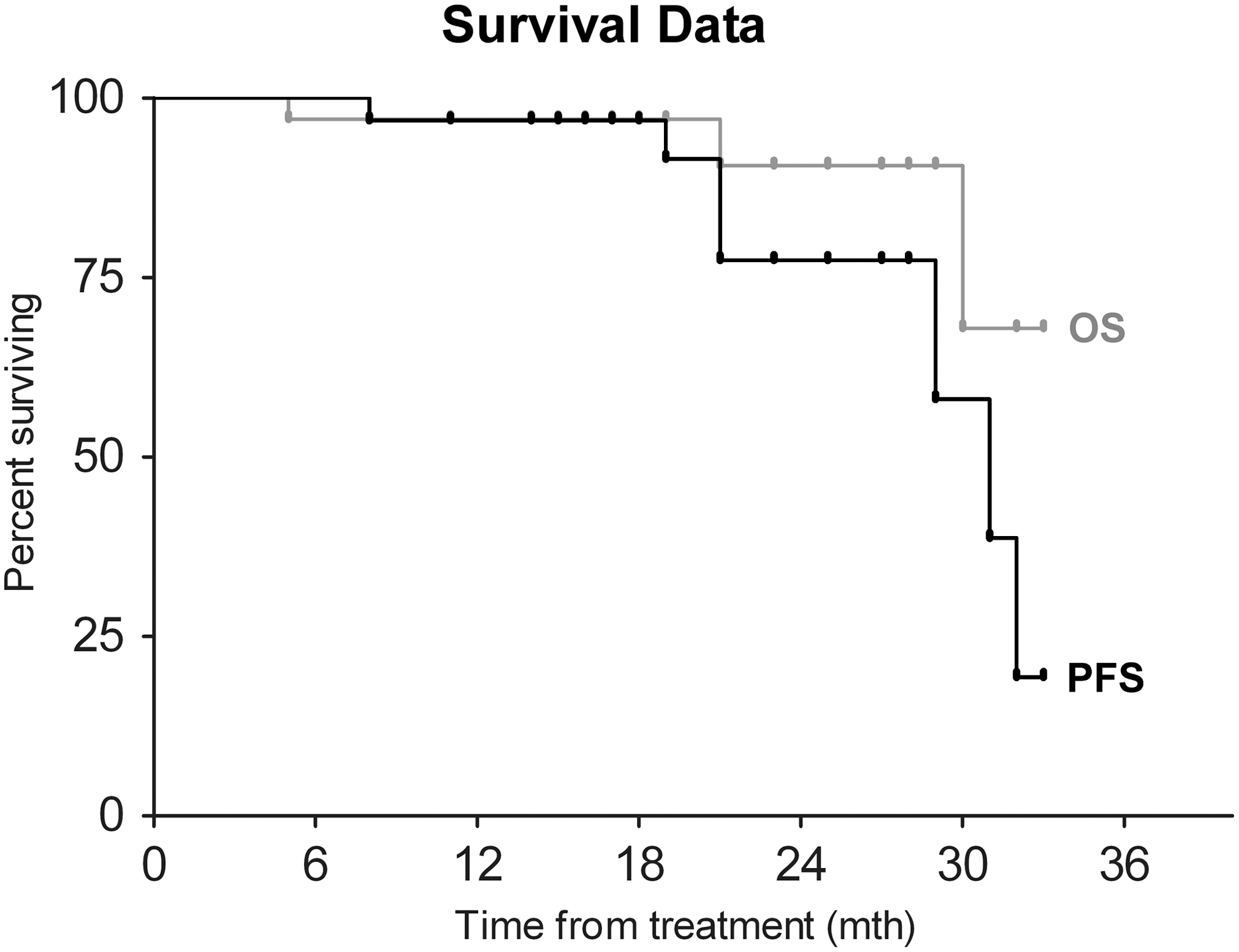
Kaplan–Meier plot of progression-free (PFS) and overall survival (OS) after 177Lu-octreotate, temozolomide, and capecitabine radiopeptide therapy in 34 patients with well-differentiated, progressive disseminated NETs. OS 97% survival at 12 months (95% CI 81–100). OS 90% survival at 24 months (95% CI 64–98). Median PFS 31 months (95% CI 21–33).
Discussion
NETs are a diverse group of malignancies arising in different anatomical locations, and manifest variable clinical behavior and responsiveness to therapies. Surgical resection is the only curative treatment, but is not possible in the common situation of presentation with widely metastatic disease. While these tumors tend to have a slowly progressive course, ultimately patients may suffer from the complications of uncontrolled hormone secretion and usually succumb to fatal tumor progression. Median survival rates for advanced PNETs are 30 months, and for carcinoids, they are 65 months. 19 Therapeutic molecular targeting of NETs is under active investigation with receptor-directed radiopeptides, mTOR inhibitors, and VEGF receptor pathway inhibitors now being well-established therapeutic options. Many of these treatments do not display substantial cytoreductive properties, but can achieve impressive clinical benefit, in both symptom control and freedom from progression. 2,20,21 In keeping with the emerging paradigm of tumor stabilization, it is now generally accepted that long-term tumor control, as measured by PFS, is the best primary endpoint for clinical studies of NETs therapy. Delay in progression is often achieved without significant radiologically defined responses. 22 However, it should also be noted that most studies also show that substantial improvements in tumor mass, qualifying under RECIST criteria as complete and PRs, generally lead to superior PFS outcomes for those few fortunate patients.
Our initial study of the radiosensitizing effect of capecitabine combined with the targeted radiopeptide 177Lu-octreotate 6 showed impressive tumor control with an ORR of 24%, and 90% of patients remained progression free at 2 years. In our current trial, we sought to build on this experience with the addition of temozolomide to the regimen. Temozolomide is an alkylating agent that is available as an oral medication. Initial clinical trials have shown activity in NET,s but responses have been largely confined to GP-NETs rather than carcinoids. 23 Tumor sensitivity to temozolomide appears to be determined by the levels of a DNA repair enzyme methylguanine DNA methyltransferase (MGMT), which is responsible for the repair of DNA methylation injury caused by temozolomide. 24 Immunohistochemical studies have shown deficient levels of the enzyme in more than 50% of GP-NETs but intact levels in virtually all carcinoids of lung and small bowel origin. These findings possibly explain the different sensitivity profiles of PNETs compared with carcinoids. Temozolomide regimens are much less effective in therapy of carcinoid than PNETs. 24 Radiographic response rate to temozolomide-based regimens has ranged from zero 25 in combination with bevacizumab, to 2% with thalidomide and other combinations. 24 Thus, it is likely that our PR rate of 27% for carcinoid patients is attributable to the radiopeptide component of the multimodality therapy; whereas the ORR of 82% in GP NETs almost certainly reflects the synergistic effect of temozolomide.
Capecitabine is thought to act synergistically with temozolomide by depleting MGMT levels before temozolomide exposure. Strosberg et al. 9 have exploited this synergy by treating a group of PNET patients with the combination of capecitabine and temozolomide. An impressive tumor PR rate of 70% and 90% survival at 2 years of follow-up was achieved, which is substantially greater than the 35% response generally reported for temozolomide alone.
In our study, we have treated both PNET and carcinoid patients, also hoping to exploit the capecitabine–temozolomide synergism and the potential radiosensitizing effects of the cytotoxics on 177Lu-octreotate. While it is always difficult to make valid comparisons with other single-arm phase II studies, our observed responses appear at least equivalent, if not superior, to Strosberg's and other targeted studies. We have achieved an ORR, according to RECIST, of 53% in the entire group and 82% in GPNETs. The median PFS of 31 months can be compared with Strosberg's reported 18 months. We were able to achieve these outcomes with only 4 chemotherapy 177Lu-octreotate cycles, given at 2 monthly intervals; whereas Strosberg's cohort received a median of 8 treatments and some patients greater than 20 cycles. Toxicities were mild for both programs with very few grade 3 or 4 events. Our results appear markedly superior to those achieved with targeted therapies. The PROMID study compared octreotide LAR with placebo in low-volume carcinoid tumors. 2 The treatment group achieved a PFS of 14.3 months. Likewise, RADIANT 2 26 compared everolimus plus LAR with placebo plus LAR with a PFS of 16.4 months in the treatment group. In our carcinoid subgroup, 27% of patients experienced a PR, and the PFS is in excess of 30 months. In PNETs, everolimus 20 and sunitinib 27 therapies produce PFS durations of around 11 months with ORR of less than 10%.
We are not able to answer the question of how much added benefit is realized by combining chemotherapy with 177Lu-octreotate. Kwekkeboom et al. 5 have published the largest study of single-agent PRRT and report a 43% PR rate for PNETs compared with our 82%, and 27% compared with 27% in our carcinoid patients. We have used PR to describe changes in tumor burden as a primary objective in our phase II screening trial of a new drug combination, and, as such, it is intended simply to describe what happens to tumor during therapy, rather than to infer a meaningful benefit from those changes. 28 The growing use of PFS as a primary end point in many randomized controlled trials of advanced solid tumors has not been based on evidence of its surrogacy for either OS or quality of life. 28 With regard to NETs, it is possible that some agents targeting cell signaling and angiogenesis, may, with chronic administration, delay progression for a time, but lead to evolutionary changes in tumors producing a more aggressive phenotype after treatment, thus offsetting the earlier delay in progression. 28
The detection of PFS is inexact, being subject to error in measurement, which does not apply to the date of death, which defines OS. In our study, all baseline and follow-up CT/MRI studies were reviewed by a single experienced radiologist, blinded with regard to the clinical outcome, who assigned ORR according to strict RECIST 1.1 criteria. The absence of a multiple-reference radiological review avoided the introduction of inter-observer variation, 29 but some measurement uncertainties remained. The edges of hepatic metastases were difficult to define in some patients, and the presence of necrosis within treated tumors may have been difficult to detect. Overall, the concordance of tumor response that was measured biochemically with CgA; metabolically by somatostatin receptor imaging with 177Lu-octreotate SPECT and 68Ga-octreotate PET; and objectively with CT/MRI according to RECIST 1.1 criteria was excellent. The minor discrepancies in 5 patients in our study may be attributed to differences in resolution of the imaging modalities. In the particular instances of PR on 177Lu-octreotate imaging immediately after cycle 4 of therapy and CR on CT/MRI definitive follow-up evaluation 6 months later, the discordance may be due to delayed response, which is not infrequently seen after radiopeptide treatment of NETs. 30 Using the combination of objective and metabolic response, we observed that the progression of disease occurred in only 9% of our patients after combined 177Lu-octreoate capecitabine temozolomide therapy in comparison with 20% progression following PRRT with 177Lu-octreotate as a single agent. 5
Conclusions
Capecitabine and temozolomide chemotherapy can be safely combined with standard therapeutic activities of 177Lu-octreotate radiopeptide for advanced NETs. The recommended dosages are capecitabine 1500 mg/m2 starting day 1 for 14 days, temozolomide 200 mg/m2 starting day 10 for 5 days, and 177Lu-octreotate 7.8 GBq starting day 5 with cycles repeated every 8 weeks over a period of a 32 week course. The majority of patients with advanced, progressive, well-differentiated NETs achieved tumor control and relief of symptoms. The response rates and PFS times in this study appear to exceed the reported results with 177Lu-octreotate as a single agent and those achieved by most targeted therapies, but await confirmation in larger comparative studies.
Footnotes
Acknowledgments
The authors wish to thank Jenny Lavin for preparation of the manuscript, Anna Chiam for clinical data management, and Ms. Suet Mei Yu for statistical analysis. The support of the the WA Cancer and Palliative Care Network is gratefully acknowledged. No grant funding or Pharma industry support was sought or received.
Disclosure Statement
No conflict of interest is declared.