
Abstract
Tumor thrombus is a rare complication of solid cancer. The authors report a case of a 76-year-old woman presenting a thick walled cystic mass in the lower lobe of the left lung. 18FDG positron emission tomography (PET)/computed tomography (CT) was performed, showing tracer accumulation in the wall of the pulmonary lesion and in the mediastinal and hilar lymph nodes. Moreover, PET/CT depicted a gross mass in the left adrenal gland and a hypermetabolic focus corresponding to the anatomic location of the left renal vein. Contrast-enhanced CT, subsequently performed, confirmed PET findings in the lung, lymph nodes, and adrenal glands, also demonstrating marginal enhancement and intraluminal filling defect in the left renal vein, which was interpreted as tumor thrombus due to the 18FDG uptake at PET scan. CT-guided biopsy of the mass was positive for poorly differentiated carcinoma. 18FDG PET can be useful to diagnose tumor thrombus in oncological patients.
Introduction
Tumor thrombosis is a rare complication of solid cancer, occurring with an incidence rate of 0.11%. 1 It has been reported mainly in cases of renal cell carcinoma, Wilm's tumor, testicular carcinoma, and hepatocellular carcinoma. 2 The differentiation between venous thromboembolism and tumor thrombosis represents a serious challenge for physicians since it has a significant impact in patient's management. An early diagnosis of tumor thrombosis, in fact, can prevent a long-term unnecessary anticoagulant treatment.
Contrast-enhanced computed tomography (CT) can be useful to identify tumoral and nontumoral thrombosis but has some limitations in specificity. 3 Magnetic resonance imaging seems to be a promising technique; nevertheless, its application in this field is still limited. 4
To date, positron emission tomography (PET)/CT represents the most readily multimodality imaging method. It has been successfully applied in many oncological settings. 5 Due to the rarity of the condition, sporadic reports have been described concerning its usefulness for the correct diagnosis of tumor thrombus.
However, recently published articles strongly suggested that 18FDG PET/CT can be useful for the diagnosis of tumor thrombus, 6,7 especially when it is used in combination with contrast-enhanced CT. 8
The authors report a clinical case showing the value of 18FDG PET/CT to diagnose tumor thrombus in the left renal vein in a patient with a gross adrenal metastasis from lung cancer.
Case Report
A 76-year-old nonsmoking woman, affected by dyspnea, weight loss, and coughing, was admitted to the Pneumology Unit of our hospital. Chest X-rays showed homogenous opacity in the left lower zone. Low-dose CT scan of the chest showed a mass with fluid density, 73×50 mm at its maximum diameter, in the inferior lobe of the left lung, close to the thoracic wall, with enlarged mediastinal and hilar nodes.
The suspicion of hydatid cyst was excluded by investigating patient's clinical history and by serological tests (i.e., indirect hemagglutination test and enzyme-linked immunosorbent assay negative for the detection of anti-Echinococcus antibodies).
Patient was subjected to whole-body 18FDG PET/CT. PET/CT scan was acquired 60 minutes after the intravenous administration of 3.7 kBq/kg of 18FDG. The PET/CT device was a Discovery ST (GE, Milwaukee, WI) with bismuth germanate crystal units arranged to form 24 rings combined with a 16-slice Light Speed Plus CT scanner. The average FWHM axial resolution of PET (full width at half maximum) is 5.2 mm and the system sensitivity is 9.3 cps/kBq for the 3D acquisition mode. Scanning was performed from the neck to the proximal tight in 3D modality, with an acquisition time of 3 minutes per table position. Images were reconstructed using an ordered subset expectation maximization iterative algorithm (OSEM-SV, VUEPoint HD, GE, 2 iterations, 15 subsets). The CT was performed immediately before PET in the identical axial field of view using a standardized protocol consisting of automatic tube current modulation with auto-milliampere, tube rotation time of 0.5 seconds/rotation, and slice thickness of 3.75 mm. The CT data were resized from 512×512 to 256×256 matrix to match the PET data. The data were transmitted to a nuclear medicine database, fused, and displayed using a dedicated software (Advantage; GE).
As reported in Figure 1, PET images demonstrated 18FDG uptake within the wall of the mass and in the hilar and mediastinal nodes. Moreover, PET scan revealed a gross mass in the left adrenal gland (Fig. 2), two lymphadenopathies in the left upper quadrant of the abdomen, and a focus of increased uptake corresponding to the anatomic location of the left renal vein, suggestive for tumor thrombus (Fig. 3A).
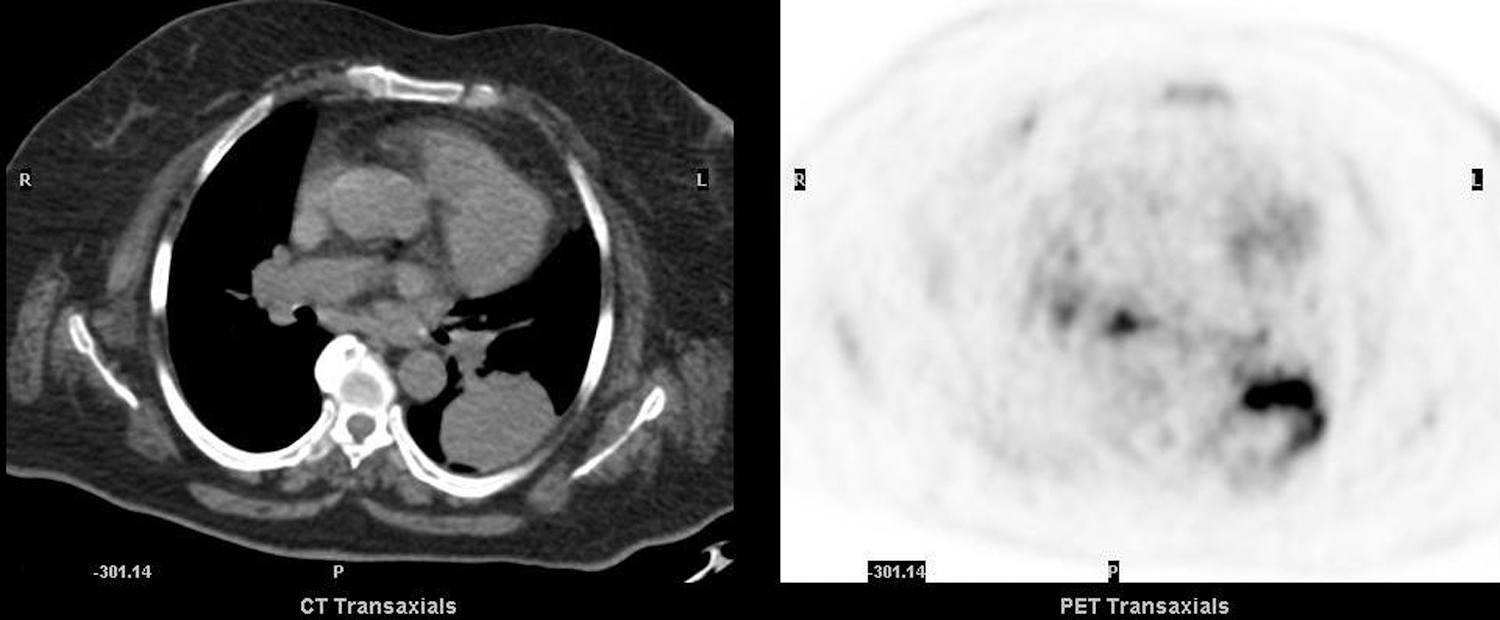
18FDG positron emission tomography (PET) transaxial slice showed tracer uptake in the wall of the pulmonary mass (SUV max: 21.5) and in mediastinal nodes (SUV max: 12.5).

18FDG PET transaxial slice depicted a gross mass in the left adrenal gland, interpreted as metastasis from lung cancer. The tumor area (triangulation) presented a necrotic core surrounded by a hot semicircular region (SUV max: 22.3).
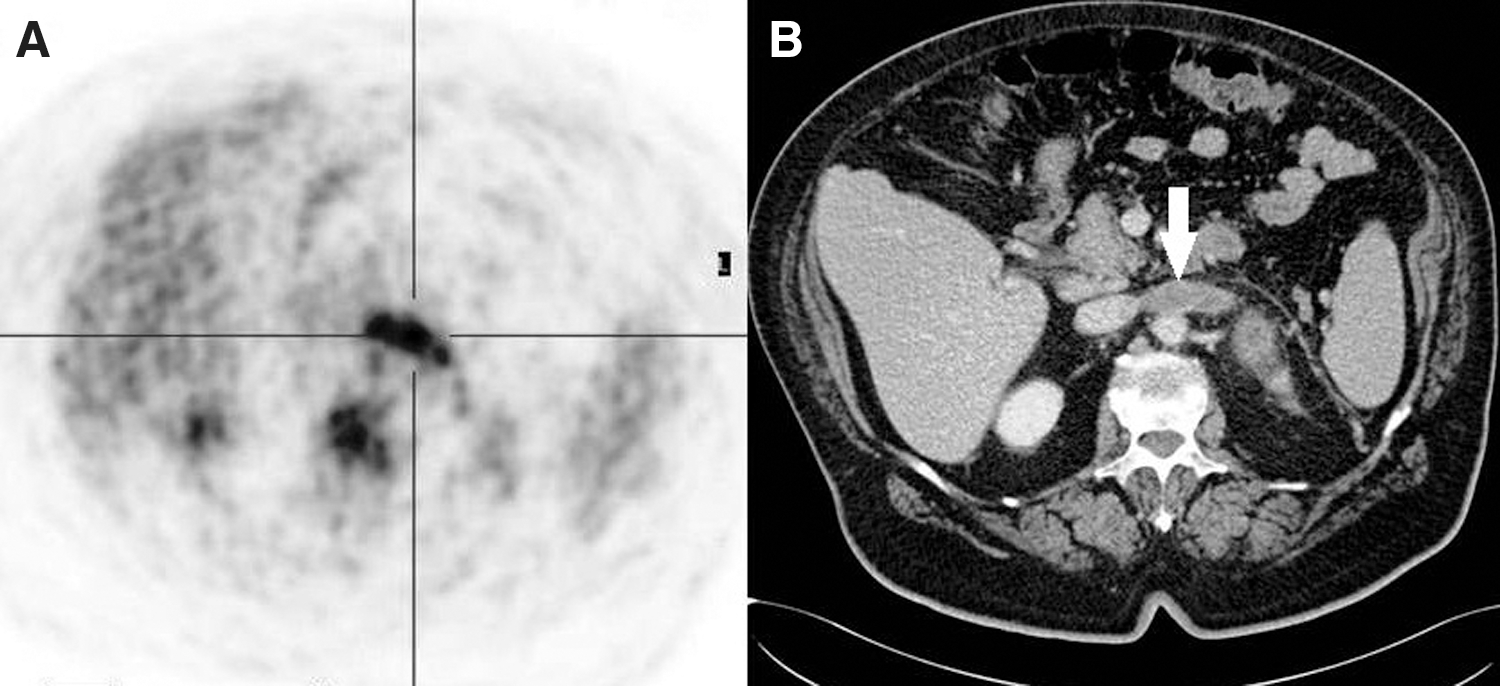
18FDG PET transaxial slice showed intense tracer uptake corresponding to the anatomic location of the left renal vein
Contrast-enhanced CT, subsequently performed, confirmed PET findings concerning lung cancer with metastases in thoracic and subdiaphragmatic lymph nodes and in the left adrenal gland, also demonstrating marginal enhancement and intraluminal filling defect in the left renal vein (Fig. 3B), which was interpreted as tumor thrombus due to the 18FDG uptake at PET scan. The patient was subjected to a CT-guided biopsy.
After routine paraffin fixation (4% buffered formalin) and paraffin embedding, the biopsy specimen was histopathologically examined. The slides stained with hematoxylin and eosin revealed necrotic tissue with rare and small foci of poorly differentiated carcinoma (Fig. 4). At present, the patient is receiving chemotherapy according to standard clinical protocols.
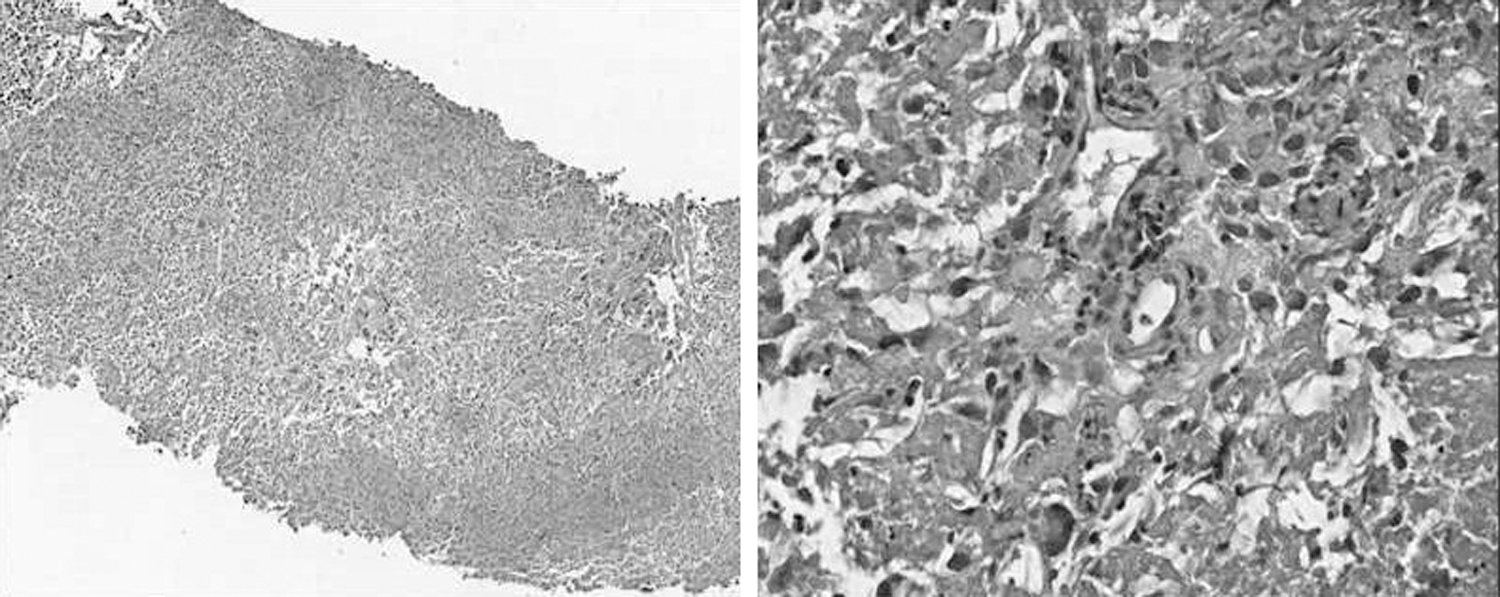
Histopathological examination of the biopsy specimen showed necrotic tissue with rare and small foci of poorly differentiated carcinoma (10× and 40×).
Discussion
Venous thromboembolism is a well-known and relatively frequent complication in oncological patients. 9 On the contrary, tumor thrombus is a rare complication. 1 It is composed of both tumoral and thrombotic components, and it is more often observed in subdiaphragmatic malignancies. In particular, it presents a significant association with renal cell carcinoma involving the renal vein and the inferior vena cava. 10 Tumor thrombus can be partially adherent and occasionally can migrate proximally reaching the right atrium. 11
Differential diagnosis between tumor and benign venous thrombosis in oncological patients still represents a challenge for physicians. Contrast-enhanced CT can be useful to demonstrate thrombosis by detecting the filling defect and dilation of the venous segment involved. However, these signs are not specific and might be observed in both venous and tumoral thrombosis. 3 Sometimes, the angiographic phase of dynamic contrast-enhanced CT may reveal hypervascularity corresponding to the thrombotic mass, thus suggesting its neoplastic origin.
Davidson et al. 6 evaluated the contribution of 18FDG PET/CT in a cohort of 11 patients with suspected tumor thrombosis. PET findings were compared with contrast-enhanced CT or ultrasound Doppler or pathology, when available. Eight occult sites of tumor thrombus were disclosed by PET/CT with an accuracy of 100%. Three patients had thrombotic lesion on CT scan coupled with negative PET findings: 2 resulted venous thrombosis and 1 leiomyomatosis, pathologically proven.
In a recent report, Lee and Khong 8 retrospectively evaluated the additional value of 18FDG PET respect to contrast-enhanced CT for tumor thrombus detection, also using semiquantitative analysis. The authors found that PET/CT is able to differentiate tumor from bland thrombosis; moreover, they demonstrated that the difference between tumor and bland thrombus SUV max was statistically significant with an optimal cut-off value of SUV max of 2.25. In this case, the authors described that the SUV max corresponding to anatomic site of the renal vein was 15.9, much higher than the cut-off value reported by the Lee group.
Mudalsha et al. 12 described a patient with extensive tumor thrombus in the inferior vena cava due to a gross adrenal metastasis from lung cancer: patient presented dilated superficial abdominal veins and pain in the lower limbs. The inferior vena cava resulted partially obstructed by the thrombotic mass extending from the third lumbar vertebra to the right atrium. To the best of knowledge, this case is the first report of a tumor thrombus in the renal vein detected by 18FDG PET/CT in a relatively early and nonsymptomatic phase.
The well-known limit of PET/CT is depicted by its relatively low spatial resolution so that small tumor thrombus may be missed. Moreover, false-negative results can arise in tumors that are non-FDG-avid.
Since 18FDG accumulates in both malignant and inflammatory cells, septic thrombus may cause false-positive results. Previous reports suggested that septic thrombus presents high tracer uptake, whereas aseptic thrombus does not accumulate 18FDG. 13,14 Only clinical examination and laboratory tests can aid the differential diagnosis between tumor and septic thrombus in an oncological patient. The patient had normal white cell counts, no elevation of the inflammation markers, and no clinical evidence of sepsis. Therefore, the hypothesis was that the adrenal metastasis might have led to the constitution of the tumor thrombus in the left renal vein.
Further studies with larger series might better define the role of PET/CT for the correct characterization of thrombosis in oncological patients, especially when a differentiation between septic and tumoral thrombus is needed.
Footnotes
Disclosure Statement
There are no existing financial conflicts.