
Abstract
Background:
Histone deacetylase (HDAC) inhibitors have been shown in preclinical studies to upregulate norepinephrine transporters in neuroblastoma and pheochromocytoma, and somatostatin receptors in pulmonary carcinoid, small cell lung cancer, and pancreatic neuroendocrine malignancies. This pilot imaging study in humans focuses on midgut neuroendocrine carcinoma metastatic to the liver, evaluating the effect of pretreatment with the HDAC inhibitor vorinostat on uptake of 123I-MIBG and 68Ga-DOTATOC.
Materials and Methods:
Multiple midgut neuroendocrine liver metastases in clinically stable subjects were imaged with 123I-MIBG and 68Ga-DOTATOC before and after a 4-d course of vorinostat. Scans were performed with strict attention to detail and timed about 1 month apart occurring just before monthly long-acting octreotide administrations. Uptake changes in tumor and normal liver parenchyma were assessed on positron emission computed tomography (PET/CT) with standardized uptake values and on single photon emission computed tomography (SPECT) with qualitative ratio images.
Results:
The experimental units were metastatic liver lesions within patients (n = 50). There was no significant difference in administered activity or uptake time between pairs of scans for either radiotracer. Statistically significant increase in maximum standardized uptake values (SUVmax) averaged over all lesions was noted on the 68Ga-DOTATOC PET scans (+11%, p < 0.01). SUVmax in normal liver showed no significant change (p = 0.12). There was no qualitative change in uptake of 123I-MIBG after vorinostat.
Conclusions:
In this pilot imaging study in patients with midgut neuroendocrine liver metastases, a short course of the HDAC inhibitor vorinostat induced a statistically significant increase in SUVmax on 68Ga-DOTATOC PET/computed tomography (CT) imaging in some hepatic neuroendocrine tumor metastases. There was no significant effect of vorinostat on tumor uptake of 123I-MIBG on SPECT/CT imaging. Given the pilot nature of this trial, the findings merit further investigation with a more rigorous protocol evaluating longer pretreatment and different dosages of vorinostat or other HDAC inhibitors, as well as effects on the therapeutic capability of 177Lu- or 90Y-somatostatin analogs.
Introduction
Neuroendocrine tumors (NETs) comprise a family of malignancies whose incidence has seen a dramatic fivefold increase over the past three decades. 1 Nearly half of patients demonstrate regional or distant disease at presentation. The median 5-year survival for distant disease ranges from 28% to 69% depending on the site of origin. 2 For patients with small intestine NETs, few systemic therapeutic options are available because these tumors are typically resistant to chemotherapy and the most widely used systemic therapy (somatostatin analogs) are prescribed primarily to ameliorate symptoms (e.g., diarrhea, flushing).
Targeted radionuclide therapy has long been considered a potential alternative systemic therapy for patients with NETs. The promise of this approach is precise targeting of cytotoxic radiation dose to tumor cells, with limited adverse side-effects. 3 Thus, targeted radionuclide therapy has the potential to circumvent NET drug resistance to conventional chemotherapy, while improving quality of life for NET patients. 3
It is widely recognized that radiolabeled peptide 90Y-DOTA-tyr3-Octreotide (90Y-DOTATOC) and 177Lu-DOTA-Octreotate (177Lu-DOTATATE) targeting predominately the somatostatin receptor subtype 2 (SSTR2) are effective for targeted radionuclide therapy of NET in adults and children. 3 –5 Although less well established, other authors have also demonstrated the potential value of 131I-meta-iodobenzylguanidine (131I-MIBG) therapy for midgut NETs in a somewhat smaller fraction (50%–70%) of patients. 6,7 However, the efficacy of either 90Y-DOTATOC, 177Lu-DOTATATE, or 131I-MIBG individually is limited by internal normal organ dosimetry relative to the amount of radiation that can be delivered to the patient's tumors. 3 Enhancing tumor uptake of these therapeutic radiopharmaceuticals has the potential to improve their efficacy. Consequently, studying methods for improving the tumor concentration of these agents relative to normal tissues has become very important.
Histone deacetylase (HDAC) inhibitors have gained interest recently for their ability to increase expression of cell surface norepinephrine transporters in neuroblastoma and pheochromocytoma and somatostatin receptors in pulmonary carcinoid and pancreatic NET. 8 –15 The norepinephrine transporter is known to be highly expressed in ∼60% of midgut NETs. 7 The ability to substantially increase norepinephrine transporter expression could notably improve the effectiveness of 131I-MIBG therapy in patients with NETs. Likewise, the ability to increase the somatostatin receptor expression in NETs could lead to improved efficacy for therapeutic agents such as 90Y-DOTATOC and/or 177Lu-DOTATATE.
Establishment of midgut NET cell lines has been challenging and availability of these lines is limited. 16 In this pilot study in humans, the authors tested whether the HDAC inhibitor vorinostat could increase the uptake of the norepinephrine transporter and SSTR2 receptor-based radiotracers through imaging with 123I-MIBG single photon emission computed tomography/computed tomography (SPECT/CT) and 68Ga-DOTATOC positron emission computed tomography (PET)/CT.
Materials and Methods
Study design and patient selection
The study was approved by the Institutional Review Board. Enrollment was voluntary. All 5 subjects provided written informed consent. Subjects living more than 20 miles away were compensated for car mileage at the standard reimbursement rate and were compensated for a total of two nights lodging during their participation in the study. At the time of the study, 68Ga-DOTATOC was utilized with oversight by the Food and Drug Administration under an Investigational New Drug Application (IND114398). Regularly scheduled safety assessments were performed as required under IND.
The study was a prospective, single-institution trial in humans consisting of a test-retest methodology evaluating change in liver tumor uptake of 68Ga-DOTATOC PET/CT and 123I-MIBG SPECT/CT before and after oral administration of vorinostat (suberoylanilide hydroxamic acid). Subjects were enrolled and scanned between March and August 2016. Each subject underwent baseline scans with each radiotracer before vorinostat and then underwent the same set of scans after a short course of oral vorinostat. Strict attention was given to relationship of scans to patient preparation, somatostatin analog administration, radiotracer quantity and timing, and scan acquisition on the same scanner to minimize differences in imaging conditions. Figure 1 shows a diagram of the imaging and medication administration schema.
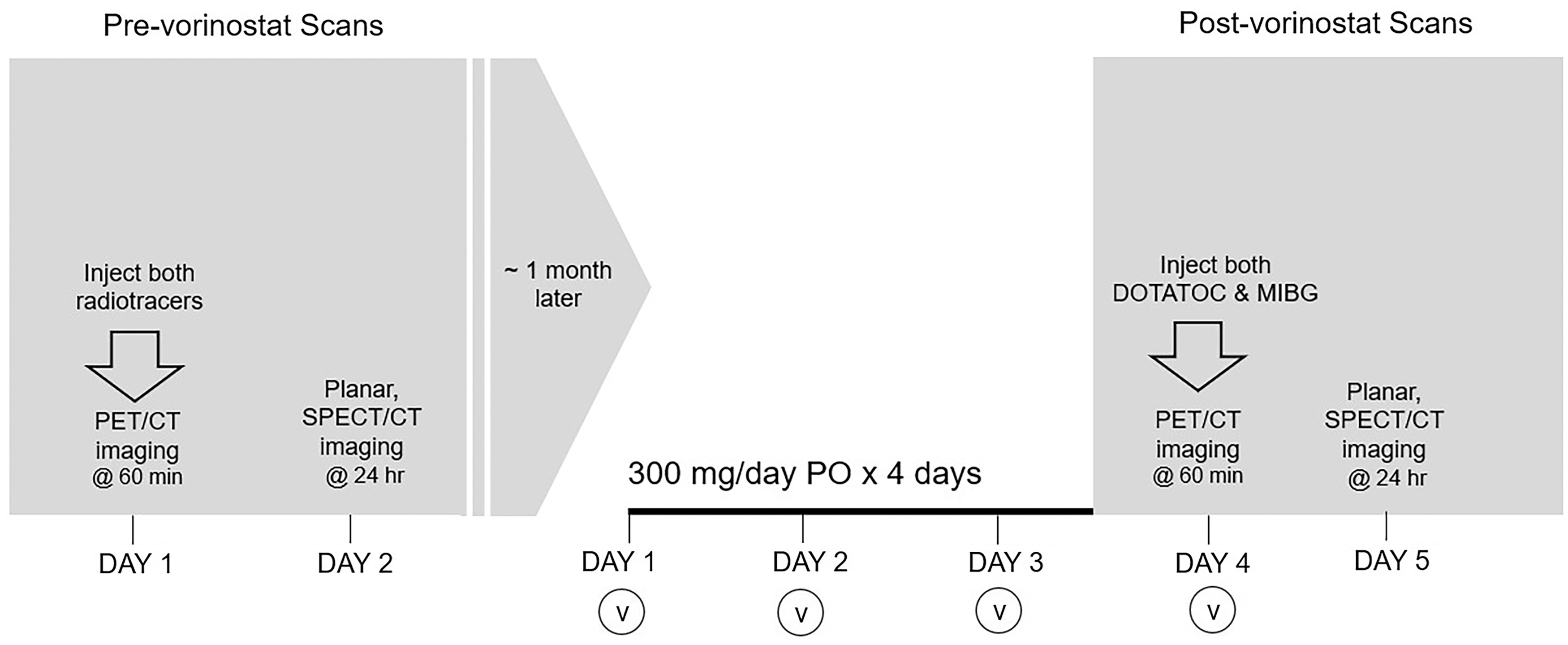
Diagram of protocol for imaging and vorinostat administration. CT, computed tomography; PET/CT, positron emission computed tomography; PO, per os; SPECT, single photon emission computed tomography; v, vorinostat.
Patient and lesion characteristics are listed in Table 1. Five subjects with clinically stable metastatic midgut NET, including at least one liver metastasis measuring ≥2 cm were evaluated. If patients were on monthly long-acting release (LAR) octreotide acetate (Sandostatin® LAR Depot) they were required to be on the same dose for at least 3 months to assure steady state levels before the first scan. Exclusion criteria included (1) known receptor negative disease based on somatostatin receptor-based PET/CT imaging, (2) prior radionuclide therapy with 131I-MIBG or 90Y-DOTOTOC or 177Lu-DOTATATE within 1 year of enrollment, and (3) current or prior treatment with HDAC inhibitors (including vorinostat, valproic acid [VPA] and derivatives, romidepsin, and other HDAC inhibitors currently undergoing clinical trials).
Subject and Tumor Characteristics
Per 2017 WHO Classification of Tumors of Endocrine Organs.
Cases are assessed for extent (%) and intensity (3+, 2+, 1+, 0) of membrane staining. Positive indicates >10% of tumor cells stain; indeterminate indicates 1%–10% of tumor cells stain with moderate or strong intensity; negative indicates <1% of tumor cells stain. 22
Equal to (minimal), slightly greater than (mild), moderately greater than (high), markedly greater than (very high) intensity of liver parenchyma.
SSTR2A, somatostatin receptor subtype 2A; SUVmax, maximum standardized uptake values; WHO, World Health Organization.
Patient preparation and medications
Scans and octreotide administrations were carefully coordinated to minimize variability. For subjects on continuous octreotide infusion (2 subjects), the night before the 68Ga-DOTATOC PET/CT, the infusion was stopped; a subcutaneous bolus of short-acting octreotide (200 μg) was given at that time and again in the morning if needed, up until 6 h before the 68Ga-DOTATOC injection. Subjects followed the same timing for infusion cessation and bolus administration for each of their scans. The remaining 3 subjects were on monthly LAR octreotide intramuscular injections with their monthly injection scheduled to occur immediately after the 68Ga-DOTATOC PET/CT scan. Unlike the subjects on continuous infusion, these subjects did not require short-acting octreotide boluses for symptom control.
Oral saturated solution of potassium iodide was administered 1 h before injection of 123I-MIBG per routine protocol. Subjects were not on medications known to interact with 123I-MIBG. Subjects were asked to abstain from over-the-counter sympathomimetics drugs given the potential for interaction with 123I-MIBG.
Vorinostat was obtained from the manufacturer and supplied through the institution's investigational drug services pharmacy. Before the second scan, subjects self-administered vorinostat (300 mg orally with food in the morning) for 4 consecutive days. On the fourth day of vorinostat dosing, subjects presented to the nuclear medicine department for their follow-up imaging studies. Vorinostat at 300 mg rather than 400 mg (FDA-approved maximal dose) was chosen to reduce side-effects.
Radiotracers, scan acquisition, and reconstruction
68Ga-DOTATOC was manufactured on-site under IND using methods previously described in the literature. 17 Target administered activity was 148 MBq (4 mCi) followed by target uptake time of 60 min. Each subject's PET scans were performed on the same PET/CT scanner, Siemens Biograph 40 (Siemens Healthcare). To reduce radiation exposure, scans were limited to the upper abdomen, taking care to include the entire liver. Scans were obtained at 4 min per bed position. Images were reconstructed onto a 168 × 168 matrix using three-dimensional (3D) ordered subset expectation maximization using four iterations, eight subsets, and a 7 mm Gaussian filter.
Unit doses of 123I-MIBG (AndreView®; GE Healthcare) were obtained from a commercial vendor. Target administered activity was 370 MBq (10 mCi) followed by target uptake time of 24 h. Each subject's pre- and postvorinostat SPECT/CT scans were performed on the same scanner, Symbia T 2-slice SPECT/CT (Siemens Healthcare) and with the same technique. Scans were centered on the upper abdomen, taking care to include the entire liver. The SPECT study was acquired with a total of ninety 128 × 128 projection views at 40 s per projection. Before reconstruction, the raw projection images were scaled by a factor of 10 to reduce integer truncation. Flash 3D iterative reconstruction was used with three iterations, six subsets, and a 12 mm postreconstruction Gaussian filter.
Lesion selection and analysis
For 68Ga-DOTATOC PET/CT, quantitative assessment of lesions and background liver was performed on MedView Display software (MedImage, Ann Arbor, MI). In each subject, 10 random lesions were selected for a total sample of 50 lesions. Ten of the lowest maximum standardized uptake values (SUVmax) lesions per subject were also selected for analysis in a separate sample of 50 lesions. Selected lesions were visually discrete (i.e., separable from other lesions), allowing for segmentation (Fig. 2). Regions of interest for normal liver were placed near each liver lesion for a total of 50 normal liver measurements. SUVmax were used for tumors, and both SUVmax and mean standardized uptake values (SUVmean) were used for normal liver.
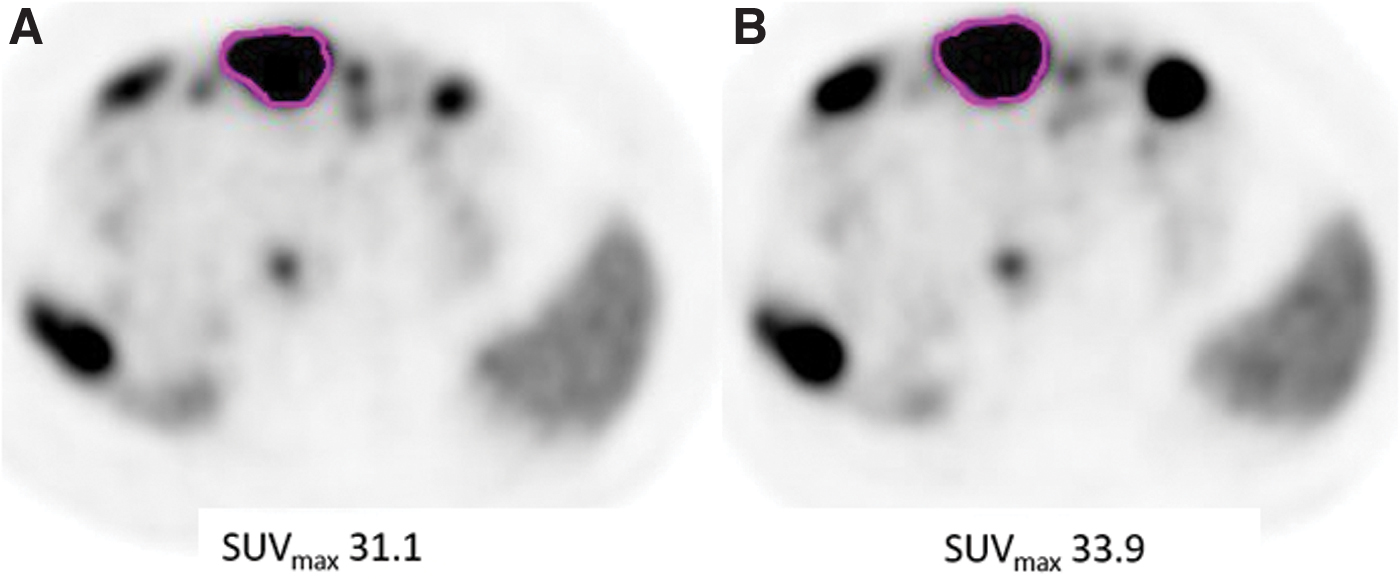
68Ga-DOTATOC PET axial plane at the level of the liver for Subject 1. Region of interest for measurement of SUVmax is drawn around a target lesion for both prevorinostat scan
For 123I-MIBG SPECT/CT, qualitative assessment of tumors was assessed on ESoft software (Siemens Medical Solutions, Erlangen, Germany). Uptake intensity of tumors compared to background liver parenchyma was categorized qualitatively with a following 4-point scale: equal (minimal), slightly greater (mild), moderately greater (high), and markedly greater (very high).
Pre- and postvorinostat SPECT images were manually registered in three planes to precisely match the contours of the liver and any visible lesions (Fig. 3). Once registered, composite SPECT ratio images were created by dividing the postvorinostat scan by the prevorinostat scan. Each pixel in the resulting composite image represented a ratio of the counts per pixel before and after vorinostat. When no discernible change in uptake occurred within a pixel, its grayscale intensity was a medium gray, centered between black and white on the color scale. Pixels in tumors with no change appeared similar in intensity to pixels of background liver parenchyma, such that the overall liver in a subject with no change in tumor uptake showed a diffuse homogenous medium gray (Fig. 4). In the setting of discernible change in uptake in tumor, the composite imaging would show pixel intensity toward the black or white poles of the color scale depending on the direction of change.
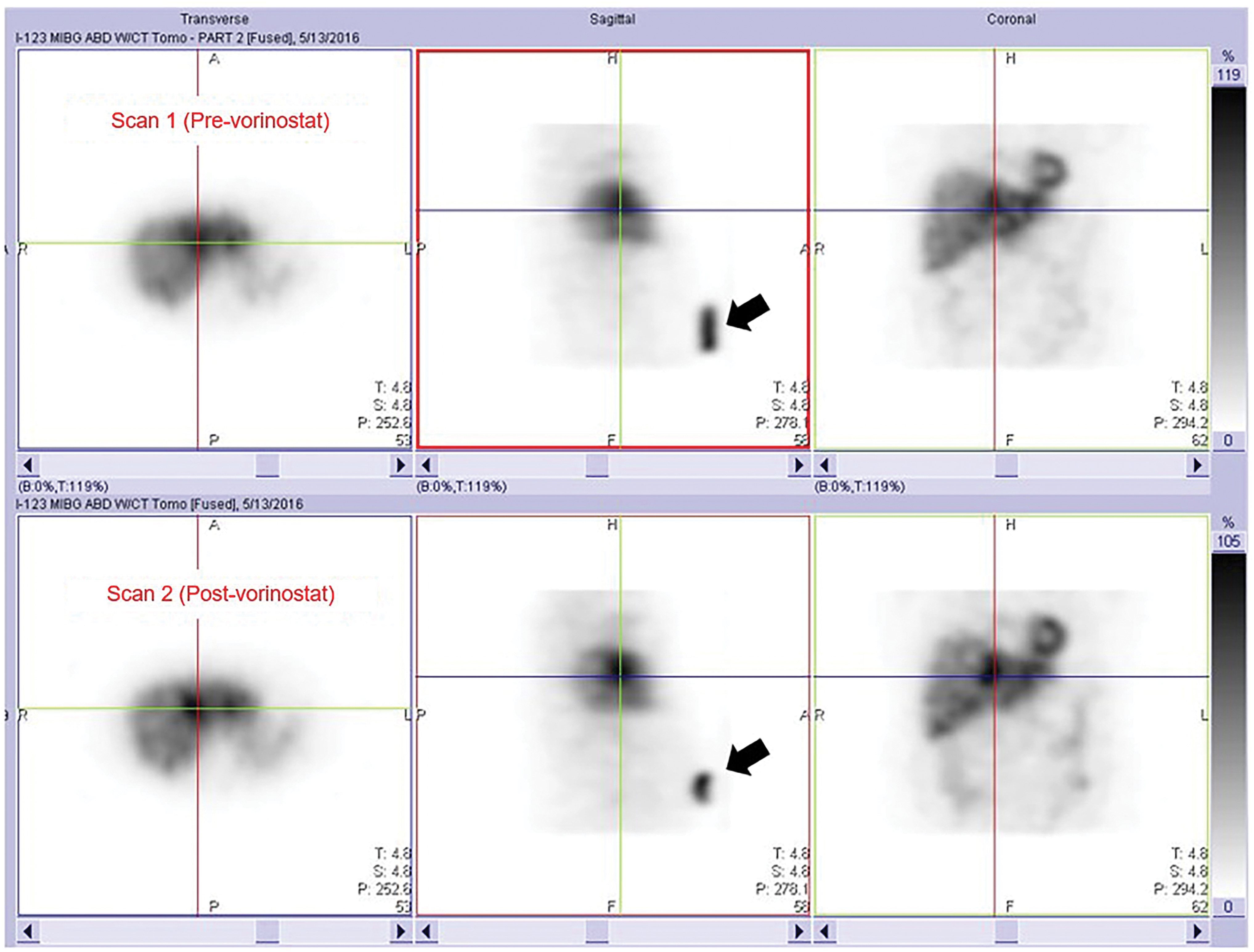
Image registration for 123I-MIBG SPECT showing axial, sagittal, and coronal planes through the liver before (top row) and after (bottom row) vorinostat. Crosshairs pinpoint a radiotracer-avid tumor in the left lobe of the liver. A quantitative standard (black arrows) was prepared and placed on the subject's lower abdomen. Ultimately, the standard was not used for data analysis during this study. Color images are available online.
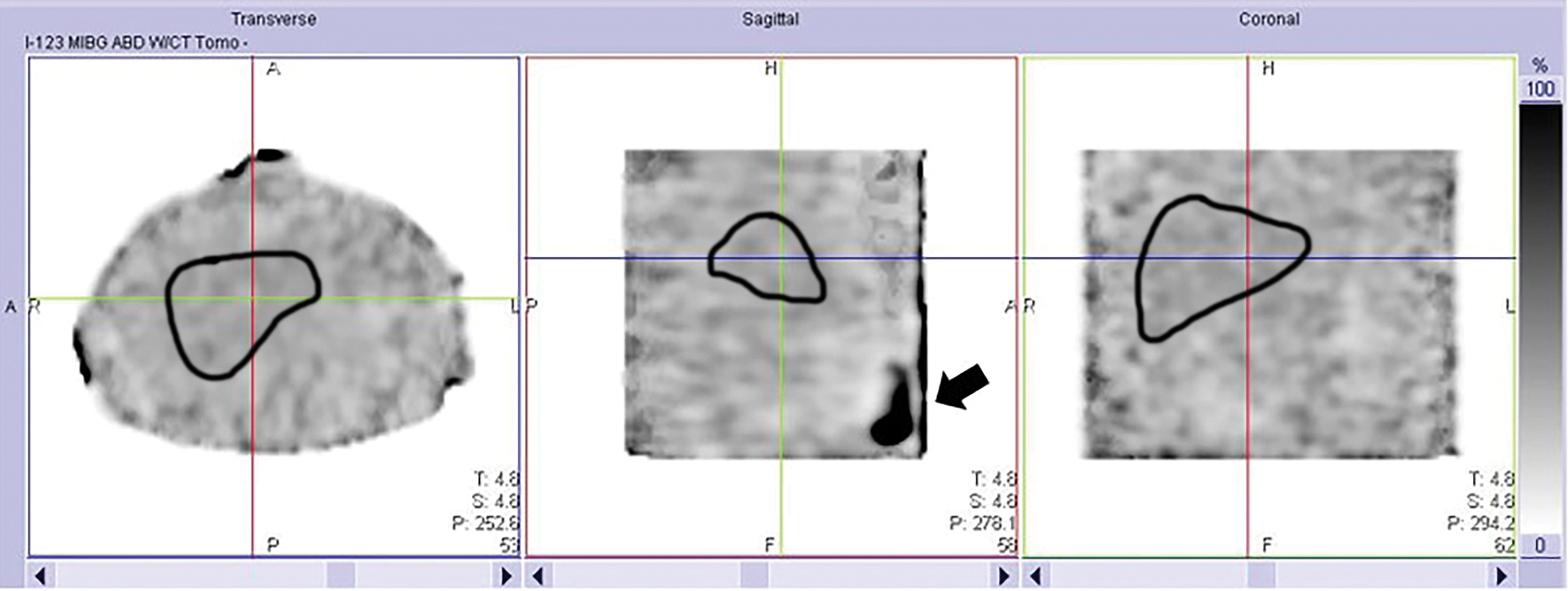
Ratio image for 123I-MIBG SPECT showing axial, sagittal, and coronal planes through the liver. Crosshairs pinpoint the site of a radiotracer-avid tumor in the left lobe of the liver (visible on the original nonratio images in Fig. 3). The outline of the liver has been added in black to each plane. The tumor at the site of the crosshairs shows an image intensity that is no different than background liver because there was no significant change in uptake between the pre- and postvorinostat scans. A quantitative standard resting on the subject's lower abdomen (black arrow) was positioned differently between the two scans (as demonstrated in Fig. 3), and thus could not be perfectly registered on the ratio image; as a result, it shows high intensity on the ratio image because of an apparent change in uptake that was artifactual. Color images are available online.
Statistical analyses
The statistical analyses were handled with lesions as experimental units and subjects treated at random. 18,19 Percentage change in SUV for lesions and normal liver was calculated as [(SUVscan2 − SUVscan1)/SUVscan1] × 100%. The SUVmax from all measured lesions was averaged to give a group mean SUVmax. The magnitude and direction of percentage change in the group mean SUVmax for pre- and postvorinostat examinations was calculated for each subject. The percentage change for all 50 lesions was averaged to obtain a final group percentage change between the prevorinostat and postvorinostat scans.
To determine if there was a significant difference in standardized uptake values before and after the administration of vorinostat medication, linear mixed effects models were applied. A compound symmetry correlation structure was used to model the possible dependency among measurements within a patient. All analyses were performed using the PROC MIXED procedure in SAS v9.4 (SAS Institute, Cary, NC).
Results
No adverse events attributable to 68Ga-DOTATOC occurred. Several grade 1 toxicities (dizziness, nausea, dry mouth, diarrhea, and hair loss) possibly attributable to vorinostat occurred. One grade 2 toxicity (hyperglycemia) possibly attributable to vorinostat occurred in a sixth subject, but this subject's data were not included in the final analysis due to a patient-related deviation in vorinostat dosing.
There was no significant difference in administered activity or uptake time between pre- and postvorinostat scans (i.e., scan 1 and scan 2). For 68Ga-DOTATOC, uptake time was 60 min exactly for both scan 1 and scan 2 for all subjects. Injected activity for 68Ga-DOTATOC ranged from 140.2 to 152.4 MBq (mean 145.4 ± 5.4 MBq) for scan 1 and 139.9 to 146.9 MBq (mean 144.4 ± 3.4 MBq) for scan 2 with p = 0.61. For 123I MIBG, uptake time ranged from 24.0 to 24.3 h for scan 1 and ranged from 23.9 to 24.1 h for scan 2; this small difference trended toward marginal significance (p = 0.08), but was not clinically significant. Injected activity for 123I MIBG ranged from 332.6 to 364.7 MBq (mean 352.9 ± 12.5 MBq) for scan 1 and 338.2 to 352.2 MBq (mean 345.9 ± 5.8 MBq) for scan 2 with no significant difference (p = 0.17).
For 123I MIBG SPECT/CT no appreciable change in tumor uptake was seen based on qualitative ratio images. For quantitative imaging with 68Ga-DOTATOC PET/CT, the experimental units were lesions within patients (n = 50). For more discussion on this methodology, see Vag et al. and Lapa et al. 18,19 Mean tumor size was 2.1 ± 1.0 cm. All but one subject demonstrated an increase in the intrasubject group mean SUVmax (Fig. 5). SUV data are presented in Table 2. There was a statistically significant increase in total group mean SUVmax of all 50 tumors after vorinostat administration (+11.4% p < 0.01) (Fig. 6).
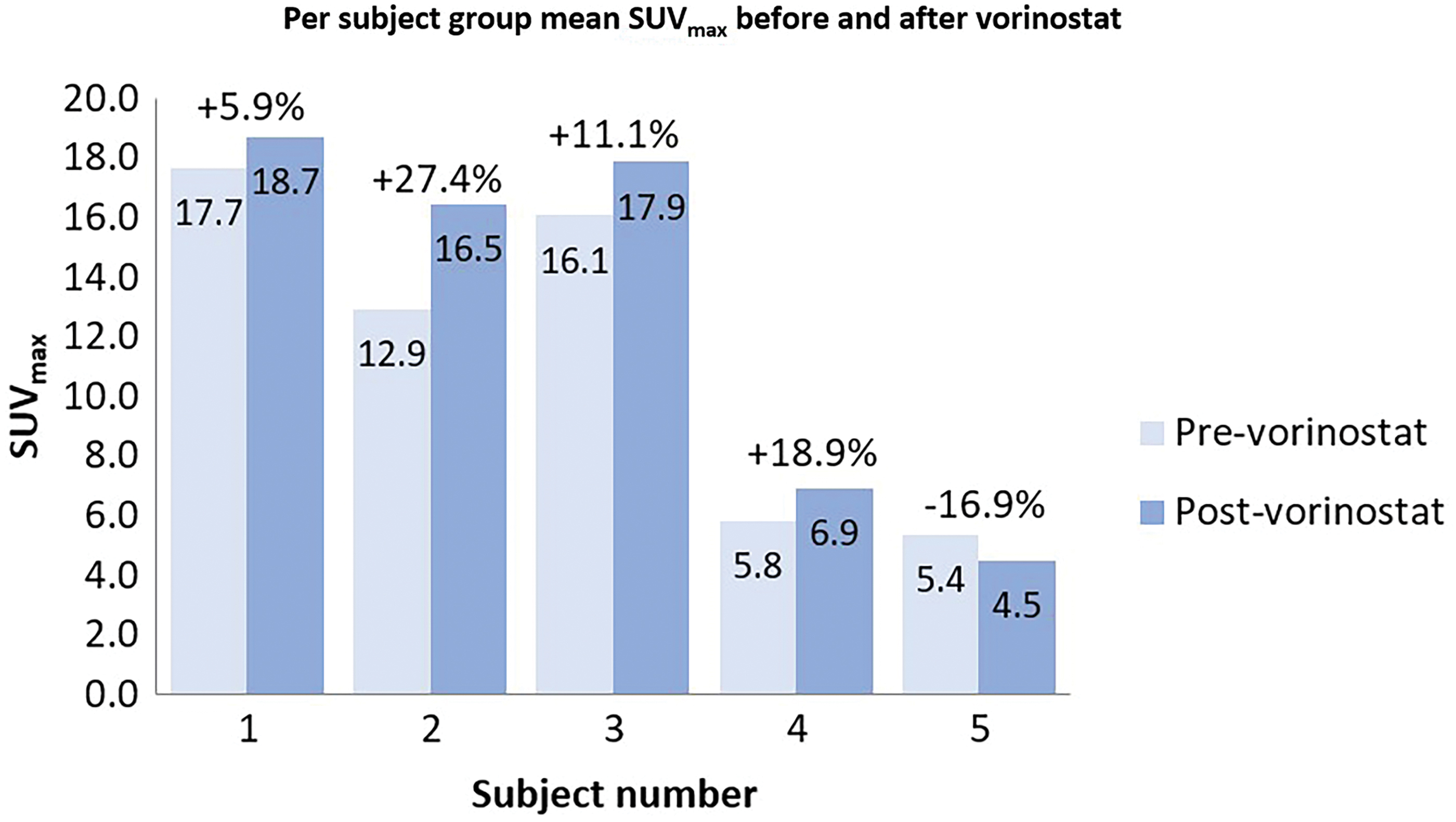
Graph comparing changes in group mean SUVmax for each subject's tumors before and after vorinostat. All but one subject showed an increase in mean SUVmax. Color images are available online.
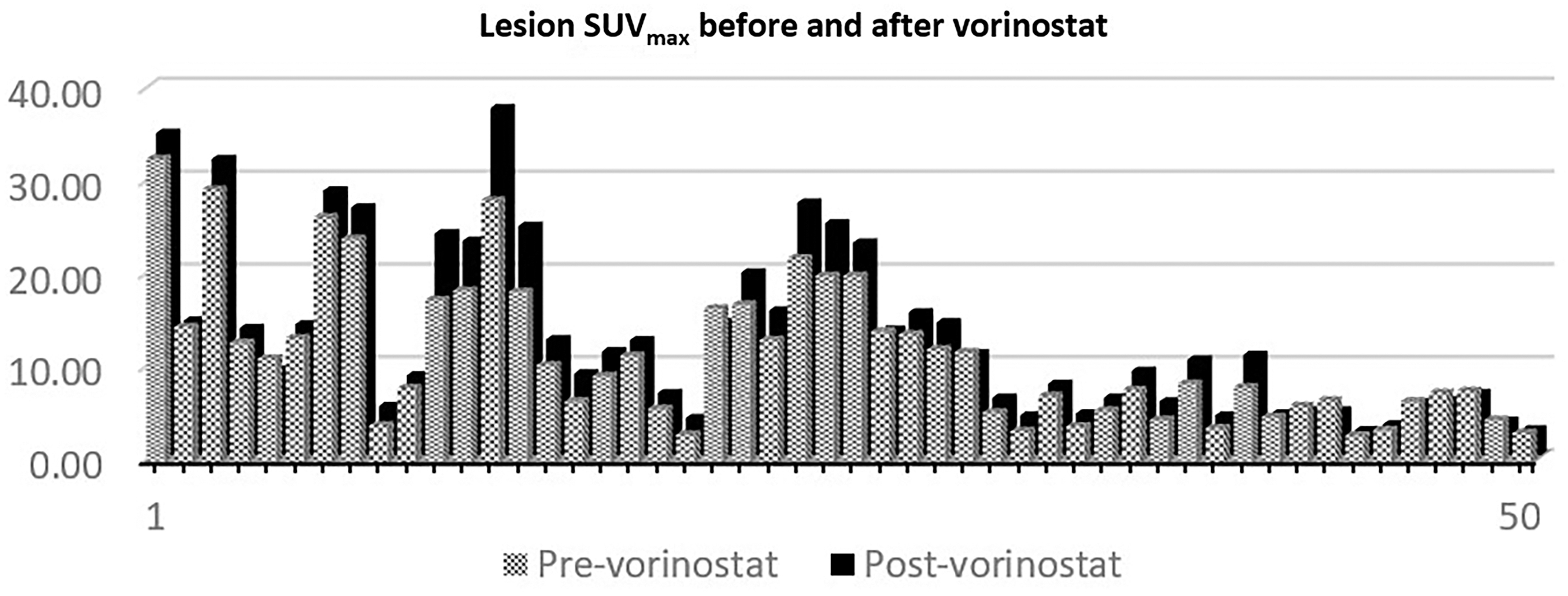
Graph comparing changes in SUVmax for each of the 50 measured tumors before and after vorinostat.
Lesion and Normal Liver Metrics
SUVmean, mean standardized uptake values.
A second sample of 50 tumors chosen specifically for their low radiotracer uptake showed a positive increase in total group mean SUVmax after vorinostat, but did not meet statistical significance (with this sample showing prevorinostat mean SUVmax 4.0, range 2.3–8.8, in contrast to the original sample of randomly selected tumors, which showed prevorinostat mean SUVmax 11.6, range 2.9–32.7). There was no significant change in normal background liver SUVmax (p = 0.12) and an increase in normal liver SUVmean that was of marginal significance (p = 0.07). There was no statistically significant difference in sizes of ROIs before or after vorinostat for normal liver (p = 0.7456).
Discussion
Imaging with peptide receptor radiotracers and therapy with peptide receptor radiotherapy is an important part of the management and therapy of patients with NET. These methods are not available, however, for the subset of patients who have diminished expression or nonexpression of the target receptors. There is growing interest in the family of drugs known as HDAC inhibitors for their apparent ability to increase expression of a number of cell surface receptors for NETs and other types of malignancies. 10,11,13 –15,20,21
The authors' pilot study demonstrated a modest but significant increase in tumor uptake of 68Ga-DOTATOC after a short course of vorinostat in some hepatic NET tumors. This appears to be in line with a number of studies showing enhanced SSTR2 expression and radioligand binding in NETs after exposure to HDAC inhibitors.
Veenstra et al. found that exposure to the HDAC inhibitor VPA increased expression of SSTR2 in pancreatic NET cell lines (BON-1 and QPG-1). 21 Taelman et al. demonstrated that an array of HDAC inhibitors increased uptake of 68Ga-DOTATOC via SSTR2, with tacedinaline showing the greatest increase in uptake. 20 Guenter et al. showed that exposure to multiple HDAC inhibitors (including romidepsin, VPA, and vorinostat) led to increase in SSTR2 protein expression in NET cells lines for pulmonary carcinoid and pancreatic NET (H727 and BON-1, respectively). 10,11 The same group also demonstrated that exposure to the HDAC inhibitor FK228 (romidepsin) led to a significant increase in tumor uptake of 68Ga-DOTATATE in small animal PET/CT imaging for BON-1 xenograft mice. 10,11 Sun et al. demonstrated that exposure to the HDAC inhibitor VPA resulted in upregulation of SSTR2 in small cell lung cancer and pancreatic NET cell lines (DMS53 and BON-1, respectively). 13,14 The Notch cellular signaling pathway is speculated to play a role in the upregulation of SSTR2 in these cancer cells. 13,14
The study has limitations. As a pilot study, the sample size was small. This was addressed by assessing multiple tumors per subject to increase the number of measurements included in analysis. There was a marginally significant increase in liver parenchymal SUVmean, which suggests that a larger sample study may be helpful.
The study evaluated a single HDAC inhibitor while there is a larger group of HDAC inhibitors that could potentially be studied. In addition, the limited duration of pretreatment with vorinostat and the nonmaximal dose that was selected for study raises the question as to whether higher doses and longer duration of pretreatment could produce a greater increase in tumor uptake than the authors observed with the subjects.
Individuals and tumors selected for assessment in this study were those with substantial radiotracer avidity; it remains to be evaluated if an HDAC inhibitor such as vorinostat could influence uptake in subjects and tumors with diminished activity. Finally, the change in uptake observed in this study is positive, but small. The magnitude of change is lower than the repeatability for 68Ga-DOTATOC, which has been estimated at ±25% SUV. 17 However, the statistical analysis found significance essentially because the change was in a positive direction in 4 of the 5 subjects.
Conclusions
This pilot study in patients with metastatic midgut NETs demonstrates that a short 4-d pretreatment course of the HDAC inhibitor vorinostat produces a quantitative increase in uptake of 68Ga-DOTATOC in some hepatic NET tumor metastases and no appreciable effect on qualitative uptake of 123I-MIBG. Given the pilot nature of this trial, the findings merit further investigation with a more rigorous protocol evaluating longer pretreatment and different dosages of vorinostat or other HDAC inhibitors, as well as effects on the therapeutic capability of 177Lu- or 90Y-somatostatin analogs.
Footnotes
Acknowledgments
The authors acknowledge the contribution of Tim Ginader, MS, to the statistical analysis. The content of this research is the sole responsibility of the authors and does not represent the official views of the National Institutes of Health.
Authors' Contributions
J.H.P., D.B., Y.M., T.O., M.S.O., M.M., and K.D.Z. discussed and designed the protocol. J.H.P. wrote the protocol, conducted the trial, coordinated the subjects, analyzed the imaging, and wrote the article. M.M. devised the approach used for analysis of SPECT imaging. K.D.Z. provided statistical support. J.H.P., D.B., Y.M., M.S.O., T.O., M.M., and K.D.Z. edited the article. All coauthors have reviewed and approved the article before submission.
Disclosure Statement
J.H.P. owns stock in Johnson & Johnson; advisory honoraria from KEOSYS Medical Imaging/Exini; investigator for AAA/Novartis and Progenics for radiopharmaceutical clinical trials relating to prostate cancer. All other authors have no conflicts of interest to declare.
Funding Information
Research reported in this publication was supported by the NIH/NCI Neuroendocrine Tumor Specialized Programs of Research Excellence (SPORE) in Human Cancer—Career Development Award under award number 1P50CA174521. Funding for subject compensation was provided through an alternate grant source.