
Abstract
Abstract
Background:
Recent research suggests that a negative relationship exists between adiposity and cognitive function in children. However, limited information is known on how they are related. This study aimed to examine the mediators of the relationship between overweight/obesity and cognitive function among school children in Kuala Lumpur, Malaysia.
Methods:
This is a cross-sectional comparison study whereby 225 overweight/obese children matched for age, sex, and ethnicity with 225 normal weight children participated in this study. Body image dissatisfaction, disordered eating, and depressive symptoms were assessed through a self-administered questionnaire. Blood pressure was measured, whereas blood was drawn to determine insulin, high-sensitivity C-reactive protein (hs-CRP), glucose, and lipid profiles. Homeostasis model assessment-estimated insulin resistance (HOMA-IR) was calculated using glucose and insulin levels. Wechsler's Intelligence Scale for Children-Fourth Edition (WISC-IV) was used to assess cognitive function in children. Ordinary least square regression analysis was conducted to determine the direct and indirect relationships between weight status and cognitive function.
Results:
A negative relationship was found between overweight/obesity with cognitive function. Overweight/obese children were on average 4.075 units lower in cognitive function scores compared to normal weight children. Such difference was found through mediators, such as body image dissatisfaction, disordered eating, depression, systolic blood pressure, triglycerides, HOMA-IR, and hs-CRP, contributing 22.2% of the variances in cognitive function in children.
Conclusion:
Results highlight the important mediators of the relationship between overweight/obesity and cognitive function. Consequently, future interventions should target to improve psychological well-being and reduce cardiovascular disease risk for the prevention of poorer cognitive performance in overweight/obese children.
Introduction
Recent research suggests that a negative relationship exists between adiposity and cognitive function in children.1–3 Literature indicates that overweight and obese children have significantly lower cognitive scores 3 ; performance in memory, reasoning, and attention 4 compared to their normal-weight counterparts. Although findings from systematic reviews and meta-analysis concluded that obesity is associated with poorer cognitive performance in children,1–3,5 there is limited information on how they were related.
Some researchers suggest that a direct relationship exists between obesity and cognitive function as the relationship was reported among subjects without serious metabolic complications.2,3 Others propose that an indirect relationship exists or that the relationship is mediated by psychological factors such as depression, lowered self-esteem, and dieting6–8 as preoccupying thoughts on body shape might have used more mental resources required for cognitive tasks. 9 Similarly, cardiovascular disease risk factors such as hypertension, dyslipidemia, or insulin resistance 2 may mediate the relationship due to endothelial dysfunction which may lead to inadequate fuel substrate in the brain during cognitive processes. 10 However, it is unclear which of these indirect relationships truly explain the relationship between obesity and cognitive function in children.
Despite the growing phenomenon of childhood obesity in Malaysia, very few studies examined the relationship between weight status and cognition in children,11,12 and none was designed specifically to examine the relationship between overweight/obesity and cognitive function. Hence, this study is designed to determine the mediating factors of the relationship between overweight/obesity and cognitive function in primary school children aged 10–11 years in Bangsar-Pudu, Kuala Lumpur, Malaysia.
Methods
Study Setting and Subjects
This cross-sectional comparison study was conducted in Bangsar-Pudu Zone of the Federal Territory of Kuala Lumpur, Malaysia. There are three educational zones in the Federal Territory of Kuala Lumpur namely Bangsar-Pudu, Keramat, and Sentul. Bangsar-Pudu Zone was randomly selected using a computerized software, and this education zone best represents Malaysia due to its mixture of ethnicity and income levels. 13 Twelve schools were selected using multistage stratified sampling method. Ethical approval was obtained from the Ethics Committee for Research Involving Human Subjects, Universiti Putra Malaysia [FPSK (FR14) P017] before the commencement of the study. Permission to conduct the study was granted by the Ministry of Education Malaysia [(KP(BPPDP)603/5/JLD.10(17)] and the Federal Territory of Kuala Lumpur Department of Education [JPNWP.900-6/1/7 Jld. 10(92)]. The purpose of the study was explained to the respondents and their parents through information sheets given. Signed informed consent was obtained from the respondents and their parents before the data collection. Data collection was carried out from July 2014 through October 2015.
Sample Size and Sampling Method
A sample size of 157 respondents 14 for each normal weight and overweight/obese group was estimated to give the study at least 80% power at 5% significance to detect a significant difference in mean scores of cognitive function between the two groups. To compensate for missing data, the estimated sample size was increased by ∼20%, which makes up a minimum of 188 respondents to be recruited for each normal weight and overweight/obese group, respectively.
A total of 1971 children aged 10–11 years were screened for BMI-for-age through measurements of height and weight and were classified as normal weight and overweight/obese using the WHO Growth Reference 2007 (BMI-for-age). 15 A sample of 225 overweight/obese children matched for age, sex, and ethnicity with 225 normal weight children consented and completed the study. No significant difference was found for monthly household income and parents' educational level between the normal weight and overweight/obese children. Inclusion criteria of the respondents were as follows: (1) age between 10 and 11 years, (2) either male or female children, and (3) healthy and not with acute disease such as fever, flu, or chronic diseases that may affect fat distribution or body composition such as Cushing's syndrome. Children with writing or speaking difficulties and those who were not fasting on the day of the data collection were excluded from the study.
Measurements
Anthropometric measurement
Body weight was measured using OMRON Body Fat Analyzer model HBF-356 (Omron Matsusaka Co. Ltd, Matsusaka, Japan) to the nearest 0.1 kg. Height was measured using a SECA Body Meter SE206 (SECA, Germany) to the nearest 0.1 cm. Both height and weight were measured twice. BMI-for-age was determined using AnthroPlus software version 10.4 and classified based on the WHO Growth Reference 2007. 15
Biochemical and Blood Pressure Measurements
After a 10-hour fast, 5 mL of venous blood sample was collected using standard venipuncture by a trained phlebotomist with an attendant nurse or physician. Fasting lipid profiles [triglycerides (TG), total cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C)], high-sensitivity C-reactive protein (hs-CRP), and fasting blood glucose were assessed using Roche Cobas E311 (Germany). Fasting blood insulin was assessed using Roche Cobas E411 Immunoassay Analyzer (Germany). All biochemical analyses were outsourced to a certified laboratory for analysis. Homeostasis model assessment-estimated insulin resistance (HOMA-IR) was determined using this formula: fasting blood insulin (mU/L) × fasting blood glucose (nmol/L)/22.5. 16 Arterial blood pressure was measured after a 5-minute rest using the OMRON Digital Automatic Blood Pressure Monitor HEM-907 (OMRON, Japan) with a suitable cuff size. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were recorded thrice after an interval of 30 seconds each, and the mean was calculated.
Body Image Dissatisfaction
The body image dissatisfaction of the children was assessed using Collin's Child Figure Drawings, 17 which consisted of seven male and seven female figures ranging from very thin to obese. Thinnest body figure was represented by a score of 1, largest body figure represented by a score of 7, and average body figure represented by a score of 4. Questions were asked to indicate the body figure chosen for current body size and ideal body size. The difference was used to measure body image dissatisfaction, with a score ranging from −6 to +6. This instrument was found to have good test-retest reliability in the current study (self-body figure, r = 0.71, ideal self-body figure, r = 0.59).
Disordered Eating
Disordered eating of the children was assessed using the Children's Eating Attitude Test (ChEAT), 18 which consisted of 26 self-reported items. The responses were rated on a 6-point Likert scale of always (3), very often (2), often (1), sometimes (0), rarely (0), and never (0). Scoring for item 26 is in reverse manner. The total scores range from 0 to 78. This questionnaire was found to have good internal reliability in the current study (Cronbach's alpha, α = 0.71).
Depression
The symptoms of depression in children were assessed using the Children's Depression Inventory, 19 which consisted of 27 items with three choices of answers rated with scores of 0, 1, or 2 corresponding to the severity of the depressive symptoms. Children were asked to select one answer that best represents how they feel in the past 2 weeks. Scoring for items 2, 5, 7, 8, 10, 11, 13, 15, 16, 18, 21, 24, and 25 was in reverse order. The total score ranges from 0 to 54. The higher the scores, the greater the severity of the symptoms of depression. This questionnaire was found to have good internal consistency (Cronbach's alpha, α = 0.75).
Dietary Intake and Physical Activity
The dietary intake of the participants was assessed using a 2 day (1 week day and 1 weekend day) 24-hour dietary recall for the calculation of energy intake (EI). Physical activity of the participants was assessed using a 2-day physical activity recall on various activities performed for every 15 minutes which was assigned with a metabolic equivalent value for each activity for the calculation of total energy expenditure (TDEE). The mean of EI and TDEE was calculated.
Cognitive Function
The cognitive function of the children was assessed using the Wechsler's Intelligence Scale for Children-Fourth Edition (WISC-IV) which is a cognitive function test for children aged 6 to 16 years. To reduce fatigue and burden of the respondents, only similarities, digit span, block design, and coding were used in this study. For each of the subtests, the raw scores were converted into scaled scores that were adjusted for age. 20 A composite score was derived from the four scaled scores and was converted into cognitive function scores using a conversion table provided by the test provider for WISC-IV short forms. 20 The internal consistency of the cognitive function scores in the current study was found to be adequate (α = 0.71). All the subtests used were translated into Malay language and back-translated by two qualified psychologists who were proficient in both English and Malay language. The face validity of the items was then examined by a qualified and registered clinical psychologist. Before the administration of the test, the researcher was trained by a qualified clinical psychologist. The data collection was then conducted in a quiet room using uniformed procedures.
Data Analysis
Data were analyzed using IBM SPSS Statistics software (Version 22.0). To determine the mediators in the relationship between overweight/obesity and cognitive function, bootstrapping (resampling) approach was used as it is suitable for testing multiple mediators simultaneously by estimating the total and specific indirect effects. 21 A significant total indirect effect suggests that weight status (X) (normal weight = 0; overweight/obese = 1) is associated with cognitive function (Y) through the multiple mediators (M). Specific indirect effects refer to the extent to which the mediator contributed to the relationship between X and Y.
The analytical diagram in Figure 1 shows the coefficients estimated where “a” coefficients represent the relationship between weight status and the mediators, and the “b” coefficients represent the relationship between mediators and cognitive function partialling out weight status. The “c” represents the total effect of weight status on cognitive function. The “c′” represents the direct effect of weight status on cognitive function. The specific indirect effects are represented by a1b1 (body image dissatisfaction), a2b2 (disordered eating), a3b3 (depression), a4b4 (systolic blood pressure), a5b5 (DBP), a6b6 (TG), a7b7 (HDL-C), a8b8 (HOMA-IR), and a9b9 (hs-CRP). The total indirect effect is the sum of all the specific indirect effects. As weight status (X) was coded to differ by one unit between the two groups, the regression coefficient of the total indirect effect can be interpreted as the difference in cognitive function score between the normal weight and overweight/obese children.
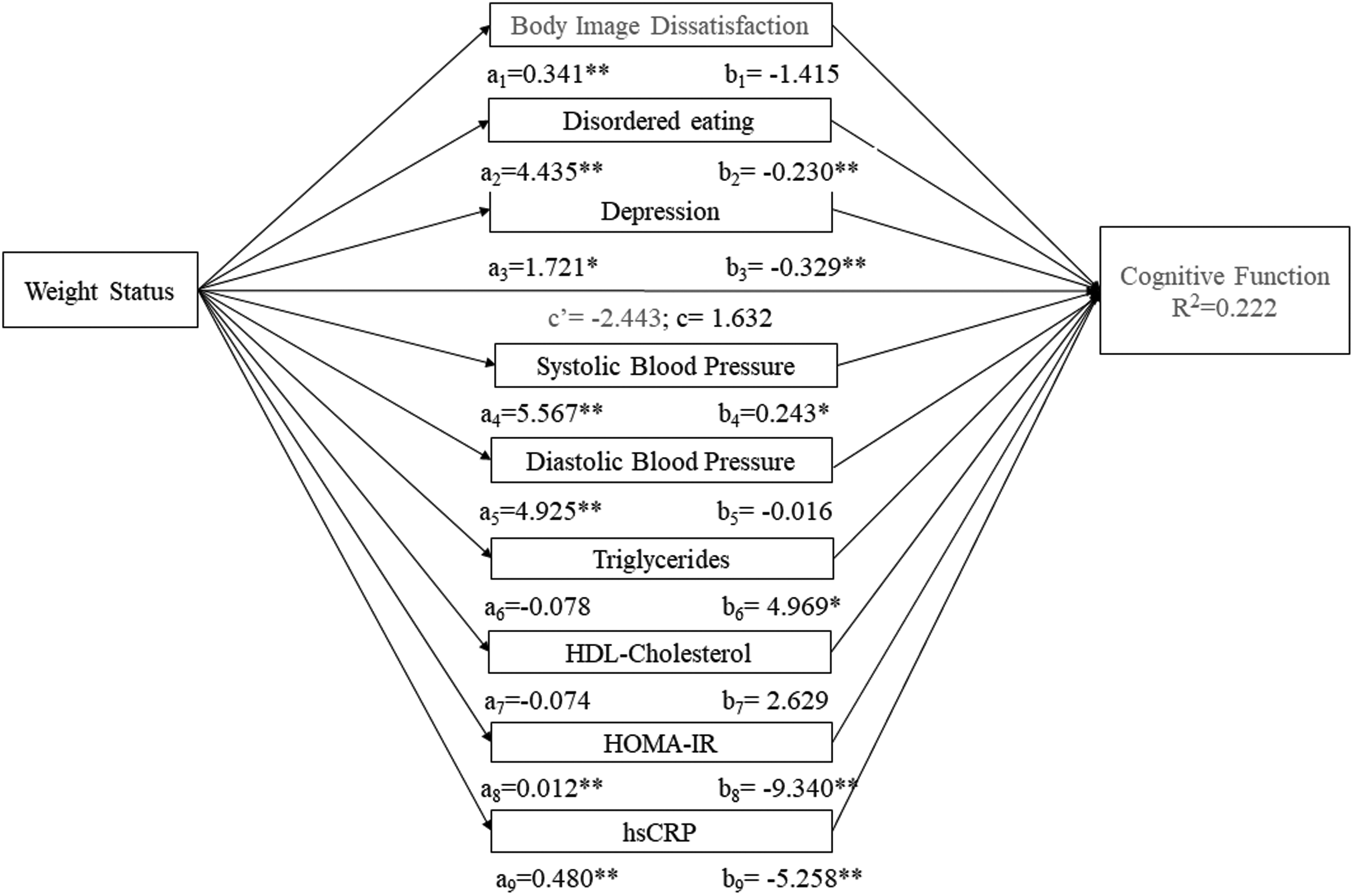
Direct effects of weight status to mediators and to cognitive function (*p < 0.05; **p < 0.01).
Current analysis was based on 5000 bootstrap samples, and 95% bias-corrected bootstrapped confidence interval (95% CI) was used to evaluate the significance and the magnitude of indirect effects. If zero does not occur between the lower level and upper-level confidence interval, the indirect effect for this mediator is deemed to be significant.
Intercorrelations of all mediators were tested before analysis. All mediators were found to be correlated with BMI and cognitive function except for EI and TDEE. As EI and TDEE are important factors associated with weight status and cognitive function, 1 these factors were included into the model as covariates instead. Fasting blood glucose and fasting blood insulin were removed from the analysis due to multicollinearity with HOMA-IR. Multicollinearity was determined with Tolerance less than 0.1 and variance inflation factor more than 10 (Pallant, 2005). When multivariate normality was tested, hs-CRP was not normally distributed; hence, logarithm transformation was conducted for this parameter.
Results
Figure 1 (see also Supplementary Table 1) presents the total and direct effects of weight status to mediators and cognitive function. The results showed that being overweight/obese had a direct positive effect on body image dissatisfaction, disordered eating, depression, systolic blood pressure, DBP, HOMA-IR, and hs-CRP. In the test of the direct effects of the mediators on cognitive function, disordered eating, depression, systolic blood pressure, TG, HOMA-IR, and hs-CRP significantly predicted cognitive function. The model explained 22.2% of the variance in cognitive function.
Indirect Effects of Weight Status to Cognitive Function through Mediators
Indicates significant difference.
CI, confidence interval; HDL-C, high-density lipoprotein cholesterol; HOMA-IR, homeostasis model assessment-estimated insulin resistance; hs-CRP, high-sensitivity C-reactive protein.
The examination of the total and specific indirect effects of weight status on cognitive function revealed interesting findings (Table 1). The total indirect effect was significant (95% CI [−6.343 to −1.886]), and the relationship was found to be negative (β = −4.075) indicating that overweight/obese children were on average 4.075 units lower in cognitive function scores compared to their normal weight counterparts. When specific indirect effects were examined, it was revealed that body image dissatisfaction (β = −0.482; 95% CI [−1.374 to −0.041]), disordered eating (β = −1.021; 95% CI [−2.081 to −0.329]), depression (β = −0.565; 95% CI [−1.443 to −0.071]), systolic blood pressure (β = 1.355; 95% CI [0.298 to 2.864]), TG (β = 0.365; 95% CI [0.017 to 1.087]), HOMA-IR (β = −1.089; 95% CI [−2.121 to −0.425]), and hs-CRP (β = −2.521; 95% CI [−4.111 to −1.265]) mediated the relationship between weight status and cognitive performance.
When pairwise comparison was made between the significant specific indirect effects, hs-CRP (B = −0.079) and HOMA-IR (B = −0.060) had significantly higher standardized effects compared to disordered eating (B = −0.029), depression (B = −0.011), and body image dissatisfaction (B = −0.019). Systolic blood pressure (B = 0.073) and TG (B = 0.022) were not compared as the standardized effects were found to be positive.
Discussion
The findings of the present study conclude that a negative relationship exists between overweight/obesity with cognitive function, and this was consistent with past literature.1–3 These findings were alarming as the children examined in the present study were healthy and nonclinical samples, which increase the importance for efforts to curb and reduce childhood obesity and to identify the key mediators contributing to the relationship between overweight/obesity and cognitive function.
Findings in the present study confirm that the relationship was mediated by psychological factors such as body image dissatisfaction, disordered eating, and depression. In line with previous finding, being overweight/obese is associated with body image disturbance, 22 and such preoccupation with body image and shape was found to be accompanied with poorer cognitive performance.7,9 Similarly, being overweight/obese is associated with increased risk of disordered eating behaviors, 23 which was then found to be associated with poorer cognitive performance. 8 According to literature, preoccupying thoughts on body image might have used more mental resources required for other cognitive tasks thus leading to poorer cognitive performance. As disordered eating, such as dieting, is related to preoccupying thoughts on body image, the relationship between disordered eating and poorer cognitive performance might also be due to the same mechanism. 9 In addition, being overweight/obese is also associated with increased depressive symptoms, 24 which were then found to be associated with poorer cognitive performance. 25 It is possible that the relationship may be through structural alterations on the white and gray matter of the brain or due to functional reasons such as elevated negative cognitions related to depression, which may then engage cognitive resources that would otherwise be allocated to cognitive processes. 26
Besides, the present study confirms that the relationship was mediated by cardiovascular disease risk factors such as inflammation and insulin resistance. The literature suggests that inflammatory mediators such as hs-CRP may be an indicator of early development of diseases associated with cognitive performance. 27 Abnormal levels of adipose tissues are known to trigger the production of C-reactive protein in response to inflammation, which in turn was reported to be associated with poorer cognitive performance. Inflammation may directly or indirectly be related to cognitive decline through further metabolic complications. 28 Findings from the present study is consistent with past studies whereby being overweight/obese poses greater risk of insulin resistance,29,30 which in turn is associated with poorer cognitive performance. 31 It was proposed that the changes in cognitive performance might be due to endothelial dysfunction associated with insulin resistance and type 2 diabetes mellitus. During cognitive processes, glucose levels in the brain decrease hence requiring further transport of glucose for cognitive processes. As endothelial cells play an important role as the mediating membrane for the transport of glucose through the blood–brain barrier, endothelial dysfunction associated with insulin resistance may lead to inadequate fuel substrate in the brain during cognitive processes. 10
A positive indirect relationship was found between overweight/obesity and cognitive function through systolic blood pressure and TG. Such a finding contradicts with past research where hypertension and elevated TG were found to be associated with poorer cognitive performance. 32 When further examined, the mean values of systolic blood pressure and TG were within the normal range. Hence, a possible reason to the positive relationship found in this study may be that the systolic blood pressure and triglyceride levels of these children did not reach a level where a negative association could be detected, as most of the children were without hypertension or elevated TG.
There are several limitations in the present study that need to be taken into consideration. First, the cross-sectional nature of the study is not able to demonstrate causal inferences between the variables despite the mediational analysis approach being taken in the analysis, as the data were collected at only one point in time. Therefore, a cohort study is needed to further confirm the findings of the model over a period of time and to understand the direction of the relationship. There is also a possibility that lower cognitive performance might have influenced weight status of the children leading to overweight/obesity as discussed in past literature. 2 Second, the respondents for this study were recruited from only one geographic area in Malaysia; hence, the results may not be generalizable to all children in the country. A larger and more diverse sample is needed from other geographical locations to confirm the findings. Third, majority of the measures except for anthropometric measurements and biochemical parameters were self-reported. Hence, there may be a response bias such as socially desirable answers or inaccuracy in recall during the assessment.
Although this study examined the mediators of the overweight/obesity and cognitive function relationship, it should not be considered as comprehensive as the mediation model was only able to explain 22.2% of the variances in cognitive function. Other possible mediators were not examined in the present study such as sleep habits or hydration status, which are known to be associated with both overweight/obesity and cognitive function. Examining these additional mediators could have helped to improve the variance explained in the cognitive function of the children. Other factors such as pubertal growth and iron status are other important confounders to be considered in the overweight/obesity and cognitive function relationship in children. Hence, further studies are needed to confirm these findings.
Conclusion
In conclusion, this study highlights the importance of psychological and cardiovascular disease risk factors as mediators of the relationships between overweight/obesity and cognitive function in children. Future childhood obesity interventions should not only target the reduction of weight but also should target to reduce the cardiovascular disease risk factors and improve the psychological health and well-being for the benefit of the cognitive development in overweight/obese children. Planning a multicomponent intervention that covers numerous plausible mechanisms is cost effective and benefits both obesity and cognitive development in children at the same time.
Footnotes
Acknowledgments
This work was supported by the UCSI University Research Grant Scheme (RGS) (Proj-In-FAS-016). The authors thank all the children involved for their participation and cooperation and their parents for permission and support in this study. The authors are also grateful to the school principals, teachers, administrators, and the Ministry of Education for their cooperation and assistance.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.