
Abstract
Background:
Several family-based efficacious pediatric weight management interventions (PWMIs) have been developed to reduce child weight status. These programs are typically based in larger cities delivered by an interdisciplinary team in a hospital or medical center. The degree to which these efficacious PWMIs have been translated to, and are feasible in, rural or micropolitan areas is unclear. This study protocol describes a pilot Type III hybrid effectiveness–implementation (T3HEI) trial testing a multilevel strategy that focuses on the adoption, implementation, and sustainability of a PWMI online training program and resource package designed for implementation in micropolitan and rural areas.
Methods:
The trial design employed the
Conclusions:
Our pilot T3HEI study has the potential to inform how best to move and sustain evidence-based PWMIs into practice. The findings will inform larger scale dissemination, implementation, and sustainability efforts in medically underserved areas across the country.
Trial registration:
This protocol is registered with clinicaltrials.gov (NCT04719442).
Introduction
The majority of efficacious family-based pediatric weight management interventions (PWMIs) have been based in large urban areas delivered through an interdisciplinary team in a hospital or medical center.1–8 Furthermore, the most recent U.S. Preventative Services Task Force recommendations for childhood obesity treatment do not address medically underserved audiences or settings where all members of an interdisciplinary team may not exist. 9 This is an important issue when considering that in rural areas the prevalence of obesity is higher,10,11 socioeconomic status is lower, access to preventive care (such as PWMIs) is limited in rural areas, 12 and 20% of the nation's populations reside in rural areas.
A related issue is the potential mismatch between the resources and available expertise used to deliver research- and hospital-based PWMIs in urban areas, when compared with micropolitan and surrounding rural areas (referred to as micropolitan areas throughout). 12 Specifically, the adoption, implementation, and sustainability of PWMIs may be limited in micropolitan areas unless adaptations are made to leverage multiple systems within a community that interact with families and children. 13
Systems-based approaches provide a model to integrate strategies that could improve the likelihood of evidence-based PWMIs to be adapted, adopted, implemented, and sustained in micropolitan areas.14–19 For example, a fund and contract dissemination strategy that includes a call for community proposals, application review, and contractual agreements for implementation can include requirements for systems-level partnerships and engaging vertical systems (e.g., decision makers and doers) in the implementation process. This also allows for the identification of community organizations with resources to implement a PWMI. 20 Similarly, a learning collaborative implementation strategy can be used to foster implementation fidelity, quality, and sustainability within and across systems that partner for PWMI delivery.21–24 Rooted in quality improvement processes, learning collaboratives provide structured training activities in a shared learning environment to close the gap between what is possible and what is practiced in clinical or community organizations.22–26
In response to the lack of movement of effective PWMIs into regular practice, the Childhood Obesity Research Demonstration Project (CORD) 3.027 called for dissemination and implementation (D&I) research to support the translation of “these programs into user-friendly packaged materials and messages that health care, community, or public health organizations can use in real-world settings.” 27 This article describes the Nebraska CORD 3.0 project that is a pilot Type III hybrid effectiveness–implementation (T3HEI) trial to test the utility of a systems-based approach with embedded D&I strategies.
Methods
This T3HEI trial was designed with a primary goal to address adoption, implementation, and setting-level maintenance (referred to as sustainability throughout) of the Building Healthy Families Online Training Resources and Program package (BHF Resources). 28 Secondary outcomes include program reach and child- and caregiver-level weight at 6 and 12 months postinitiation of the BHF program. The aim of the first study was developed to test the hypothesis that a fund and contract dissemination strategy that promoted local network weaving (i.e., systems-based multisectoral partnerships for recruitment and implementation) could identify four to eight communities where there was a demand and capacity for BHF adoption and implementation.28,29 The aim of the second study was designed to test the hypothesis that a learning collaborative implementation strategy combined with the BHF Resources would improve program adoption, implementation fidelity, and sustainability for a 2-year period—when compared with community access to the BHF Resources only. The aim of the third study was to determine the reach, effectiveness, and maintenance of BHF in participating children and families.
Guiding Frameworks and Processes
The
Study Participants
The systems-based and participatory approach to this pilot trial will yield three distinct groups of study participants reflecting the different levels of engagement and intervention.
BHF-CAB and payer subcommittee members
We will recruit up to 15 participants for the BHF-CAB including members of the original BHF development and implementation team, state-wide leaders from public health, school, health care, and other community organizations (e.g., parks and recreation, rural economic development) to support the D&I of BHF. In the last year of the study, a payer subcommittee led by a health economist and implementation scientist will be formed to engage in discussions around costs to implement BHF, potential reimbursement models and mechanisms, and sustainability of the newly adopted BHF program. The payer subcommittee will include a mix of BHF-CAB members and newly recruited participants who have expertise specific to task of the payer subcommittee.
BHF community implementation teams
The recruited communities will create implementation teams that will include both decision makers and BHF program implementors from community-based organizations that will support or deliver BHF. BHF Community Implementation Team (CIT) members will participate in the research trial and provide data including surveys and qualitative feedback on various aspects of the BHF Resources.
BHF program participants
Children and caregiver(s) that enroll in the BHF program across all recruited communities will provide data to determine the reach, effectiveness, and maintenance of effects of BHF when implemented in each community setting. All data will be gathered pragmatically based on information needed by CITs to successfully monitor program implementation and effectiveness.
BHF Resources
The backward-design approach and translation of the BHF Resources into the digital training and program materials platform have been described in detail in Heelan et al. 28 In brief, the BHF Resource was developed based on the successful adaptation of the Epstein Traffic Light Diet PWMI that has been delivered in micropolitan areas in Nebraska.37–39 The BHF Resource includes content focused on training CITs for program delivery, program materials, and a data portal with a reporting system to track participant success across the 12-month program—all necessary for a community to adopt and implement BHF. 28
Measures, Procedures, and Analysis Plan by Study Aim
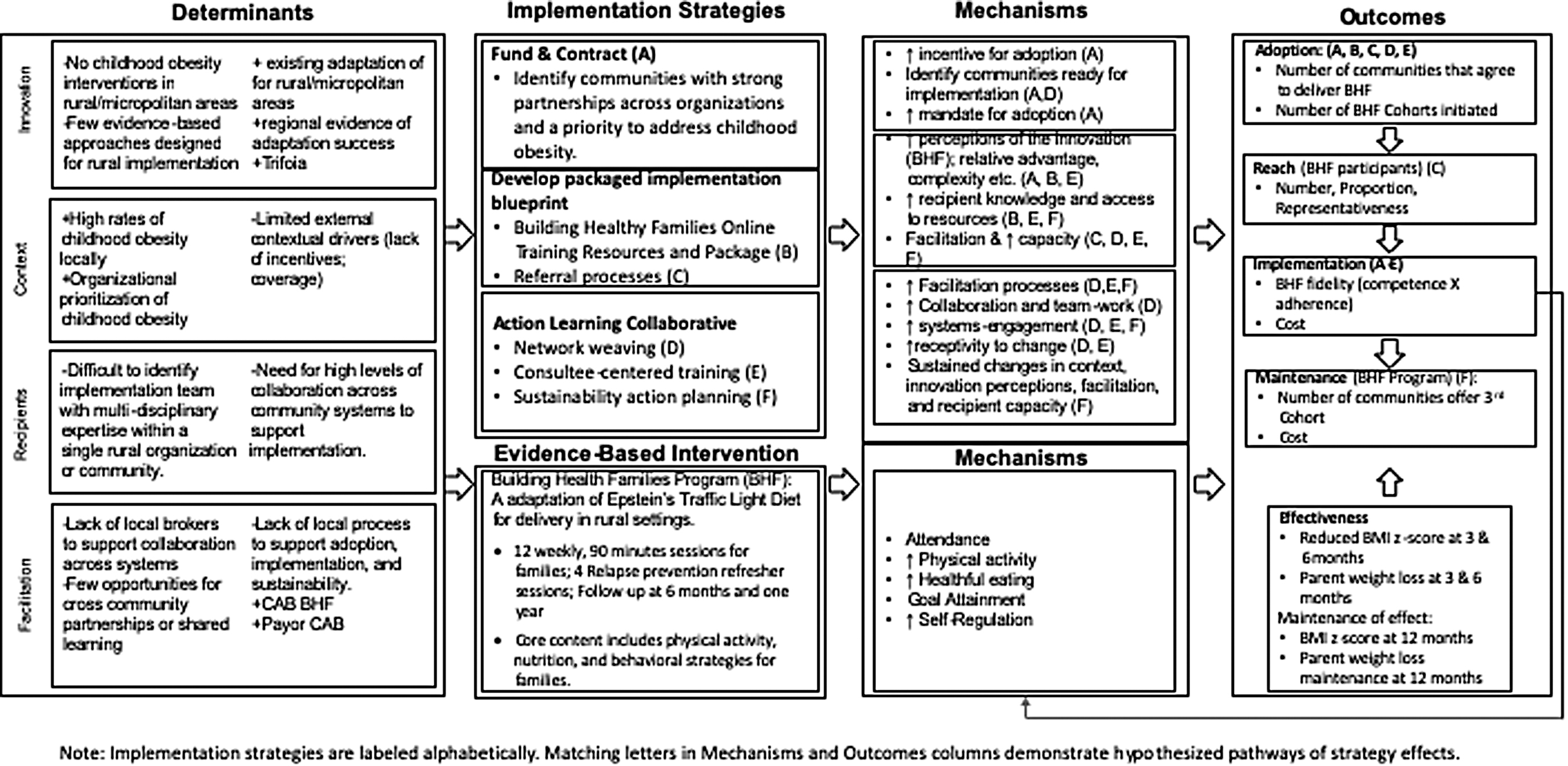
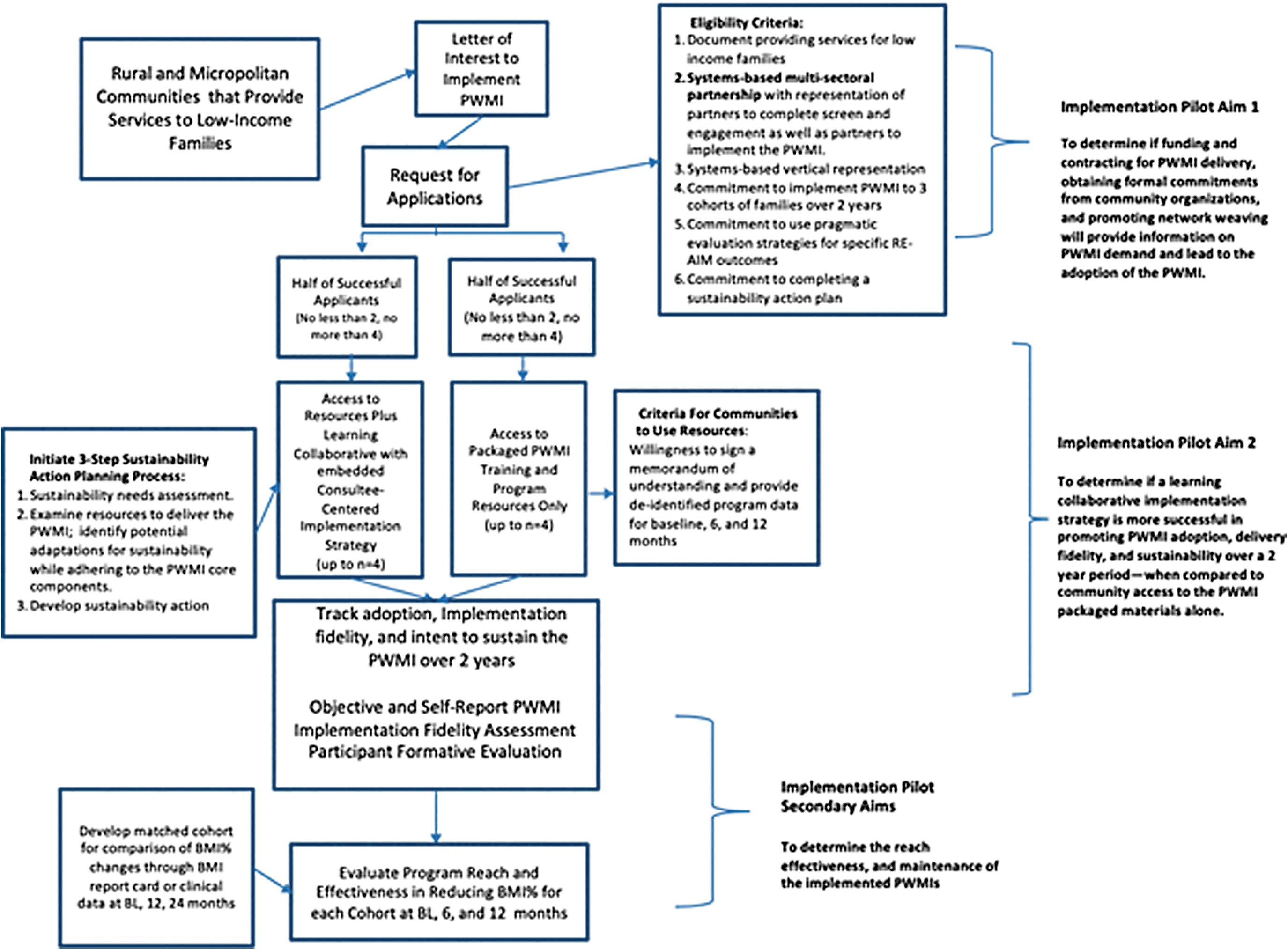
The following section outlines additional details on the measures, procedures, and analysis for each study aim. Figure 2 shows a schematic overview of the HEI pilot trial. Table 1 specifies the construct from either PARIHS or RE-AIM framework, the intended measure and data source, and a description of the outcomes for the trial. This study was approved by the University of Nebraska Kearney Institutional Review Board.
Type III Hybrid Effectiveness–Implementation Outcomes Are Guided by Promoting Action on Research Implementation in Health Services (PARIHS) and
BHF, Building Healthy Families; ORCA, Organizational Readiness to Change Assessment.
Specific Aim 1
To achieve Aim 1, the scientific team in collaboration with the BHF-CAB members will write and enact the request for applications (RFA). A call for letters of intent (LOI) will include a description of the packaged BHF, the need for communities interested in receiving training to implement BHF, and community rating of PARIHS constructs (e.g., evidence, context, and facilitation). This strategy is intended to target community readiness for BHF implementation and promote network weaving necessary for CIT program delivery. Communities that complete and submit an LOI will be invited to complete a full application. The BHF-CAB will collectively review all full applications and develop a rank order of communities with the possibility of selecting four to eight communities to participate in the trial and be assigned to the package-only (BHF-PO) or learning collaborative (BHF-LC) condition. 29
The scientific team and BHF-CAB members will disseminate the RFA broadly through their organizations and networks to ensure statewide reach and penetration into multiple communities and a range of organizations within communities. Count, proportion, and self-reported community characteristics of responding communities will be tracked to assess potential adoption and representativeness. At least one decision maker and one staff member who would be responsible for screening, recruiting, or implementing BHF from each organization will complete a characteristics questionnaire, which includes a modified ORCA, 34 when submitting the LOI. The BHF-CAB will then review, rank, and select communities for participation in the trial. 29
Hypothesis
Formal implementation commitments and network weaving will reduce the number of community responses, and higher community perceptions of the BHF evidence, local context, and facilitation (measured by the ORCA) will be related to adoption. Use of the BHF-CAB will increase the reach and identification of a broad cross section of communities interested in BHF.
Data Analysis
The baseline context, evidence, and facilitation domain scores as well as the total score from the ORCA 34 will be compared between organizations that opt to submit a full application versus those that do not submit a full application for participation in the study. The domain and total scores for the ORCA will be calculated by averaging the responses to sets of 5-point Likert responses. Given the pilot nature of this trial, analysis will move forward under the assumption that the ORCA is performing as designed and a linear mixed model will be utilized to analyze for potential differences between organizations that do and those that do not submit a full application.
Specific Aim 2
In Aim 2, a learning collaborative (BHF-LC) implementation strategy will be tested by assigning communities to one of two study conditions—the learning collaborative (BHF-LC) or package only (BHF-PO). The scientific team will create learning session topics that align with the timing of BHF program activities (e.g., participant recruitment and session implementation). Consultee-based training approaches will be embedded within learning sessions and action periods of the BHF-LC. 40 Learning collaborative activities will include instruction, review of previous implementations of BHF, self-reflection on implementation processes, goal setting and feedback, and collective problem solving to improve participant screening and engagement, implementation fidelity, and sustainability.
Two to four communities will be assigned to the BHF-LC and two to four communities, matched on proposal quality, will be assigned to BHF-PO. Training, knowledge, confidence, and engagement data for CITs in both conditions will be captured in the BHF Resources learning management system and the data portal. During program delivery, observed and facilitator self-reported fidelity assessments will be completed for each session across all communities. Process outcomes from learning sessions and action periods, including skills training, goal setting, and audit/feedback, will be tracked for BHF-LC sites. The ongoing training will be facilitated by the scientific team in collaboration with the BHF-CAB members. The sustainability action planning will be initiated after the completion of the first implementation of BHF by the BHF-LC communities and will be supported by the payer subcommittee and the BHF-CAB.
Adoption will be measured based on the number of cohorts initiated by CITs in the BHF-PO or BHF-LC conditions. PARIHS constructs will be compared between community partnerships in the BHF-LC with those that are in the BHF-PO condition. Perceptions of the innovation (i.e., the BHF Resources) will be assessed using an adaptation of a validated tool 41 through survey from each member of the implementation teams that engages with the online resource. Each member of the CITs will complete ORCA assessments at baseline, 2 weeks after initiating cohort 1 in their community, end of cohort 1, and end of cohort 2 for their community. Qualitative interviews will be conducted at the end of cohort 1 and end of cohort 2 for each community to allow for ongoing qualitative information on the evidence, context, and facilitation factors that may influence reach, implementation fidelity, and intent to sustain BHF.
Hypotheses
BHF-LC communities will be more likely to deliver BHF multiple times, demonstrate higher implementation fidelity, and have higher intentions to sustain the BHF when compared with BHF-PO communities. In addition, CITs in the BHF-LC will increase perceptions related to organizational context and facilitation potential for a local BHF program compared with the BHF-PO communities.
Data Analysis
Implementation fidelity will be analyzed using descriptive statistics and reported as proportion of intervention delivered as intended for the referral strategies and BHF implementation. A linear mixed effects model with the effect of time, group, and the time by group interaction as well as the appropriate nesting and repeated random effects will be utilized to capture ORCA changes between groups and over time. If the time by group interaction is not statistically detectable (i.e., if p > 0.05), it will be dropped from the model.
Specific Aim 3
Two dissemination strategies are proposed to increase program reach. The first focuses on integrating program information with school BMI report cards. In this approach, children with a BMI percentile ranking that is at or exceeding the 95th percentile will receive BHF program information. The second focuses on partnerships with local pediatric or family medicine practices. This strategy includes either electronic health record review or point-of-care referrals to BHF for children at or exceeding the 95th percentile for BMI. We will monitor program effectiveness and maintenance using the data portal embedded in the BHF Resources. 28 The data portal provides CIT with a central location to manage data collection related to communities, cohorts, CIT facilitators, participating families, and outcomes data.
Participant reach and representativeness data will be tracked through the screening and referral process used by each CIT (i.e., school or clinical strategy already described). Each CIT will report a denominator of potentially eligible participants based on available school or clinic data. The numerator will be collected using enrollment data that are embedded in the BHF Resources. Participant demographic information, including race, ethnicity, and socioeconomic status, will be collected by the CITs and entered into the BHF Resources data portal. The number, proportion, and representativeness (based on economic status) of children enrolled in BHF will be tracked across all sites.
Effectiveness and maintenance data will be tracked using height and weight information for all caregivers and children assessed at baseline, 12 weeks, 6 months, and 12 months. BHF CIT will use a calibrated digital scale and mounted digital stadiometer. Height, weight, gender, and age will be used to compute BMI and extended BMI z-score using standard algorithms. 42 BHF program outcomes, including weekly attendance, weekly weight, and change in weight, and behavioral outcomes (i.e., goal attainment and self-regulation), are tracked by BHF CIT and entered into the data portal. Change in weight, BMI or extended BMI z-scores, attendance, and behavioral outcomes will be computed weekly for use by CITs and research outcomes will be based on values at baseline, 12 weeks, 6 months, and 12 months. Matched cohort data will be compiled using annual school BMI assessment and report cards from local schools. One-to-one matches, based on age, gender, and BMI percentile ranking, will be used to reduce potential biases.
Hypotheses
Participants in BHF will reduce extended BMI z-score at 12 weeks and 6 months, and will maintain reductions at 12 months. BHF participants will also have a significantly larger extended BMI z-score reduction when compared with the matched cohort at 12 months. There will be no difference in program reach between communities.
Data Analysis
The number, proportion, and representativeness of participants enrolled in the study will be considered based on the referral source—schools and/or clinic. Number and proportion of families by referral source will be crudely assessed through chi-square test and modeling the number and proportion enrolled per month per referral source per cohort through generalized estimating equation (GEE). GEEs allow for the inclusion of a working correlation structure to account for the “repeated” nature of the outcome. 43 Representativeness of the participants based on referral source will be assessed by calculating point estimates and associated 95% confidence intervals for basic demographics, health, and behavioral information.
Discussion
The overarching goal of this pilot T3HEI study is to fill a gap in our understanding of how best to translate effective PWMI into micropolitan areas. To date, most of these studies have been conducted in large urban medical centers with little understanding of the factors that are relevant to translate to rural and micropolitan communities. There is not a lot of information about what types of organizations and professionals may serve as substitutes in underserved areas and what types of training on the evidence-based intervention are needed. BHF was developed to address this problem and has shown to be effective in reducing child and caregiver weight.
In this article, we outlined a T3HEI pilot trial of a systems-based approach to disseminating and implementing the BHF Resources.. This pilot trial will test novel implementation strategies (i.e., learning collaborative) for their ability to increase implementation quality and sustainability. Learning collaboratives have seldom been tested against a control condition; our design will allow us to examine the degree to which a learning collaborative adds benefit to implementation and sustainability of BHF and to what extent that benefits the effectiveness of the program at achieving intended outcomes. This pilot also includes several participatory systems-based research components to ensure local stakeholder engagement and that the packaged and testing of the BHF are acceptable, feasible, and likely to be adopted by micropolitan communities.
Potential challenges exist for the trial. As a pilot trial, we will target a smaller number of communities and cohorts, and potential attrition within and across sites of families enrolled in BHF will be carefully monitored. This will limit our ability to use inferential and predictive analyses. There is the potential the packaged training resource is not effective and implementation fidelity of key BHF components is low. To the extent possible, the research team will act to minimize these possibilities. However, as a HEI trial, information about barriers to implementation and factors associated with attrition are important outcomes. Identification of the relevant adoption and implementation factors, particularly in rural settings, is sorely lacking in family-based obesity treatment trials and our findings will contribute to what is known about uptake of evidence-based PWMI in micropolitan communities.
Footnotes
Disclaimer
This work is solely the responsibility of the authors and does not represent official views of the Centers for Disease Control and Prevention (CDC), Health and Human Services (HHS) or the US Government.
Funding Information
This study was supported by the Centers for Disease Control and Prevention (CDC) (Award No: 1U18DP006431-01-00).
Author Disclosure Statement
No competing financial interests exist.