
Abstract
Background:
Celiac disease (CD) is a multifactorial, immune-mediated enteropathic disorder that may occur at any age with heterogeneous clinical presentation. In the last years, unusual manifestations have become very frequent, and currently, it is not so uncommon to diagnose CD in subjects with overweight or obesity, especially in adults; however, little is known in the pediatric population. This systematic review aims to evaluate the literature regarding the association between CD and overweight/obesity in school-age children.
Methods:
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines were followed. An electronic database search of articles published in the last 20 years in English was carried out in Web of Sciences, PubMed, and Medline. The quality of the included studies was assessed by using the STrengthening the Reporting of OBservational studies in Epidemiology statement.
Results:
Of the 1396 articles identified, 9 articles, investigating overweight/obesity in children/adolescents affected by CD or screening CD in children/adolescents with overweight/obesity, met the inclusion criteria. Overall, the results showed that the prevalence of overweight or obesity in school-age children (6–17 years) affected by CD ranged between 3.5% and 20%, highlighting that the coexistence of CD with overweight/obesity in children is not uncommon as previously thought.
Conclusion:
Although CD has been historically correlated with being underweight due to malabsorption, it should be evaluated also in children with overweight and obesity, especially those who have a familiar predisposition to other autoimmune diseases and/or manifest unusual symptoms of CD.
Introduction
Celiac disease (CD) is a chronic and immune-mediated enteropathic disorder that primarily involves the small intestine of genetically predisposed individuals. 1 It is a multifactorial disease resulting from the interaction between genetic, immunological, and environmental factors, the latter including gluten found in wheat, rye, and barley, that triggers and maintains the small intestinal injury.2–4 The overall prevalence of CD is ∼1%, according to sex, age, and geographic location,4–6 even if it seems to be globally underdiagnosed. 7
For a long time, CD has been considered a pediatric disease, manifesting with diarrhea, malabsorption, and failure to thrive. 8 Currently, it is well known that CD may occur at any age with heterogeneous clinical presentation, which differs according to the age and may include usual symptoms, unusual symptoms, or sometimes no symptoms at all.1,4,9 Usual CD symptoms are mainly related to the injury of the primary target organ of the disease, the small intestine, and therefore comprise gastrointestinal manifestations, such as chronic diarrhea and abdominal distension.8,10,11 These symptoms may or may not be present at diagnosis and are more common in very young children (<2 years old).8,10,11
Unusual CD symptoms frequently affect older children, adolescents, and adults and include gastrointestinal manifestations, such as abdominal pain, constipation, and vomiting, but also extraintestinal symptoms, such as anemia (iron, vitamin B12, folic acid deficiency), fatigue, headache, recurrent aphthous stomatitis, osteopenia/osteoporosis, short stature, arthritis, miscarriage, infertility, and neurologic symptoms.7,8,12,13 In the last decades, the usual clinical presentation of CD has changed both in children and adults and extragastrointestinal symptoms have become more frequent than the intestinal ones 14 ; at the same time, atypical manifestations have increased more and more.8,15 Consequently, it is not unusual to diagnose CD in subjects with overweight or obesity, as several studies performed on adults have demonstrated the presence of overweight or obesity, according to their BMI.16–20
Similarly, other findings21,22 have shown the presence of overweight/obesity in children with a recent CD diagnosis; these results were recently confirmed by Nenna et al, 23 who found a range of 8.8%–20.8% of patients with overweight and up to 6% of patients with obesity at CD onset. Thus, although the relationship between CD onset and weight gain is not yet fully elucidated, over time, the prevalence of CD has increased, and it is now common to see patients with CD also diagnosed with overweight or obesity.23–30 This phenomenon is noteworthy because many cases risk not being accurately assessed. Therefore, professionals should be careful in considering the plethora of signs and symptoms associated with CD, without a priori ruling out the diagnosis of CD in children with overweight/obesity to perform early screening and prevent the organic complications of untreated CD.
To understand the scope of this association, the present research aimed at systematically reviewing the scientific literature of the last two decades with the purpose to investigate the coexistence between CD and overweight/obesity in the pediatric population.
Methods
The present systematic review has been registered in the PROSPERO International prospective register of systematic reviews (register no. CRD42020201775) and has been reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 31
Search Strategy
A systematic review of the literature was performed on July 30, 2020. The search was carried out in the content of MEDLINE, through PubMed and Web of Science; since the exponential increase of articles on CD in children from 2000, all the articles published in the last 20 years (from 2000 to 2020) were taken into consideration. A literature search was performed using structured search strings, taking into consideration the following combined search terms for the CD, the study population, and the weight status. Therefore, “Celiac” OR “Coeliac” combined to “Child*” OR “Infant*” OR “Paediatr*” OR “Pediatr*” OR “Adolesc*” combined to “Obes*” OR “Growth” OR “Overweight.” An example of the search strategy is reproduced in Supplementary Table S1.
Inclusion Criteria
We included studies (“clinical study,” “clinical trial,” “comparative study,” “randomized controlled trial,” “multicenter study,” “observational study,” “case-control study,” “cross-sectional study,” “cohort study”) in English language examining school-aged subjects (age range 6–17 years) with the diagnosis of overweight or obesity, according to the different BMI growth percentile curves classification [the CDC, Growth Charts, 32 the International Obesity Task Force,33,34 the World Health Organization (WHO), 35 the country-specific curves from Cacciari et al, 36 the BMI z score-based criteria from the CDC, 37 or WHO 38 ].
The diagnosis of CD was referred to (1) the European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) published in 1990, 39 where the diagnosis of CD is based on the presence of flat small intestinal mucosa with histological characteristics of hyperplastic villous atrophy while the patient is still eating gluten-containing foods, and the diagnosis is confirmed by full clinical remission, after gluten exclusion; (2) to the revisited ESPGHAN criteria published in 2012, 40 where serological tests have gained a pivotal role in diagnosis avoiding the collection of intestinal biopsy samples from children who meet the following criteria (i) having the characteristic symptoms of CD (particularly malabsorption); (ii) showing levels of Transglutaminase (TGA)-immunoglobulin A (IgA) greater than 10-fold, the upper limit of normal (confirmed with a positive result for endomysial antibodies (EMA)-IgA in a second serum sample), and (iii) having homozygosity or heterozygosity for Human Leukocyte Antigen (HLA)-DQ2 or -DQ8 to add strength to the diagnosis; (3) to the last version of the ESPGHAN criteria revised in 2020, 41 where some additional criteria have been included, such as (i) the combination of total IgA and TGA-IgA for a more accurate initial testing; (ii) the need for biopsy to decrease the risk of false-positive diagnosis for children with positive TGA-IgA but low titers (<10 times upper limit of normal); (iii) the no-biopsy approach for CD diagnosis in symptomatic or asymptomatic children with high TGA-IgA values (≥10 times the upper limit of normal) with appropriate tests and positive EMA-IgA in a second serum sample; and (iv) the not required HLA-DQ2 and DQ8 typing in patients with positive TGA-IgA, if they qualify for CD diagnosis with biopsies or have high serum TGA-IgA (≥10xULN) and EMA-IgA positivity (if anyone tests negative for HLA-DQ2 and DQ8, the risk of CD is very low, while a positive result does not confirm the diagnosis); (4) to the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) guidelines, 42 published in 2005, where the measurement of tissue transglutaminase (TTG)-IgA levels for the initial screening (total IgA when TTG-IgA is low, and TTG-IgG in individuals with known selective IgA deficiency and symptoms suggestive of CD) and the intestinal biopsy for CD diagnosis confirmation; when the diagnosis is uncertain additional strategies can be considered, including HLA type determination; (5) to the British Society of Paediatric Gastroenterology, Hepatology and Nutrition, 43 guidelines that extend the earlier NASPGHAN Celiac Guideline of 2005 and the original guideline from the Welsh Paediatric Gastroenterology MCN to incorporate the changed ESPGHAN 2012 diagnostic guidelines.
The age group of subjects ≥6 was chosen because the investigation of unusual symptoms associated with CD in school-aged patients is easier. In fact, in this age-range group, communication between the patient and doctor is clearer than in younger children, as they can describe their feelings and symptoms more accurately. Second, school-age children are more independent in their food choices, thus enjoying a wider range of foods.
Outcome
The main outcome of this systematic review was to evaluate the copresence between CD and overweight/obesity in school-aged subjects.
Exclusion Criteria
Narrative reviews, systematic reviews, meta-analyses, and case reports were excluded, as well as case series, descriptive studies, comments, and articles that did not correspond to the objective of this review or had no full-text accessible in English. Furthermore, studies involving children younger than 6 years or adults older than 17 years, or children/adolescents studied solely for CD or solely for overweight/obesity were excluded.
Data Collection and Extraction
Three coauthors (F.B., F.L., and G.P.) determined whether the studies met the criteria previously established by undertaking the initial duplicates and title screenings and abstract review independently. In brief, after applying the search filters, the studies were divided equally among the three coauthors for data extraction. A fourth coauthor (R.D.G.) randomly checked a sample of about 20% of the articles.
Before its inclusion in the article, each full-text article selected for retrieval was reviewed independently by the three coauthors (F.B., F.L., and G.P.), checking the eligibility. Any difference in the selection process was solved by discussion until they agreed. Whenever there was no full consensus, a fourth coauthor (R.D.G.) was consulted. The three coauthors (F.B., F.L., and G.P.) independently extracted relevant information from all the included studies, such as (1) author and publication year, (2) type of the study, (3) country, (4) sample size, (5) characteristics of participants (age and gender), (6) criteria utilized for CD diagnosis, (7) outcome assessment (BMI, percentile, or BMI z-score), (8) analysis method, and (9) findings. Whenever there was no full consensus, a fourth coauthor (R.D.G.) was consulted.
Data Synthesis
Data extracted from this systematic research are presented as a narrative summary of the findings. For the longitudinal studies considered for the present review, only baseline data were considered and presented.
Study Quality Assessment
Three coauthors (F.B., F.L., and G.P.) independently assessed the quality of each study that met the inclusion criteria; any differences were resolved by discussion with a fourth reviewer (R.D.G.). The criteria for quality appraisal were adopted from the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement. 44 The 22-item checklist (the STROBE statement) is reported in Table 2. A formal quality score for each study was completed on a 22-point scale by assigning a value of 0 (absent/inadequately described/unsure) or 1 (explicitly described and present) to each item, consisting of a 22-point scale. Studies that scored 0–11 were classified as low quality, and those with a score ≥12 were considered high quality. The STROBE checklist was used in conjunction with the article published by Vandenbroucke et al 45 that handed the use and the understanding of the STROBE checklist. 44
Results
Overview of the Studies
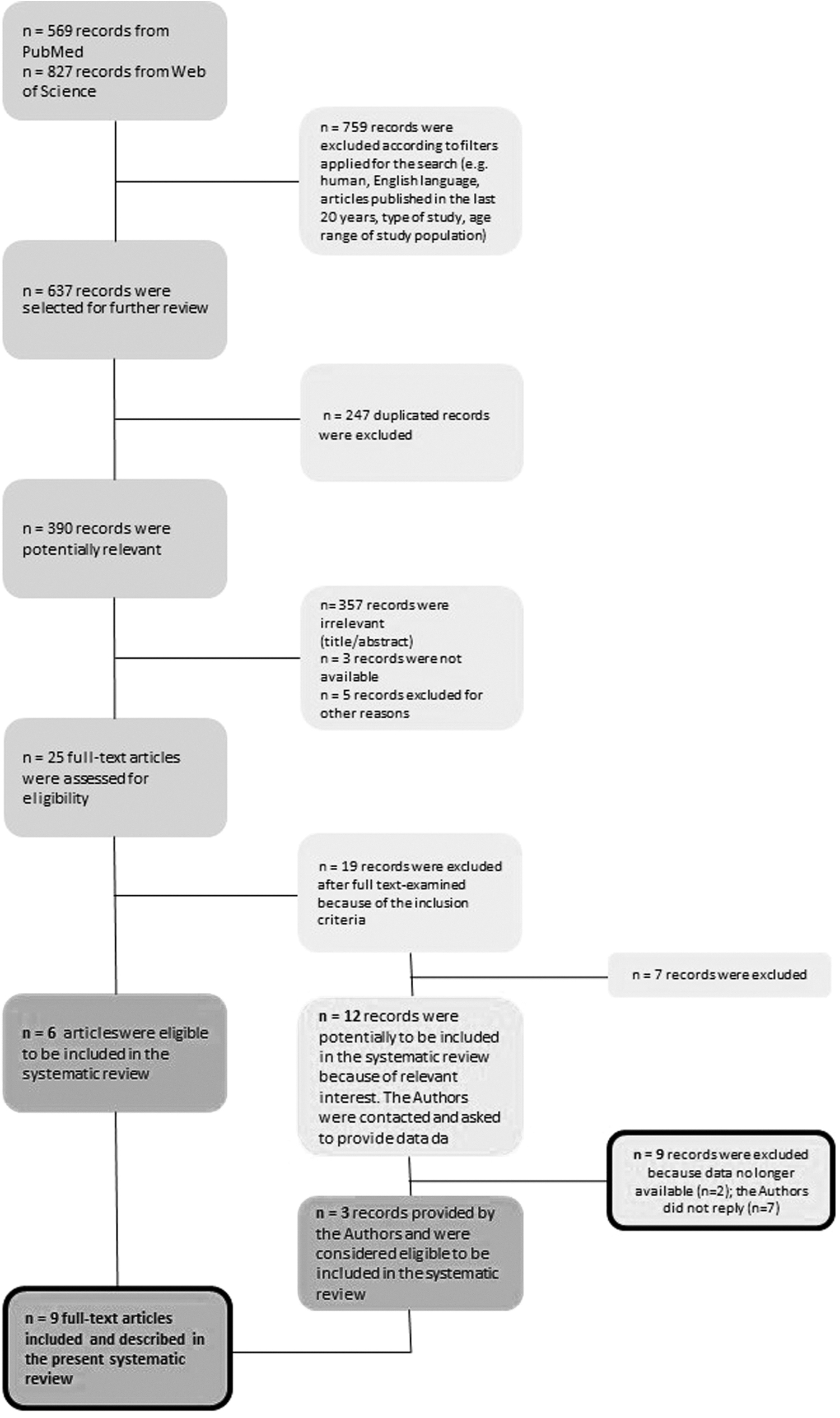
A flowchart summarizing the study selection procedure is presented in Figure 1. Electronic searches from PubMed and Web of Science returned 1396 records; 759 records were excluded based on the filters applied for the search. Duplicates (n = 247) were first removed. Then, 365 studies were excluded because the titles and abstracts were not relevant or because the studies were not available or for other reasons. Finally, 19 studies were further excluded after reading the full texts, since they did not meet the inclusion criteria; only 6 studies met all the inclusion criteria (green box in Fig. 1 and Table 1).25,29,30,46–48
Description of the Studies Selected According to the Inclusion and Exclusion Criteria and Included in the Systematic Review (Bold-Line Lower Left Box in Fig. 1)
Data are presented as percentages and the absolute number of children/adolescents presenting overweight or obesity. Furthermore, although this systematic revision aimed to investigate the coexistence between CD and overweight/obesity, the authors reported also the normal weight and underweight status data.
BSPGHAN, British Society of Paediatric Gastroenterology, Hepatology and Nutrition; CD, celiac disease; ESPGHAN, European Society for Paediatric Gastroenterology Hepatology and Nutrition; ETICS, Exploring the Iceberg of Celiacs in Sweden; F: females; GFD, gluten-free diet; IOTF, International Obesity Task Force; M: males; n.a.: not applicable; NASPGHAN, North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition; SD, standard deviation; WHO: World Health Organization.
It remains noteworthy that of the 19 excluded studies, 12 could only potentially be included in the systematic review (yellow box in Fig. 1),21–24,26–28,49–53 because they did not meet the age inclusion criterion, since the study population ranged from a few months of age to 18 years, without the possibility to analyze the specific age group of interest (school-aged subjects ranging 6–17 years) or because they did not report any information on the CD diagnostic criteria. For this reason, the authors of those studies21–24,26–28,49–53 were contacted to obtain the data sets and extrapolate the necessary information, following the inclusion/exclusion criteria applied in the present systematic review.
Among the authors contacted, only authors of three studies50,51,53 provided data (green box in Fig. 1), while for nine studies, data were no longer available (n = 2) or the authors did not reply (n = 7) (yellow box in Fig. 1). Hence, only nine studies25,29,30,46–48,50,51,53 were included and evaluated in the present systematic review (bold-line green box in Fig. 1 and Table 1). However, the other nine studies21–24,26–28,49,52 (bold-line yellow box in Fig. 1) are reported in Table 3 and summarized in a separate paragraph (“Characteristics of studies not included in the systematic review”) as they reported outcomes of relevant interest.
Quality Assessment
A value of 1 (V: explicitly described and present) or 0 (X: absent/inadequately described/unsure) was assigned to each item. For the 22-item checklist, studies that scored 0–11 were classified as low quality, and those with a score of 12 or more were considered high quality.
Description of Some Studies (n = 9) Excluded from the Systematic Review (Bold-Line Lower Right Box of Fig. 1), Nonetheless With Results of Relevant Interest
Data are presented as percentages and (the absolute number) of children/adolescents presenting overweight or obesity. Furthermore, although this systematic revision aimed to investigate the coexistence between CD and overweight/obesity, the authors reported also the normal weight and underweight status data.
Children with BMI below the age- and sex-specific cutoff points corresponding to the adult BMI value of 18.5 (grade I), 17 (grade II), and 16 (grade III).
Overview of the Study Quality
The assessment of the study quality of the eligible studies (bold-line green box in Fig. 1)25,29,30,46–48,50,51,53 of the present systematic review is reported in Table 2. Most of them29,30,46–48,50,51,53 were considered of high quality, as they scored 12 or more. Only Venkatasubramani et al 25 reported a score of 11.
Characteristics of Studies Included in the Systematic Review
The description of the nine studies included in this systematic review25,29,30,46–48,50,51,53 (Table 1 and bold-line green box in Fig. 1) is provided below. Different study populations were considered. Seven studies25,29,46,48,50,51,53 investigated the weight status (e.g., underweight, normal-weight, overweight, and obesity) in children/adolescents affected by CD. On the contrary, Calcaterra et al 30 explored the prevalence and clinical presentation of CD in children and adolescents with overweight and obesity, while Al-Hussaini et al 47 conducted a large mass-screening study, investigating the prevalence of CD in school-aged children, and then characterized the celiac iceberg. Interestingly, the CD could be exemplified as an iceberg in which clinically symptomatic patients are represented above sea level, while below the water surface, CD patients are asymptomatic. 54
As far as studies performed on populations with CD,25,29,30,46–48,50,51,53 five of them were cross-sectional studies25,30,46,47,51 and four29,48,50,53 included a healthy control group.
Briefly, Assa et al, 46 in a large cross-sectional and population-based study, investigated the association of CD with cardiovascular risk factors, including overweight and obesity, in 2,001,353 Jewish adolescents. The authors stratified the overweight and obesity prevalence according to gender, reporting overweight in 15.3% of males and 15.7% of females and obesity in 3.6% of males and 3.4% of females. Similarly, Van der Pals et al, 29 starting from the 12,632 twelve-year-old children included in the Exploring the Iceberg of Celiacs in Sweden (ETICS) study, 55 compared the weight, height, and BMI of 239 screening-detected CD children with those of 12,227 healthy peers (without CD). The prevalence of overweight/obesity was observed in 13.8% of subjects with CD and was significantly lower when compared with the prevalence of healthy peers. 29
Three studies25,48,51 were longitudinal and retrospective; two of them25,48 evaluated the presence of BMI >95th percentile and BMI >85th percentile in children/adolescents with CD, while the third one 51 used the BMI as a measure of weight status, according to the country-specific curves from Cacciari et al 36 ; in this case, only one study 48 included a healthy control group. Venkatatsubramani et al 25 estimated the prevalence of obesity at diagnosis in 143 subjects with CD and described the clinical characteristics of this group one year after initiating a gluten-free diet (GFD). Focusing on diagnosis time, obesity was observed only in 5.0% of the study population. 25 Similarly, Capriati et al 51 described the nutritional status of a cohort of children with CD at presentation and during follow-up on GFD by prospectively enrolling 445 biopsy-confirmed CD children (age range 2–17 years), diagnosed between 2009 and 2013 in two Italian centers (e.g., Rome and Bari).
In general, the authors 51 reported that, at diagnosis, overweight/obesity was present in 7.8% of children with CD; however, considering only children with CD between the ages of 6 and 17 (n = 249), according to the inclusion/exclusion criteria of this systematic review, 15% of children with CD were also affected by overweight/obesity. 51 Again, another recent longitudinal, retrospective, and case–control study 48 was conducted on 125 Italian children with CD and 125 healthy controls and 140 US children with CD and 140 healthy controls. The overall aim of the study was to explore the weight status between the two cohorts of children with CD and to better characterize the changes occurring in growth indices following long-term treatment with GFD, compared with healthy peers in a follow-up period of 3 years. 48
Within the aim of the present systematic review, the prevalence of overweight/obesity at diagnosis was observed in 6.0% of the Italian children with CD and 17.0% of the US ones. 48
Aurangzeb et al 50 conducted a cross-sectional evaluation of BMI, triceps skin fold, midarm circumference, body composition, and serum leptin levels of 25 children with newly diagnosed CD (age range 1.70 month–15.9 years), in comparison with 25 well-age and gender-matched controls. In general, at presentation, 20.8% of children with CD showed overweight, 50 however, considering only children aged ≥6 years (n = 14), the prevalence of overweight slightly increased to 21.4%. 50 Another cross-sectional study conducted by Tsiountsioura et al 53 assessed anthropometries, body composition, dietary intake, eating habits, and grip strength in 168 patients from outpatient gastroenterology clinics (Crohn's disease, n = 53; ulcerative colitis, n = 27; CD, n = 31; other gastrointestinal diseases, n = 57) and compared with contemporary healthy controls (n = 62) and the results of the recent UK, National Diet and Nutritional Survey. Interestingly, no children with CD were also affected by overweight or obesity. 53
Contrary to the studies described above, Calcaterra et al 30 investigated in a cross-sectional study, the prevalence and clinical presentation of CD in 200 children and adolescents with overweight (54% of subjects) and obesity (46% of subjects). The authors diagnosed CD in 4% of the children (six children with overweight and two children with obesity). 30
Last, Hal Al-Hussaini et al 47 performed, between January 2014 and June 2016, a cross-sectional, mass screening, TTG-IgA-based study on 7930 Saudi students to determine the prevalence of CD and characterize the celiac group among a Saudi pediatric population. The authors identified CD in 1.5% of children (103 cases of confirmed CD, 13 cases of celiac autoimmunity, and 2 cases of CD already diagnosed); among the 103 cases of confirmed CD, 20% of children were affected by overweight or obesity (7.8% and 11.7%, respectively). 47
Characteristics of Studies Not Included in the Systematic Review but Considered of Relevant Interest
This section presents the nine studies21–24,26–28,49,52 that were not included in this systematic review due to unmet age-related inclusion criteria, but with noteworthy results (bold-line yellow box in Fig. 1 and Table 3). Indeed, although the age population ranged in general between 6 months and 17 years,21,22,24,27,28,52 it was not possible to accurately identify the range of school-age children/adolescents. Furthermore, Alrae et al, 49 Reilly et al, 26 and Nenna et al 23 included also young adults (at or more than 18 years old).
Considering the study population, most of the studies21,22,24,26–28,49 investigated the weight status (e.g., underweight, normal-weight, overweight, and obesity) in subjects affected by CD; only Nenna et al 23 explored the presence of CD in 1527 subjects with overweight or obesity. As far as the studies assessing the weight status in subjects with CD are concerned, three studies21,49,52 were cross-sectional, while others22,24,26–28 were longitudinal retrospective researches, evaluating the effect of a GFD on several variables, including the BMI variations. Furthermore, only one 28 of them included a control group of healthy subjects (not affected by CD), which was well-matched for gender and age only in two studies.
Despite the nature of the studies and their objectives, for all of them21,22,24,26–28,49,52 it was possible to describe the prevalence of overweight or obesity in subjects affected by CD at diagnosis time (Table 3). Obesity was observed in four studies22,24,27,28 with a prevalence ranging between 0.7% 28 and 5.3% of subjects, 27 while overweight was reported in four studies22,24,27,28 and ranged between 8.6% 22 and 11.3%. 28 Contrarily to other colleagues, Alraee et al, 49 Gokce et al, 52 Reilly et al, 26 and Shahraki et al 21 reported a prevalence of increased BMIs in 4.2%, 5.8%, 14.8%, and 3.5% of subjects with CD, respectively, without discriminating between overweight and obesity.
In the study including a healthy control group, 28 a significant difference in the prevalence of overweight and obesity between patients and controls was observed, whereas the prevalence of increased BMIs (overweight plus obesity) was less frequent in subjects with CD when compared with the healthy controls (12% vs. 23.3%, p = 0.014).
Last, Nenna et al, 23 in a longitudinal and retrospective study on a population with overweight or obesity, reported a prevalence of CD in 11.1% of subjects at diagnosis time (Table 3).
Discussion
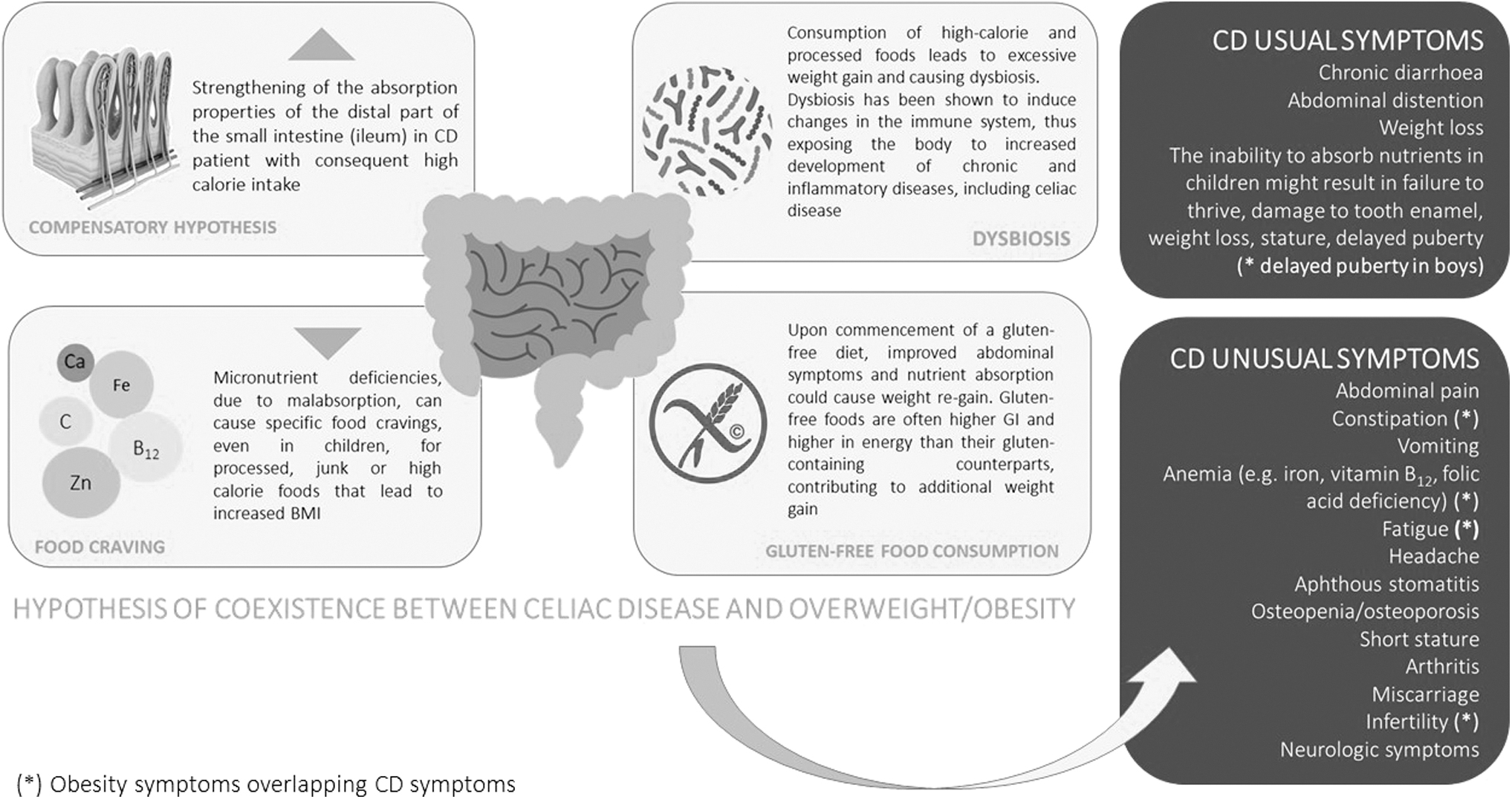
Although CD has been historically associated with underweight due to malabsorption,56,57 in the last decades, the clinical presentation of the disease has become more heterogeneous, including atypical manifestations and association with overweight and obesity being increasingly recognized (Fig. 2). For these reasons, in this work, scientific literature published in the last two decades on the coexistence between CD and overweight/obesity in the pediatric population (school-age children between 6 and 17 years) has been systematically reviewed. In particular, studies on overweight/obesity in children/adolescents affected by CD21,22,24,26–28,49–53 and studies screening CD in children/adolescents with overweight/obesity25,29–31,43–45,53 were evaluated to understand the extent of CD associated with overweight or obesity.
As shown in Table 2, most of the studies included were of good quality,29,30,46–48,50,51,53 reporting that the coexistence of CD with overweight or obesity in school-age children is not uncommon as previously thought. Eight studies25,29,46–48,50,51,53 evaluated the presence of overweight/obesity in subjects at the time of CD diagnosis, while one research 30 diagnosed CD in children with overweight and obesity. In detail, at the time of CD diagnosis, the prevalence of overweight ranged from 7.8% to 21.4%, while the prevalence of obesity was between 3% and 11.7%.
The data seem to follow the global trend of an increased rate of overweight/obesity in children, as already reported by the WHO in 2017. 58 In the last decades, indeed, the prevalence of overweight and obesity among children and adolescents aged 5–19 has globally increased at an alarming rate, 58 with 18% of girls and 19% of boys with overweight and 6% of girls and 8% of boys with obesity in 2016. 58 In addition, the wide range of overweight or obesity prevalence between countries could be due to the different geography of the studies (e.g., Israel, Saudi Arabia, Italy, Sweden, the United States), where different rates of overweight/obesity are the consequence of the cultural differences in the epidemiological background and public health prevention strategies to tackle childhood obesity. 59
The aforementioned considerations were also consistent for the other studies that were not considered in the present review because of the age-related inclusion criteria (bold-line yellow box in Fig. 1 and Table 3).21–24,26–28,49,52 Indeed, even if it was not possible to identify in these studies the range of school-age children, they strongly contributed to highlighting the importance of assessing the prevalence of overweight or obesity in subjects affected by CD at diagnosis time, as well as evaluating the frequency of CD with unusual symptoms in children with overweight or obesity, pointing up for both researchers and clinicians the necessity to take care of these patients from a new point of view.
In the present review, we particularly focused our attention on children and adolescents aged 6–17 (school-aged) for several reasons. First, this age group is the one in which most often unusual CD symptoms, frequently associated with overweight or obesity, are present 60 ; consequently, these patients escape the diagnosis of CD more easily. In general, CD screening is done only for weight and growth deficiency and not for other unusual symptoms or overweight/obesity that are initially not attributable to CD. 17 However, it should be considered that investigation of unusual symptoms associated with CD in school-aged patients is easier, as communication between the patients and clinician is clearer than in younger children, as they can describe their feelings and symptoms more accurately.
Second, school-age children are more autonomous in their food choices thus enjoying a wider range of foods. 61 Therefore, their dietary pattern may shift toward “unhealthy dietary habits,” also changing their weight status as they are more likely to snack and eat energy-dense and nutrient-poor foods and sugary drinks. 61 Besides, adolescents become more susceptible to their peers and social media influence acquiring overall unhealthy behaviors 62 that may expose them to a higher risk of excessive weight gain. 63
In the last few years, some hypotheses have been advanced to explain the coexistence between CD and overweight/obesity (Fig. 2).60,64,65 One of the most debated explanations is related to the ability of the small intestine, the target organ of CD, to adapt to the surrounding stressful environment. 66 Thus, the “compensatory hypothesis” 64 describes how the plasticity of the intestinal epithelium plays an important role in response to trauma, carrying out morphological and functional changes also in subjects with CD, where the distal part of the small intestine (ileum) strengthens its absorption properties as the duodenum and jejunum are atrophic.
However, the renewal properties and plasticity of the intestinal epithelium are both ineffective in very young children and become more reactive with increasing age. 64 As a result, an older child's gut is more likely to compensate for absorption problems, sometimes overcompensating. 64 High-calorie intake occurs when overcompensation occurs, and so, children with CD develop overweight or obesity. 64 However, the extent of intestinal damage defines the severity and type of clinical manifestations,12,67 also influencing the patient's BMI. 17
Another possible explanation for the coexistence between CD and overweight/obesity is that micronutrient deficiencies, due to malabsorption, can cause specific food cravings in adults, leading to increased BMI. 65 This probably also occurs in children and adolescents with CD, bearing in mind that the food craving is often for processed, junk, or high-calorie food 68 and that these patients usually consume lower amounts of fruits and vegetables, as recently shown by Calcaterra et al. 30 As previously mentioned, on one hand, school-age children and adolescents are more autonomous and influenced by their peers and social media marketing concerning food choices resulting in a shift toward unhealthy dietary patterns61,62; this can lead to the consumption of high-caloric and processed food that, together with reduced physical activity, leads to excessive weight gain. 63
On the other hand, an unbalanced diet rich in fat and sugar changes the composition of the gut microbiota, causing dysbiosis, which is defined as perturbations to the structure of complex commensal communities because an imbalance between increased pathogenic microbes and reduced beneficial bacteria occurs. 68 Dysbiosis has been shown to induce changes in the immune system exposing the organism to a higher development of chronic and inflammatory diseases, including CD. 69 Furthermore, the intestinal microbiota shaping seems to play a role in the pathophysiology of obesity development as it is related to energetic-humoral variations in the host.70,71 Therefore, based on these considerations, a hypothetical role of the microbiota in explaining the link between CD and obesity cannot be excluded.
Last, a factor that over time could exacerbate the coexistence of CD and overweight/obesity or increase the risk of developing overweight/obesity in the patient with CD is that once a diagnosis such as CD is given, parents and caregivers may try to overcompensate with gluten-free, but empty-calorie foods. Indeed, it has been reported 24 that replacing everyday staples with gluten-free foods could increase the risk of obesity, including also in children. Reasons for weight gain in patients with CD include better nutrient absorption and improvement in abdominal symptoms. 24 Besides, gluten-free foods are often higher in fat and calories than their gluten-containing counterparts, while being less high in fiber and whole grains. 24
The current work presents some limitations that should be taken into account, including (1) the few available studies evaluating the association between CD and overweight or obesity in children, especially considering the alarming increase of obesity prevalence worldwide; (2) the lack of data about family history of overweight/obesity in children affected by CD, with the exception of the Calcaterra et al 30 study, (3) the use of different criteria and different cutoffs for the classification of the weight status, (4) the use of different criteria for CD diagnosis, and (5) the different types of studies and their related outcomes, leading to the absence and availability of all parameters for all patients. Lastly, the updated PRISMA 2020 guidelines were not adopted.
However, despite the limitations listed above, the main strength of our work is that, to the best of our knowledge, this is the first review screening, systematically, the coexistence of CD and overweight/obesity in school-aged children and adolescents, highlighting that the simultaneous presence of CD and overweight/obesity is not so uncommon. This could be due to different reasons, such as (1) the presence of unusual CD symptoms in children and adolescents with overweight/obesity, (2) the excessive response of the “compensatory hypothesis” in individuals with CD, (3) the presence of food cravings, in response to inadequate dietary intake due to malabsorption, (4) the habitual shift toward unhealthy eating habits for teenagers, including eating too much, consuming high-energy and processed food, or eating a poorly planned selective diet, and (5) the intestinal dysbiosis that could impact negatively in the development of CD and overweight/obesity.
Therefore, in our opinion, it is crucial to take into consideration the presence of obesity in CD and vice versa. In this view, on one hand, further studies are strongly needed to (1) evaluate the frequency of CD with unusual symptoms in children with overweight or obesity, (2) assess the frequency of children with CD who develop obesity following CD diagnosis, (3) verify and deepen the etiopathogenetic mechanisms that may connect CD to overweight/obesity, and (4) unravel the possible role of gut microbiota in the association between CD and obesity.
On the other hand, clinicians should be careful in considering the plethora of signs and symptoms associated with CD, without ruling out the a priori CD diagnosis in children affected by overweight/obesity. Indeed, a delay in CD diagnosis leads to a delay not only in CD treatment but also in the treatment of obesity and its related consequences, including increasing intestinal injuries and the worsening of the disease, as well as the progression of nutritional deficiencies and the impairment of patient life quality. Thus, symptoms of patients with CD, even if they are affected by overweight/obesity, should be considered for a differential diagnosis. For their part, physicians should not be surprised in ascertaining overweight or obesity in a child with newly diagnosed CD.
Conclusion
In conclusion, CD should be considered in children with overweight and obesity, also considering the presence of a familiar predisposition to other autoimmune diseases that may represent a risk factor for the development of CD. Even though the relationship between obesity and CD is not well defined, patients with excessive weight who manifest unusual symptoms of CD should be screened for CD.
Footnotes
Acknowledgment
The authors are very grateful to Prof. Mauro Bozzola.
Authors' Contributions
R.D.G, F.B., F.L., and G.P.: protocol development, including search strategy, applied search to databases, screening and data extraction, data analysis and article write-up. F.G., V.C. and H.C.: conception of the idea, article checking, visualization and supervision. All authors have provided final approval of the article, as submitted.
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.