
Abstract
Introduction:
Children with obesity suffer excess dyspnea that contributes to sedentariness. Developing innovative strategies to increase exercise tolerance and participation in children with obesity is a high priority. Because inspiratory training (IT) has reduced dyspnea, we sought to assess IT in children with obesity.
Methods:
We conducted a 6-week randomized IT trial involving 8- to 17-year-olds with obesity. Participants were randomized 1:1 to either high [75% of maximal inspiratory pressure (MIP)] or low resistance control (15% of MIP) three times weekly. Assessments included adherence, patient satisfaction, and changes in inspiratory strength and endurance, dyspnea scores and total activity level.
Results:
Among 27 randomized, 24 (89%) completed the intervention. Total session adherence was 72% which did not differ between treatment groups. IT was safe, and more than 90% felt IT benefitted breathing and general health. IT led to a mean improvement (95% CI) in inspiratory strength measured by MIP of 10.0 cm H2O (−3.5, 23.6; paired t-test, p = 0.139) and inspiratory endurance of 8.9 (1.0, 16.8; paired t-test, p = 0.028); however, there was no significant difference between high- and low-treatment groups. IT led to significant reductions in dyspnea with daily activity (p < 0.001) and in prospectively reported dyspnea during exercise (p = 0.024). Among the high- versus low-treatment group, we noted a trend for reduced dyspnea with daily activity (p = 0.071) and increased daily steps (865 vs. −51, p = 0.079).
Discussion:
IT is safe and feasible for children with obesity and holds promise for reducing dyspnea and improving healthy activity in children with obesity. Breathe-Fit trial NCT05412134
Introduction
Nearly 40
One promising approach to reduce obesity-related dyspnea and boost physical activity is inspiratory muscle training (IT). Pulmonary rehabilitation (in its various forms, including IT) is a treatment cornerstone in adult medicine but is underutilized in pediatrics. 8 In adults, IT has been studied in healthy athletes,9,10 and in numerous lung conditions11–14 and neuromuscular diseases15–17 and has been shown to improve inspiratory muscle function, reduced dyspnea and improved exercise tolerance.18–23 For example, adding IT to an exercise regimen in healthy young adults with obesity led to significant improvements in subjective ratings of dyspnea and objectively measured exercise capacity. 24 However, the feasibility of using IT has not been sufficiently studied in children with obesity. Therefore, the primary purpose of this study was to examine feasibility of high- and low-intensity IT in children with obesity. The secondary purpose of this study was to examine the effects of high- and low-intensity IT on feasibility, inspiratory strength, dyspnea, activity levels, and exercise capacity.
Methods
Study Design and Procedures
The Breathe-Fit trial was a single-center, partially blinded, randomized 6-week parallel group intervention trial of inspiratory training in youths with obesity being seen at the Duke Healthy Lifestyles childhood obesity treatment clinic (Fig. 1). Participants were English-speaking children 8 to 17 years of age with obesity (BMI ≥95th percentile for age and sex) being seen at the Duke Healthy Lifestyles clinic and satisfying all inclusion and exclusion criteria. Patients with stable asthma were allowed to participate. Participants (or parent/guardian) were required to have access to the internet and an approved device/computer (see Intervention section). Participants and legal guardians were required to speak and read English. Participants were excluded if they had any of the following conditions: known pregnancy, recent lung surgery or pulmonary embolism, recurrent spontaneous pneumothorax, progressive neurological or neuromuscular disorders, need for chronic oxygen therapy, or body weight greater than 300 pounds.
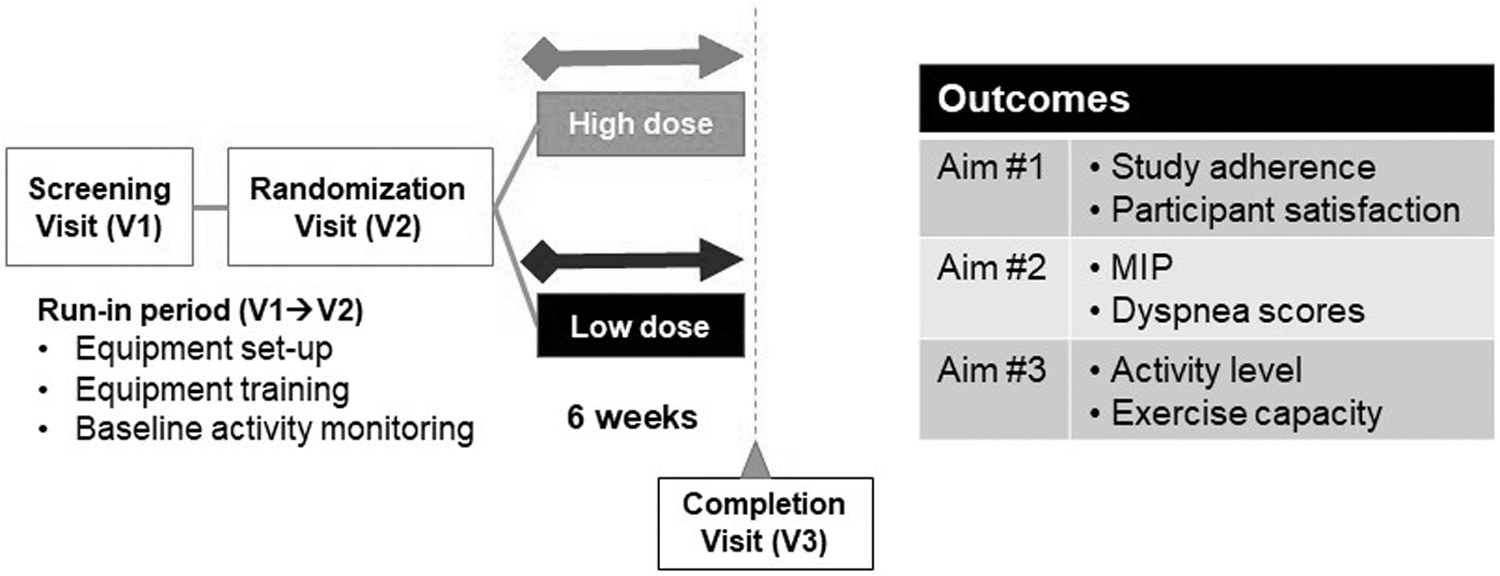
Study schema.
In brief, study staff screened the clinic schedule for initial eligibility and then approached potential patients to for recruitment and to confirm eligibility criteria. At this initial screening visit (V1), study staff obtained consent/assent for all 27 participants and gave the patient an activity tracker to wear to measure baseline activity. At the next visit (V2, about 10–14 days after V1), study procedures included re-confirming eligibility, completion of study measures, randomization, and giving the patient the intervention device. Study staff called patients or guardians approximately once each week after V2 to briefly check in and confirm there were no questions or problems with the device, until the final visit (V3) about 6 weeks later. At V3, study measures and participant closeout procedures were completed, and devices were collected.
Randomization
Participants were allotted 1:1 to either high or low inhalation resistance. Randomization assignment was obtained through the Duke REDCap randomization system in blocks of 6. One study coordinator was unblinded to ensure that the proper intervention assignments were maintained, while all participants, analysts, and remaining clinical staff remained blinded to the treatment assignment. The Breathe-Fit study protocol was approved by the Duke University institutional review board; all parents or legal guardians provided written informed consent and participants provided assent.
Intervention
Each participant was provided a PrO2™ device and trained on its use as well as the accompanying PrO2 Fit™ app (Fig. 2). The PrO2 is a flow-resistive device that provides inspiratory resistance via a fixed 2 mm orifice and has Bluetooth connectivity to most IOS/Android devices or Mac/Windows computers. The PrO2 device and app provided adherence monitoring and immediate user biofeedback to allow titration of training resistances. Participants were instructed to expire to residual volume and then inspire forcefully through the PrO2 mouthpiece (Fig. 2A) until the device signals that the user has achieved the blinded target resistance (via audible alarm and visible light signal). To achieve differing inspiratory resistances, the research team set the biofeedback signal to alert the participant at either a high or low inspiratory resistance.
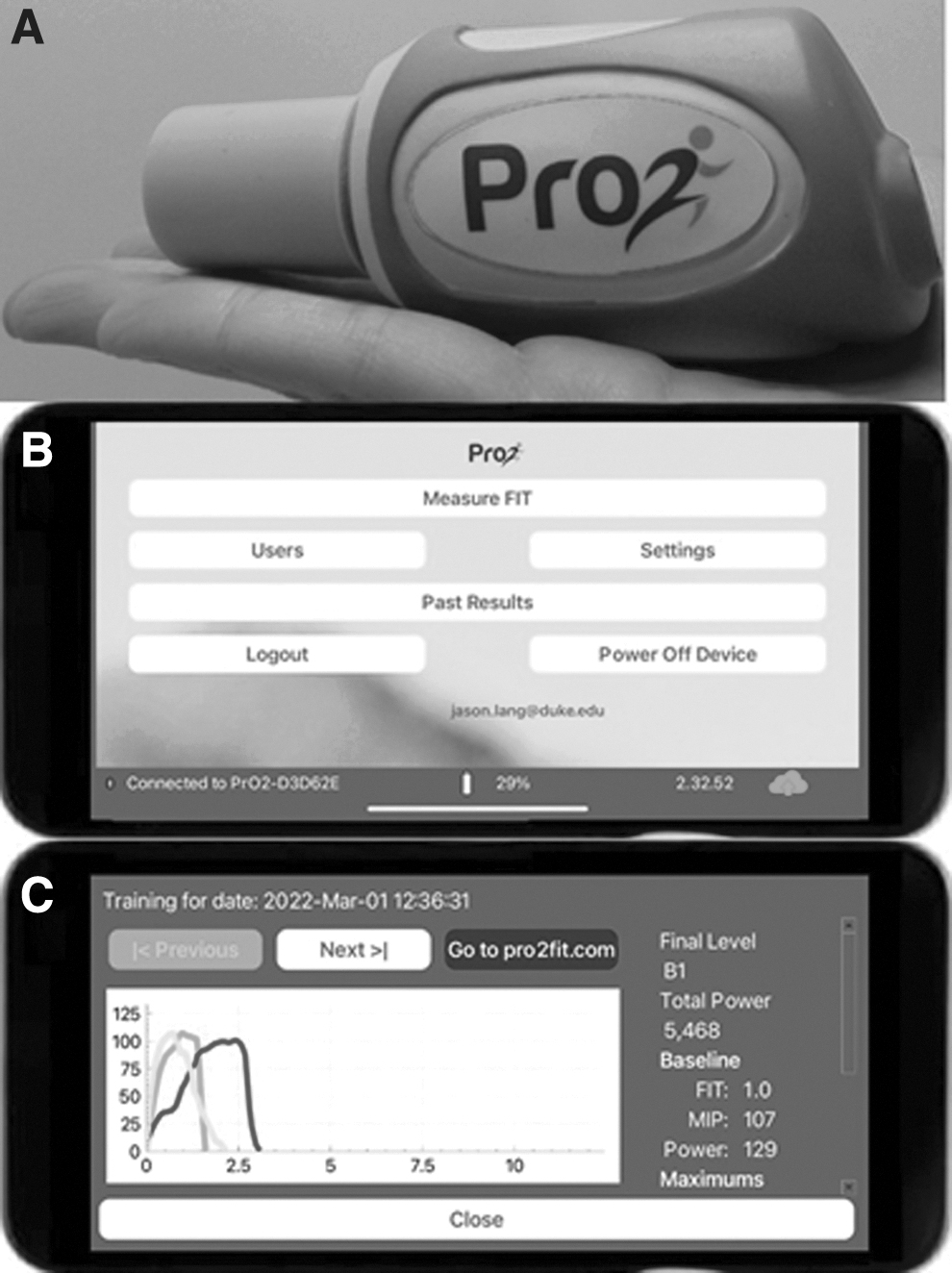
Inspiratory training device and app.
All participants were instructed to complete training sessions three times per week. In weeks 1 and 2, the target sessions involved one and two sets of 50 inspiratory repetitions, respectively. In weeks 3 through 6, participants were instructed to complete three sets of 50 repetitions. The “high” resistance group completed repetitions at 75% of each individual's individualized maximal inspiratory strength, while the “low” resistance group completed repetitions at 15% of individualized maximal inspiratory strength. To provide for exact adherence detection, all device repetitions were automatically captured and documented via the Bluetooth connection with the PrO2 app and end-to-end encrypted and transferred to a HIPAA-compliant cloud server (Amazon Web Services).
Outcome Measures
We measured the feasibility of the inspiratory training by (1) adherence to planned IT sessions and repetitions and by (2) patient satisfaction scoring. Participants were asked to indicate by Likert scale their agreement to the statement: “I am satisfied with the IT device to improve my breathing.” Adherence to IT was computed as a percent of the total expected repetitions. See Supplementary Appendix for full description of participant feedback.
Inspiratory strength was assessed using the maximal inspiratory pressure (MIP) measurement. MIP is the gold standard measure of inspiratory muscle strength and is done routinely by trained health professionals. 25 It can be completed with the PrO2 device according to published standards.25–28 Inspiratory endurance was estimated by calculating the drop from baseline in MIP after a standardized 3-minute exercise protocol.
Dyspnea (breathlessness) assessments were completed using the baseline dyspnea index (BDI) which is a retrospective participant report of dyspnea occurring during normal activities of daily living.29,30 Dyspnea during activities of daily living was assessed by asking the participants to report on their dyspnea symptoms over the previous 7 days while performing activities such as household chores, going upstairs, walking outside, and light exercise. BDI was measured before and after IT intervention; it uses a 0 (severe) to 12 (less severe) scale to assess dyspnea across three domains (function, magnitude, and effort). Dyspnea was also prospectively assessed during a standardized 3-minute exercise step-test using the validated modified Borg Dyspnea Scale,31,32 and the Dalhousie Dyspnea and Perceived Exertion Scale. 33 The Borg is a 0 to 10 scale, with a higher score denoting greater dyspnea experienced during exercise. The Dalhousie scale was developed for children using four pictorial scales to quantify whole-body breathlessness, chest breathlessness, neck breathlessness, and leg fatigue. Each 1 (least) to 7 (most severe) point scale describes the severity of body-related distress.
Each participant's level of physical activity was measured before and at the end of the intervention. Participants wore a Garmin Vivosmart 4 wristband activity tracker (Olathe, Kansas) which calculated daily steps and total time achieving sedentary, light, moderate, and vigorous activity. Tracking occurred over a 4–7-day period prior to the start of the IT intervention, and again over a 4–7-day period during the final week of the intervention. Lastly, exercise capacity was assessed by heart rate response during the standardized 3-minute step-test. 34
Data Analysis
The primary analysis involved an intention-to-treat approach using all available data. All participants with baseline and follow-up data were included in the models to estimate treatment effects. Data were assumed to be missing at random. We used two sample t tests and analysis of covariance to determine whether the mean change in endpoints from the randomization to termination visit differed between treatment groups assuming an alpha <0.05. Secondary outcomes that were continuous variables were analyzed similarly. The statistical packages SAS 9.4 (SAS Institute, Inc.). No adjustments for multiple tests were made for any primary and secondary outcomes. No data were imputed. All tests were two-tailed at a level of significance of 0.05.
Results
Characteristics of Study Participants
A total of 29 children were screened for eligibility and 27 caregivers signed informed consent. Twenty-seven children were randomized; 14 were assigned to active high resistance intervention, and 13 were assigned to low resistance intervention (Fig. 3). The baseline characteristics of study participants randomized to the two interventions were generally similar (Table 1). Among all participants, the mean age was 11.3 years and 33% were females; the majority of participants were Black or African American, and 30% had Hispanic/Latino ethnicity. More than half of participants (53%) had a current history of asthma.
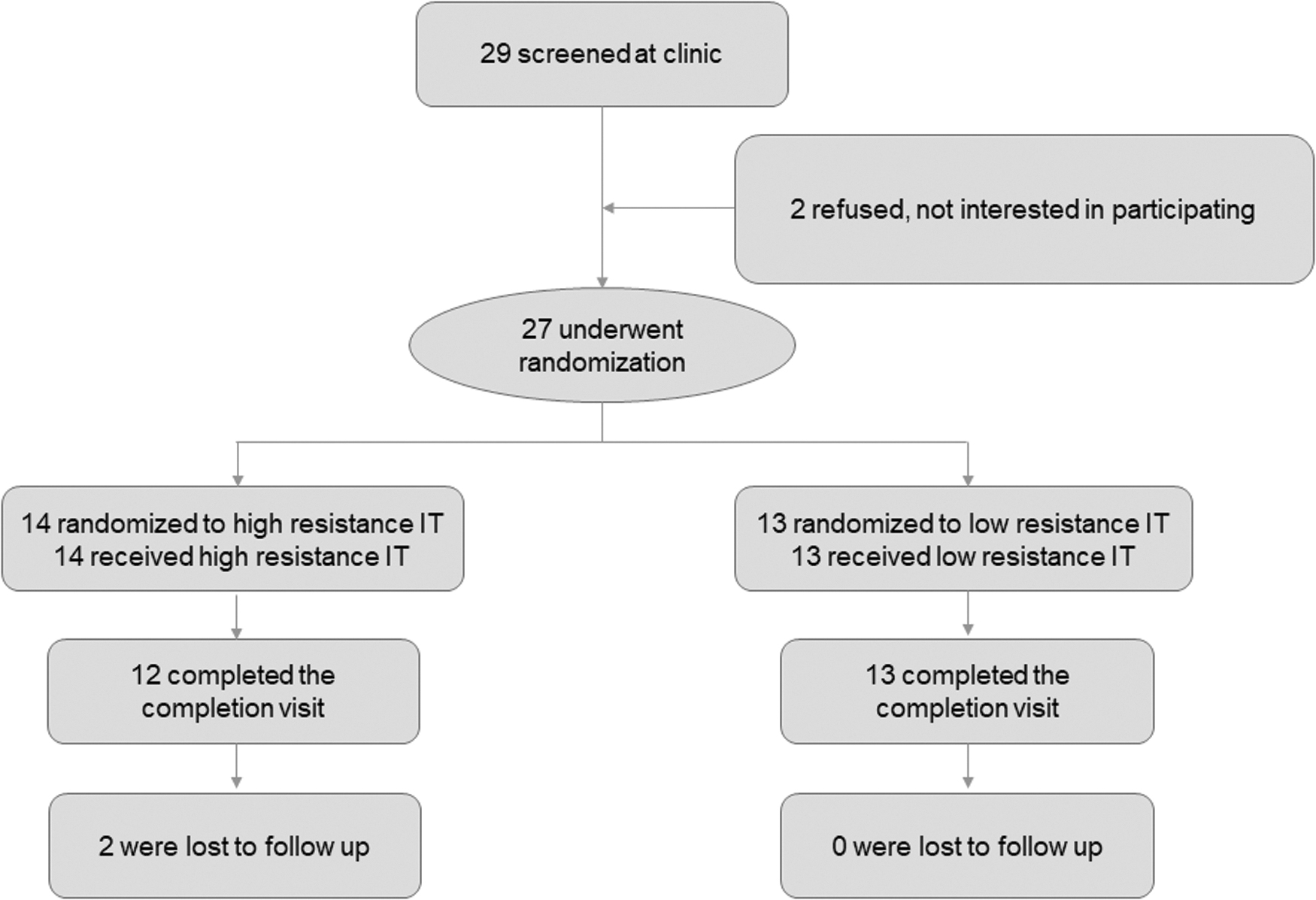
Consort diagram for consented breathe-fit participants.
Participant Characteristics
AA, African American; SD, standard deviation; SDB, sleep disordered breathing.
Recruitment, Follow-Up, and Intervention Adherence
Of the 27 participants randomized, 25 (93%) completed the postintervention study visit. Complete (i.e., 100%) adherence to the intervention over 6 weeks would yield 18 sessions and a total of 2250 repetitions. Among all participants, 72% of planned training sessions were initiated, while only 39% of the planned repetitions were completed. There was not a significant difference in session (p = 0.626) or repetition (p = 0.333) adherence between the two intervention arms. The mean number of sessions completed by the high- and low-treatment groups, respectively, were the 76% and 69% (p = 0.626), while the mean number of repetitions completed by the high- and low-treatment groups, respectively, were the 44% and 34% (p = 0.333).
Patient Satisfaction and Safety
All participants agreed that the IT device was easy to use and that they were satisfied with the IT (Table 2). We did not see a difference in satisfaction scores based on treatment assignment; participants regardless of treatment assignment generally reported they felt the IT intervention benefitted their breathing and general health. No significant adverse events were noted. Among the 14 participants with asthma, no reported worsening of asthma occurred during therapy.
Patient Satisfaction With Inspiratory Training
Scale: 1—Strongly disagree, 2—disagree, 3—not sure, 4—agree, 5—strongly agree; Values reported are median (IQR); p-values represents a nonparametric (Wilcoxon–Mann–Whitney) test comparing two nonpaired samples.
IQR, interquartile range.
Inspiratory Training Effects on Inspiratory Strength
Among all participants regardless of intervention assignment completing postintervention MIP evaluations, the mean improvement (95% CI) in inspiratory strength measured by MIP was 10.0 (−3.5, 23.6) (paired t-test, p = 0.139); while the mean (95% CI) improvement in inspiratory endurance was 8.9 (1.0, 16.8) (paired t-test, p = 0.028). There was no difference in the change in inspiratory strength (MIP) or endurance between intervention groups. The mean [standard deviation (SD)] improvement in MIP following IT for high versus low was 14 (37) and 7 (29) respectively (p = 0.581). The mean (SD) improvement in inspiratory endurance following IT for high versus low IT was 10 (23) and 8 (15) respectively (p = 0.850).
Inspiratory Training Effects on Dyspnea
Among the 25 participants completing one of the two interventions, we saw a significant reduction in dyspnea reported during daily living (Table 3). When the two interventions were compared (high vs. low), there was a nonsignificant trend toward reduced dyspnea among participants given the active intervention. Among all participants, we noted a significant reduction in maximum reported dyspnea measured by Borg during the 3-minute exercise test. These results were corroborated by the Dalhousie perceived exertion scale, with participants reporting reduced total exertion and reduced body and chest distress with exercise. However, when comparing the changes from baseline according to intervention assignment, we did not see significant differences.
Measures of Dyspnea from Daily Activities and 3-Minute Step Testing
Values are means (SD) unless noted.
Values are medians (IQR).
p-Value taken from paired t-test.
p-Value taken from independent t-test.
IQR, intraquartile range; SD, standard deviation.
Effects of Inspiratory Training on Daily Physical Activity and Exercise Capacity
At baseline, 27 participants completed actigraphy monitoring (Table 4). A majority of participants (21/27, 75%) achieved fewer than 60 minutes per day of moderate-to-vigorous activity. Among all participants completing either active or control intervention, there was a nonsignificant trend in increased total daily steps, though none of the daily activities were significantly changed from baseline. When the active intervention was compared to control, there was a similar nonsignificant trend for increased daily steps (roughly +900 steps daily) in the high intervention group (p = 0.079). Heart rates measured during the 3-minute step tests (measured by peak and average increases from baseline) were not affected by study intervention (Table 4).
Baseline and Postintervention Activity
Values are mean (SD) unless noted.
Pre- versus postintervention comparison using dependent (paired) t-test.
Comparison between treatment groups adjusting for baseline values (ANCOVA).
ANCOVA, analysis of covariance; HR, hazards ratio; MVA, moderate-to-vigorous activity.
Discussion
Our study showed that this at-home inspiratory breathing program among children and adolescents with obesity is feasible and acceptable. Our results show promise that this simple intervention may be able to affect obesity-related health outcomes including (1) reduced dyspnea with daily activities, (2) reduced dyspnea with vigorous exercise, and (3) promotion of increased physical activity. These findings raise the need for larger studies with increased power to detect and confirm clinically significant changes.
Experts recommend that youths have at last 60 minutes per day of moderate-to-vigorous physical activity35–37 though few American adolescents attain this recommendation.38–40 Thus, best practice in obesity management includes both reducing sedentariness and establishing durable increases in daily physical activity4,5; however, attrition from planned exercise programs remains high. 6 New clinical tools that support activity adherence are needed.
In our study, we recruited participants from a university-based pediatric treatment clinic for children and adolescents with obesity. We found that most participants were satisfied with the IT intervention regardless of high or low resistance. The satisfaction scores were encouraging that IT may be a feasible long-term therapy; however, the data appear to give a mixed message. Participants completed less than half of the recommended IT repetitions; however, they did engage in more than 70% of the total recommended sessions. Participants were asked to complete just three sessions per week, but a number of repetitions per sessions were likely too many for good long-term adherence. Factors commonly associated with reduced therapeutic adherence include a treatment's side effects, complexity, and therapeutic burden. 41 The side effects of physical activity as a treatment, particularly for children with obesity, can include extreme breathlessness and chest discomfort. Patients going through adolescence often also experience challenging developmental and psychosocial changes which can complicate adherence.42,43 An added complexity with children and adolescents is the involvement of parents and transition of responsibility. 41 Our results may help tailor future interventions. The adherence patterns in our data suggest that children generally do fairly well engaging with the training device on a consistent manner, but more often fail to compete the recommended repetitions once the session is started. We speculate that future trials of IT in adolescents may benefit from a similar number of weekly sessions with a reduction in repetitions per session, for example, that four to five sessions per week with a repetition maximum of 40–80 would promote better adherence while maintaining clinical benefits.
When we evaluated IT's effects on dyspnea, we found that both the high and low intervention arms resulted in significantly reduced dyspnea. We did see trends toward greater reductions in dyspnea in the high versus low group. Our study was not designed or powered to evaluate the potential mechanisms of IT. However, we can anticipate that the low group experienced improvements in endurance, while the high group experienced improvements in both strength and endurance. The IT repetitions may have also served to desensitize participants to the perception of dyspnea. Dyspnea is perceived consciously when respiratory stimuli reach consciousness via a subcortical threshold-gated mechanism. 44 Only large intensity stimuli typically generate cortical awareness. Patients could theoretically become desensitized to dyspnea if a repeated ventilatory stimulus, such as repeated inspirations during IT, is provided. Reductions in dyspnea may be related to improvements in the inspiratory muscle function, changes in airway function, alterations in central ventilatory centers, or yet detected mechanics. 7
Prior studies of IT in obesity are relatively rare. Most studies involving IT to date have included adults. In these adult studies, IT has been associated with improved inspiratory muscle strength,45–47 endurance,24,48 reduced exertional dyspnea,24,48 and improved exercise performance.24,45,46,48 It is hard to know whether or how these results apply to children and adolescents. Only one research lab has published IT results in children with obesity.49–51 This group used a different intervention approach, titrating inspiratory resistance to 50%–60% of maximum voluntary ventilation, 1 session per day, 5 days per week for 3 weeks. Importantly, the study intervention was also a part of a more comprehensive body weight reduction plan that involved psychological and nutrition counseling, caloric restriction, and exercise. Their intervention group reported significant weight loss, improvements in exercise performance and forced vital capacity (FVC), and reduced dyspnea and leg discomfort during exercise. 51 However, because these gains occurred following a multimodal intervention, it is difficult to assess the specific effects of IT in pediatric obesity.
There were several limitations to the current study. We did not employ nose-clips during respiratory muscle testing. Also, exercise-related interventions are difficult to create a true blinded comparator group. We cannot rule out some degree of participant unmasking because of the degree of difference between the high and low inspiratory pressures. Though ours was the longest IT intervention trial in pediatric obesity, 6 weeks is still a relatively short duration. Thus, it is hard to assess implications of these results over a longer duration. Also, ours was a modest-sized pilot study and had limited power to detect clinically significant effects from IT. Lastly, some of the dyspnea measures (e.g., BDI) have not been used extensively in children and should be viewed as exploratory. Strengths of the current study include that it focused on the effects of IT alone. It also used both a high and low resistance and was both randomized and partially blinded.
Our group recently completed a systematic review of IT in pediatrics. 7 We concluded that IT is a very promising nonpharmacologic option for some patients in need of improving their exercise tolerance and reducing dyspnea. The optimal resistance of IT as a percent of MIP, repetitions and weekly frequency, and duration requires additional study. Our results would suggest that low training doses may yield similar improvements in dyspnea, inspiratory strength, and activity levels. Our current study is important because it showed the feasibility and preliminary efficacy in children. Additional controlled trials that evaluate the mechanisms of IT are needed in the pediatric population in addition to trials that can offer insight into specific patient groups that may benefit most from IT.
Impact Statement
Inspiratory training (IT) has had success in other populations in reducing dyspnea and improving various health measures. Among children with obesity, IT was safe, acceptable, and viewed with high satisfaction. IT was associated with trends in reduced dyspnea and improved inspiratory muscle endurance and daily physical activity.
Footnotes
Authors' Contributions
J.E.L.: Funding acquisition, conceptualization, methodology, formal analysis, writing—original draft. V.M.C.: Project administration, software, data curation, writing—review and editing. D.M.B.: Writing—review and editing. J.B.H.: Resources, methodology, writing—review and editing. S.C.A.: Funding acquisition, conceptualization, methodology, writing—review and editing.
Funding Information
This project was funded from a grant from the Derfner Foundation (453218) and Duke University.
Author Disclosure Statement
J.E.L. reports consulting fees from AbbVie, Inc., unrelated to the current project.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.