
Abstract
Abstract
The experience of pain is affected by remarkable psychological factors. The concept of neuromatrix suggests that pain is an amalgam of affect, cognition, and sensation mediated through diverse brain regions. Moreover, the experience of pain appears to be reduced by environmental stimuli that drive attention away from the noxious events. Accordingly, immersion in a computer-generated, three-dimensional virtual environment has been used as an efficient distraction tool in a number of studies on pain management. However, no systematic approaches have explored the psychological factors that influence the effectiveness of virtual reality (VR) as a distraction technology. This review aims to outline the fundamental psychological factors involved in the use of VR to provide pain management. An analysis of the literature revealed some important elements associated with the patients' subjective experience. Eleven studies met the inclusion criteria and were included in the review. The results suggest the importance of different psychological factors in the effectiveness of the analgesic distraction. While sense of presence influence the effectiveness of VR as a distraction tool, anxiety as well as positive emotions directly affect the experience of pain. Future challenges for pain management via VR include adopting properly validated measures to assess psychological factors and using different experimental conditions to better understand their complex effects.
Introduction
C
The role of psychological factors in the experience of pain has become even more critical in light of recent work related to the neuromatrix.6–8 The neuromatrix is an extensive neural network representing the cerebral signature for pain perception. This network is deemed to mediate the pain experience itself, 9 and the authors use a biopsychosocial model 7 to describe pain as an amalgam of affect, cognition, and sensation mediated through diverse brain regions. 10 In the original model, parallel networks contribute to the sensory-discriminative (S), affective-motivational (A), and evaluative-cognitive (E) dimensions of the pain experience. 8 In this view, pain is not only an unpleasant sensory experience, but also a multisystem output that is aimed to action 11 with the primary goal of restoring the brain's homeostatic regulation system.8,12,13
Recent research10,14,15 has partially challenged the concept of neuromatrix; pain intensity can be dissociated from the magnitude of response in the matrix, and the neural configuration of the matrix also appears responsive to non-nociceptive stimuli. However, the idea of a complex pain network is still fundamental to understand how the final experience of pain is mediated by different factors, including cognitive and emotional factors.16,17 According to the review by Linton and Shaw, 18 psychological factors involved in pain experience deserve to be recognized and treated independently of physiological factors. Attention is particularly important because pain perception requires that cognitive resources be directed toward the painful stimulus. A patient's interpretation of the events surrounding the painful stimulus, expectations about pain, cognitive sets, and preexisting beliefs and attitudes all play a role in the way a patient experiences and copes with pain. Furthermore, emotional activations have a strong effect on pain experience. Not only does pain generate negative emotions such as fear and anxiety, 19 but also emotions actively mediate the experience of pain (e.g., they are associated with higher self-reported pain19,20). Moreover, recent research suggests that anticipatory anxiety related to difficult incoming situations could directly generate pain experiences, even in the absence of actual painful stimuli in the environment. 21
Given that distraction and other psychological factors influence the experience of pain, numerous interventions aimed to reduce pain in medical procedures are based on distraction techniques.22,23 Patients are engaged in tasks at the same time of their pain experience. Patients report significant pain reduction when they allocate cognitive and attentional resources to the distractor stimulus. To date, distraction techniques have used many types of materials and activities to engage patients' attentional system and help them to manage their pain. Past research has found that relaxation, hypnosis, 24 cognitive tasks,25–27 movies, and nurse coaching 28 all reduce patients' experience of pain. More recently, virtual reality (VR) has emerged as an innovative and very efficient distraction tool. In VR, a patient is fully immersed into a simulated environment by using a head-mounted display, headphones with environmental sound and/or noise reduction, and a head-tracking system that allows the patient to naturally move in the virtual environment. Moreover, VR can be interactive, so that the user is able to act within the virtual environment to achieve a goal.
Several reviews about the efficacy of VR-based analgesia have already been published,5,29,30 and some of these reviews recognize the importance of properly understanding the role of patients' individual characteristics 31 and subjective experience 32 when considering the effectiveness of VR as a pain reliever. If pain distraction is a psychological process, then psychological factors need to be considered to improve its efficacy. For this reason practitioners and researchers have experimented with distraction in different forms by manipulating its intensity and adapting their methods to different types of pain through different contexts. Additionally, VR methods vary in the technology that they employ, and experience in a VR simulator can vary based on the active contribution of the user's cognitive and emotional characteristics. 33 VR functioning and effectiveness are sensitive to the user's expectations, emotions, and engagement in the activity. To our knowledge, no reviews of VR-based analgesia have directly assessed the effects of psychological factors. Thus, we decided to focus our review on these factors to outline the psychological validation of VR-based analgesia in order to provide insights and guidelines for future implementation. In general, psychological factors influence both the experience of pain and the treatment outcome, 18 so they must be properly assessed in pain management interventions. Focusing on the particular intervention of VR-based analgesia, we then propose a theoretical discussion about the different effects of the psychological factors upon the process.
Methods
We followed guidelines from the preferred strategies to report items in systematic reviews (PRISMA 34 ).
Search strategy
A preliminary search performed independently by two of the authors identified several psychological factors analyzed in past research on VR-based pain management. Some factors are related to the subjective experience of the virtual environment, such as sense of presence or immersion; others are emotional and concern patients' individual reactions to the pain management situation, such as anxiety or fun. We then performed an extensive review of the scientific literature to identify articles investigating psychological factors, specifically immersion, presence, fun, and anxiety. A computer-based search was carried out (updated January 2014) on scientific databases (Scopus and PubMed) using the following search string: (pain control OR pain management OR analgesia AND virtual reality) AND (presence OR immersion OR fun OR anxiety).
Systematic review flow
Figure 1 illustrates the flow diagram of the review process. In total, 156 publications emerged from an initial search. All publications were individually abstract-screened by the authors on the basis of the following inclusion criteria:
a. Research article b. Experimental design (either between or within subjects) with at least one group of participants (single-case studies excluded) c. Measured at least one of the psychological factors of interest
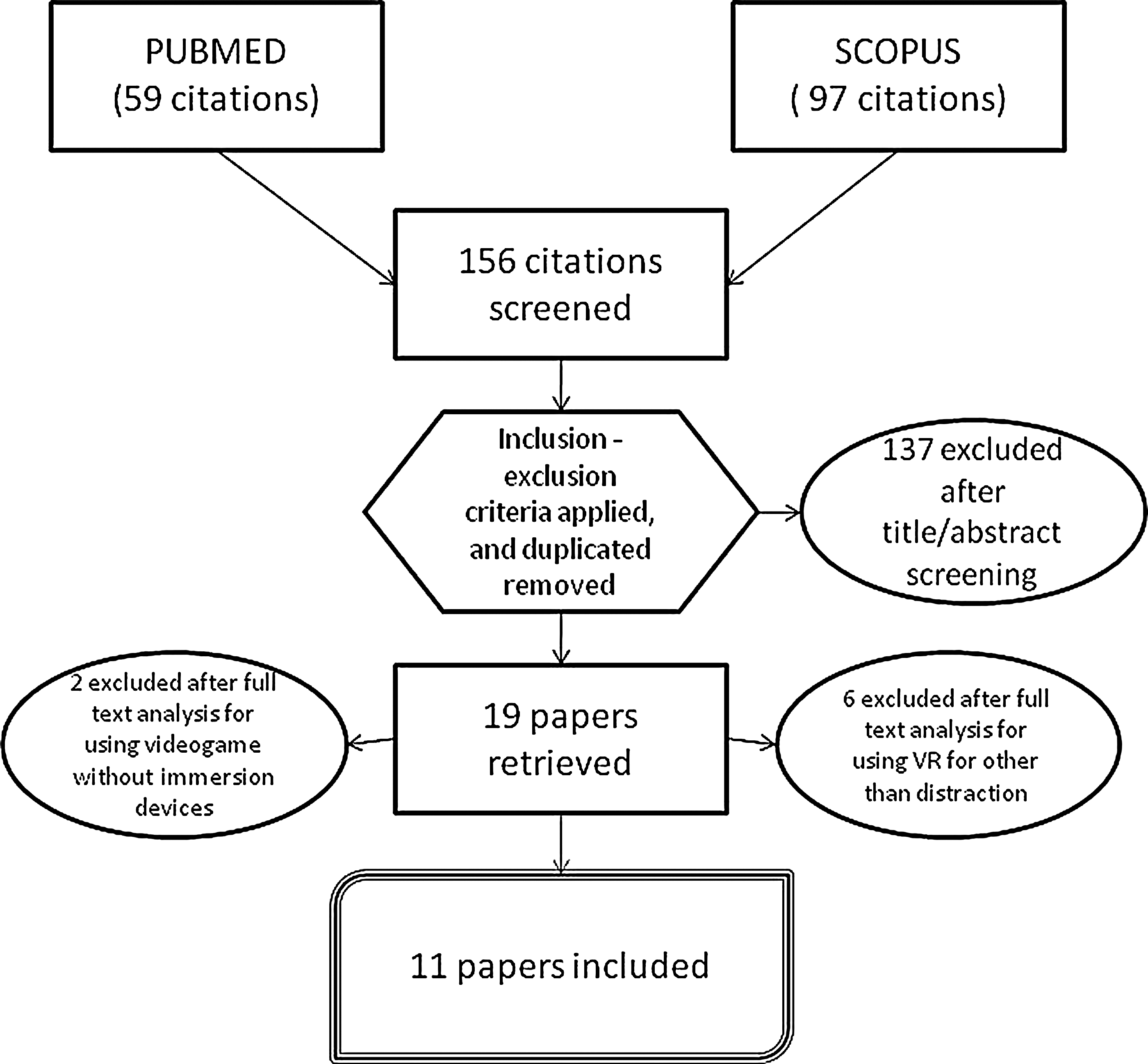
The flow diagram of the review process.
After this screening, 19 nonduplicated citations emerged. A deeper investigation of these 19 articles was performed by two authors in order to select articles that met the full criteria, resolving disagreements by consensus. This analysis excluded eight articles because VR was used for purposes other than distraction or the virtual system used was a video game without immersion devices. Ultimately, 11 articles met the full criteria and were included in this review (see Table 1 for the summary of the features of each article included).
VR, virtual reality.
Results
The selected articles will be analyzed considering each psychological factor separately. Thus, each of the following sections will take into account one psychological factor and will describe the relevant results. If one article has considered more than one factor, then it will be discussed in different sections.
Immersion/presence
There is sometimes confusion between the concepts of immersion and presence. 35 Immersion is defined as the physical/sensorial stimulation provided by the virtual environment35,36 and the degree of perceptual realism that the virtual system is able to achieve.37,38 A sense of presence is defined as the illusion of actually being in the virtual environment. From an experiential viewpoint, a VR user could feel more or less present in the environment he or she is interacting with.39–41 The sense of presence could be considered as the psychological equivalent of immersion, 42 though presence may not be described only in technical terms. If technological advancements in the VR machinery influence the sensation of “being there,” the state of mind of the user, the user's personality traits, and the arrangement of a narrative context within the virtual experience also play a fundamental role.33,43–45 For this reason, the sense of presence measured in users has been often considered as sort of “ecological validity” for VR implementations.45,46
There is surely debate about how to measure the sense of presence. Past studies have considered behavioral responses, 47 physiological correlates,48,49 and qualitative interviews, 50 but self-report instruments are the most frequently used method to assess presence. Users are asked to report their presence level on a scale when answering questions about how much they felt immersed into the virtual environment. Moreover, a number of validated questionnaires to evaluate presence are available.51,52 Ten out of the 11 studies included in this review evaluated presence. However, presence is sometimes analyzed only as a one-condition control variable. This happens when the design of a study uses an experimental group of participants who are exposed to VR distraction and a control group that either is or is not exposed to another type of distraction. Some studies only measured presence in the VR condition, given that presence is an important control for the efficacy of VR.53–57
Gutierrez-Martinez and colleagues 54 investigated the effects of VR-based analgesia in a group of 37 volunteers who were exposed to experimentally induced pain by placing their hand in a cold pressor. All volunteers participated in two consecutive sessions, one session using VR (Surreal World, a presentation of 3D environments with strange and evocative images) and the other session using only a blank screen. The session with VR produced significant reductions in pain compared with the control condition. The authors found a significant negative correlation between subjective pain ratings and presence ratings: The greater the sense of presence in the VR condition, the more attention drawn to the VR environment, and consequently the perceived pain is reduced. Similar results were found by Hoffman et al. (11 participants with burn wounds) 58 and by Tse and colleagues (72 participants with experimentally induced pain). 59 Presence ratings (or, in the case of Tse et al., 59 “the degree of immersion”) were positively correlated with an increase of the pain threshold. Furthermore, in three different studies with 88 total participants of different ages, Sharar et al. 57 measured presence in the VR conditions. Interestingly, children reported higher levels of presence (and also of perceived “realness” of the environment) than adults.
A few studies tested participants who were already experiencing pain, rather than inducing pain experimentally. Maani et al. 55 compared VR and a control condition without VR in 12 soldiers with combat related burn injuries; Gold et al. 53 used a similar protocol with 20 children who were experiencing pain from intravenous placement. Both experiments were successful in reducing pain using VR and showed that participants reported sufficient levels of presence in the VR condition. In particular, Gold and colleagues 53 consider a good presence level as an important indicator to validate their virtual environment (Street Luge) for future applications.
Schmitt et al. 56 considered the integration of VR with standard pharmacological pain therapy in a 5-day study with repeated sessions. Participants were 54 pediatric patients with burn injuries. Researchers found a meaningful reduction in pain ratings in the VR condition starting on the first day, and the reduction was maintained over the subsequent therapy sessions. Presence ratings were also affected on the first day of treatment and maintained over the course of the experiment.
Wender et al. 60 tried to understand the importance of interactivity in the analgesia effect of VR, so they compared the use of an interactive VR and a noninteractive VR with 21 subjects (pain was experimentally induced). Interactive VR showed an increase of 75% in the perceived analgesia effect compared with noninteractive VR. Presence ratings did not significantly differ between interactive and noninteractive VR. However, the opposite was found by Hoffman and colleagues. 61 Noninteractive high-technology VR showed stronger pain reduction and higher presence ratings confronted with low-technology VR in 39 students with experimentally induced pain.
The only other negative result was reported by Chan et al. 62 : Eight children with burn injuries were divided between a VR condition and a non-VR control. Children in the VR condition played an interactive game featuring an ice cream factory. Although a general reduction in perceived pain emerged, it did not discriminate between VR and non-VR and so sense of presence showed no significant correlations with pain ratings.
Fun
Users' emotional responses are fundamental for the effective functioning of a virtual environment, 63 and surely an emotional involvement appears to be strongly connected to a sense of presence and perceived realism in VR.41,43,64 For this reason, many researchers consider the concept of “fun” and evaluate positive emotions and delight in virtual applications. To date, fun has been considered in many user experience studies65,66 to the point that some usability experts describe their work as “funology.” 67 Six out of the 11 studies in the present review evaluated participants' experience of fun, all obtaining strong positive results. Hoffman and colleagues58,61 found that fun ratings positively correlated with presence ratings and pain reduction. Similarly, soldiers with high pain ratings also experienced more fun when exposed to VR. 55 In the experiments by Sharar et al. 57 and Schmitt et al., 56 participants in the VR condition obtained significantly higher fun ratings compared with participants who participated in a non-VR condition. Wender et al. 60 compared interactive VR and noninteractive VR in 21 healthy participants with experimentally induced pain and asked them to rate their fun during the most recent painful sensation. Participants in the interactive VR condition showed significantly higher ratings of fun compared with participants in the noninteractive VR condition. Taken together, these studies suggest that participants' experience of fun is a critical component of the effectiveness of VR as a pain reliever.
Anxiety
In the context of pain management, negative emotions of patients are also an important factor. Anticipatory anxiety is a well-known problem for patients who are involved in bothersome or painful medical procedures.68,69 In the field of VR-based pain reduction, a number of studies have considered the particular moment of wound care treatments in patients with burn injuries, events that are often characterized by anticipatory anxiety regarding the upcoming pain (see 70 for a review). Despite the great amount of studies measuring anxiety during VR-based interventions for pain reduction, none of them considered anxiety as a mediator of VR efficacy. For this reason we selected studies that either provided a measure of anxiety changes between pretreatment and treatment, investigated the difference between state and trait anxiety, or analyzed the correlations between anxiety and other variables affecting the virtual experience.
Chan et al. 62 considered anticipatory anxiety in their experiment, which involved eight children with burn injuries. The children played an interactive VR game while nurses changed their dressing. The researchers used qualitative interviews with the nurses, a common method to understand the relationship between pain and anxiety in medical procedures.71,72 The authors report important reductions in anxiety: During VR exposure, patients stopped crying and kicking and, with little encouragement by the nurses, started concentrating on the game without showing negative reactions to the procedure. Gold et al. 53 used validated measures to analyze affective pain (i.e., worry about the pain) and the Childhood Anxiety Sensitivity index 73 to assess trait anxiety in their sample of children undergoing intravenous placement. Anticipatory anxiety related to the procedure was also assessed. The analysis showed multiple significant correlations between measures. Affective pain increased in the control condition with no VR, but remained identical in VR condition, and was also significantly correlated with pain intensity. Anticipatory anxiety regarding the procedure positively correlated with child's general anxiety, and also with the anxiety they experienced during past intravenous placements.
State and trait anxiety may influence the effectiveness of VR differently. Tse et al. 59 induced a controlled pain in 72 participants using a tourniquet technique. They assessed anxiety with a single Likert scale (1–10 level of anxiety) before the experiment and found that participants' ratings were negatively correlated with their improvement in pain threshold during the VR stimulation. Participants with a lower level of anxiety had better improvement in pain reduction; therefore, it may be important to use proper instruments to evaluate dispositional anxiety in patients before VR interventions, such as STAI. 74 In fact, Van Twillert et al. 75 were the only researchers to measure trait and state anxiety using the STAI questionnaire. Patients with burn injuries (N=19) were either not distracted or were exposed to different distraction methods, including VR (SnowWorld), during their dressing change. A state anxiety reduction (2%) was present in conditions with VR and television, but this reduction was not significant.
Discussion
The findings of the reviewed literature indicate that psychological factors influenced the effectiveness of VR-based analgesia. These studies suggest that elements related to the subjective experience of VR influence or are related to the outcomes of interventions. In the few studies that did not find significant differences for what regard the psychological factors, such as Chan et al. 62 with presence, the analgesic effect is not significant too. The reviewed studies suggest that a high sense of presence is associated with desirable analgesia effects. It is also important that participants have fun in the virtual experience, as pleasant virtual environments tend to generate better distraction outcomes. Subjects who experience less pain also report having more fun. The role of anxiety must also be considered, as anxiety related to the intervention could be reduced by VR, and participants with low anxiety are more responsive to VR-based analgesia.
Psychological factors, considered broadly, might interact with VR-based analgesia in two ways. On the one hand, they could directly modify the experienced pain, regardless of the VR system (e.g., high anticipatory anxiety increases the amount of perceived pain). On the other hand, they could influence the efficacy of the VR technology involved in the process of pain management via distraction (e.g., high attention devoted to the VR increases its distractive properties). Figure 2 shows a schema of how the psychological factors considered here impact the VR-based analgesia process. However, we think that the study of psychological factors in VR-based analgesia is in its infancy and, to date, it has not been performed with validated and solid instruments. In the following sections, analyzing the psychological factors one by one, we provide some guidelines to develop and improve the study of VR-based analgesia in the future.
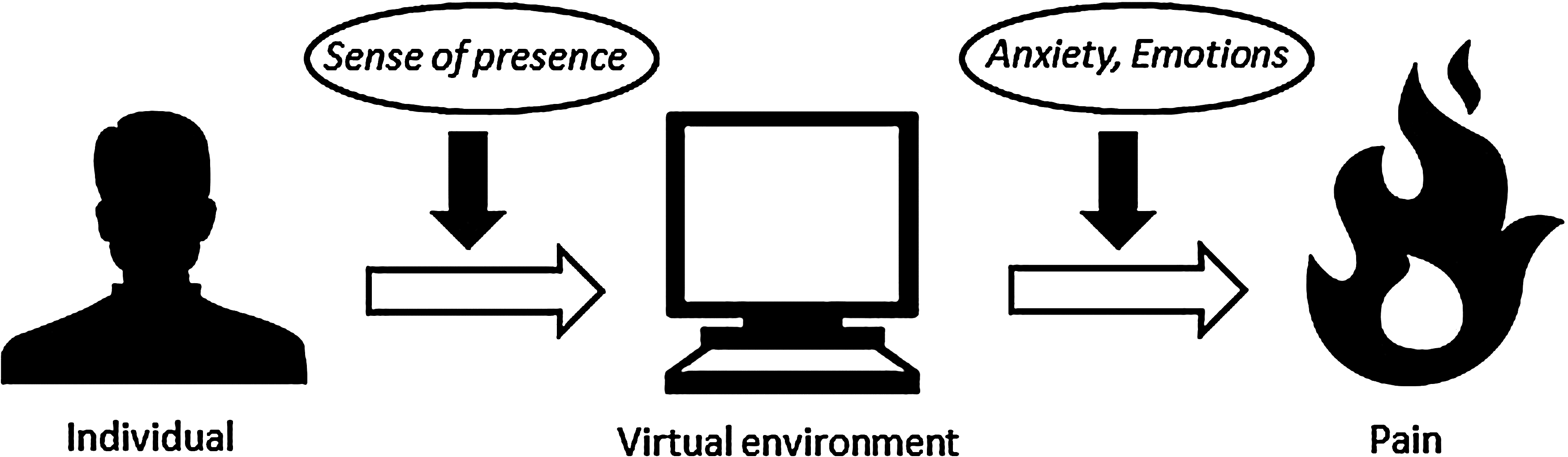
The virtual reality–based analgesia process. The experience of pain by the individual is mediated by the virtual environment. Sense of presence affects the effectiveness of the virtual environment as a distraction tool, while anxiety and emotional responses affect directly the perceived pain.
Presence
Presence may be the most important psychological factor that is directly linked to the experience of VR. The results of the reviewed studies showed that a high level of presence appears to be associated with desirable analgesia effects. The sense of presence may not have a direct impact on pain experience per se; however, presence could allow VR to be distractive from a perceptual point of view. Some recent accounts strongly link presence to attention, 76 and measuring presence informs experimenters whether their virtual representation is perceived as an environment by users. It is a place where they could have experiences, watching, hearing, and interacting with things. They could experience imaginary adventures in the VR environment and enact their intentions through the mediation of connected peripherals. 41 In conclusion, VR is a very rich stimulus that is also able to distract people from their pain, but for VR to be effective, users must have the feel of being in it. For this reason, it is important to measure presence to monitor VR-based interventions.
Ten of the 11 articles considered in this review measured the sense of presence. Unfortunately, all but two studies53,62 used a single question, such as, “To what extent did you feel like you ‘went into’ the virtual world?” Chan et al. 62 used the Presence Questionnaire, while Gold and colleagues 53 used a Child Presence Questionnaire whose reference is not provided. Research and debate on the sense of presence suggests that a number of factors generate or influence presence (see 39 for a review), so some complex questionnaires are now available to properly assess this construct. A single question may not be a complete way to measure the sense of presence, since the sensation of “being there” normally emerges from several different elements of the experience. Reducing presence to a unique question risks preventing the participant from evaluating the complexity of his or her sensations. For example, the Presence Questionnaire by Witmer and Singer 52 measures different dimensions such as involvement, perceived control, naturalness/realness of the virtual representation, and interface quality. In contrast, the ITC-SOPI by Lessiter and colleagues 51 considers additional elements, such as characteristics of the user (previous experience with technology and virtual devices) and possible negative effects that interfere with the sense of presence (symptoms related to simulator sickness).
Another issue is that researchers often measured the sense of presence as only a one-condition control variable. This is understandable because, in these cases, they compared VR with non-VR or with other distraction tools that do not promote immersion. However, to really advance knowledge about the effectiveness of VR-based analgesia, different virtual environments have to be compared. Certainly, numerous experiments and reviews today offer support to the efficacy of VR-based analgesia. However, guidelines about how exactly a virtual environment has to be conceived and designed are generally missing from past research. Hoffman et al. 61 compared high-tech VR with low-tech VR (i.e., differently advanced machineries for VR), while Wender and colleagues 60 compared interactive VR with noninteractive VR. Other comparisons are necessary in order to identify the best-performing type of technology to be used in pain management. Is one type of device better than others? Does narrative/cinematic VR provide more distraction than a simple exploratory design? Are there differences in gender or age regarding the response to different types of contents in VR? In the context of similar research objectives focused on the different types of VR, measuring the sense of presence with proper instruments could be a fundamental variable, given its strong links with efficacy.
Fun and anxiety
We combine fun and anxiety here into a single section as emotional responses. Both fun and anxiety were related to VR-based analgesia's efficacy and the two responses were always analyzed independently. The association between anxiety and pain is a well-known phenomenon in clinical settings. Scientific findings supported this common experience: Some studies demonstrated that anxiety levels can predict pain intensity.77,78 Furthermore, anxiety enhances the different components related to the experience of pain, including pain threshold, pain discrimination, and pain intensity. A possible explanation for the effect of anxiety on pain has been proposed by Ploghaus and colleagues. 79 The authors conducted a functional magnetic resonance imaging experiment in which they compared activation responses to noxious thermal stimulation while perceived pain intensity was manipulated by changes in either physical intensity or induced anxiety. Imaging data pinpointed differential activity in the hippocampus in response to identical noxious stimuli depending on the anxiety modulation. In other words, anticipatory anxiety acts as a prime, recruiting the hippocampus to amplify the aversive event and preparing the individual to behave adaptively in case of the worst possible outcome. While sense of presence intervenes on the efficacy of VR as a distraction tool, anxiety (and emotional responses in general) can also directly operate on the experience of pain.
Research on the influence of emotions on the experience of virtual environments (and vice versa) is broad80–82 (provide some diverse examples), but recent approaches that analyze the entire emotional response, and not just a priori emotional categories, have theoretical and methodological benefits. 83 Specifically, dimensional conceptions of emotions provide better recognition of ambiguous and complex affects. 84 Moreover, these models have been particularly useful for the research in applied cyberpsychology. 85 According to Russel's model, 86 an emotion is a modification of the “core affect,” a neurophysiological category corresponding to the combination of valence (positive/negative) and arousal (low/high intensity). Adaptive self-report methods such as the Self-Assessment Manikin, 87 which provides participants with pictorial Likert scales to evaluate their own experience on a variety of dimensions, are suitable to measure the emotional response in its entirety, without forcing participants into in predesigned categories. Also, psychophysiological measures could provide researchers with a more objective monitoring of emotions during the experimental tasks. The use of similar instruments and the reference to dimensional models of emotions in future research on VR-based analgesia could answer interesting research questions. How intense are emotions during treatment, and how could a high or low emotional intensity influence patient outcomes? Are emotions with positive valence (fun) or emotions with negative valence (anxiety) predominant during pain management? Can these emotions coexist, and with what effects?
Conclusions
The present review analyzed the impact of psychological factors on the effectiveness of VR-based interventions designed to distract from pain. The necessity to consider the phenomenon of pain as multifaceted is supported by the neuromatrix hypothesis. 12 According to this theoretical framework, pain is an amalgam of affect, cognition, and sensation mediated through widespread brain regions, and is likely to be influenced by several factors. A review of the psychological factors involved in VR-based pain distraction reveals that psychological factors (specifically, presence, fun, and anxiety) influence VR efficacy. However, this review also reveals some gaps and limitation in the literature, namely, that few studies in the extensive literature on the use of VR for pain management specifically considered these psychological factors, and sometimes these factors were not analyzed as influencing the effectiveness of VR. Given the present findings, we made only the first steps to predict which psychological state should be promoted during virtual experience in order to achieve a greater reduction in pain. Upon recognizing the importance of these psychological factors, it is now necessary to measure them with validated tools.
Footnotes
Author Disclosure Statement
No competing financial interests exist.