
Abstract
Abstract
Approximately 108 million people in North America and Europe suffer from chronic pain. Virtual reality (VR) is a promising method for pain management in a clinical setting due to the distracting properties of an immersive virtual environment. In this study, we demonstrated the potential use of mobile phones as a means of delivering an easily accessible, immersive experience. Thirty-one patients tested VR pain distraction. Objective measurements of heart rate correlated to decreased anxiety, while, subjectively, patients also reported reduced levels of discomfort. The positive results of this study indicate that mobile phones can provide an immersive experience sufficient to deliver pain management distraction. Because mobile devices are widely available, the potential for developing pain management programs that are accessible has become a realistic possibility.
Introduction
T
Evidence shows that there is a clear need for adjunctive pain relief. Chronic pain is the most common reason for seeking medical care. 1 Recent studies show prevalence ranging from 13% to 53% in countries throughout the world,2–5 and reaching up to nearly one-third of the adult population in the United States. 6 Chronic pain rises with age and affects a higher proportion of women than men.2–4 Although the definition of chronic pain is pain that lasts for 3–4 months, long-term surveys show that 20% to 46% of chronic pain patients have experienced pain for 10 years or more.3,7 Pain is of moderate to severe intensity for most patients, and other than opioid analgesics, few prescription pain drugs achieve acceptable pain relief in more than 50% of treated patients. 8 Even with the newer drugs, a 50% reduction in pain for 60% of patients is the best outcome achieved to date for patients with certain types of neuropathic pain. 9
A review of the FDA's 510(k) database for pain relief devices shows only five alternatives to drug therapy: three are transcutaneous electrical nerve stimulator (TENS) devices, one uses infrared therapeutic heating, and another uses neuromodulation (U.S. FDA, 2006). These devices, while effective for various types of pain, are not inexpensive or easily portable. The inclusion of objective physiological measures during VR distraction will help to determine precisely the amount of physical relief being provided by this innovative new modality.
Advantages of using a mobile phone for pain management include:
• The mobile phone is an appliance with which the patient is familiar, thus requiring minimal instruction in its use for a noncall purpose. • Graphics quality is improving continuously, and the software is completely portable, allowing anytime/anywhere use by the patient. • No computer is required, because the software purchase is added to the patient's mobile phone bill, and the download to the mobile phone is accomplished via Short Messaging Service (SMS). • Similarly, software upgrades can be performed automatically.
As more mobile phone subscribers opt for Internet service, new versions of software can be developed that allow patients to transmit real-time physiological data (e.g., heart rate, skin conductance) securely to their physicians while using the software. Along with that software, we can develop and package a set of mini-sensors for patients who wish to chart their physiological progress after using the pain management software over time. Physicians will be able to use these data to support insurance reimbursements based on objective evidence-based patient progress.
Brain imaging shows that being distracted has a real effect in decreasing the intensity of pain signals in the brain, and that VR actually changes how the brain physically registers pain, not just patients' perception of the incoming signals.10–12 Research on the effect of VR on pain shows a reduction of 30% in reports of “worst pain” (sensory component of pain), 44% in “time spent thinking about pain” (cognitive), and 45% in “pain unpleasantness” (emotional), as well as significant reductions in pain-related brain activity in all five brain regions of interest: the anterior cingulate cortex, the insula, the thalamus, and the primary and secondary somatosensory cortices. 13
VR systems are available with 3D images, motion capture, and an 80° field of view. However, most systems today require headgear to stimulate the VR and are therefore found in hospitals or clinics. Since chronic pain can exist for months to years after patients are discharged from the hospital, VR software on a mobile platform can provide easily accessible, transportable pain relief with little equipment required. 14
The challenge is proving that an easily portable pain management device with a small screen, such as that on a mobile phone, can be effective for pain relief in patients with chronic, neuropathic pain. To be effective, we believe that the virtual environment must be subjectively immersive. 15 Studies to date show that VR is effective at lessening distress, pain, and anxiety in burn wound care, chemotherapy, dental procedures, surgical procedures, phantom limb pain, physical therapy procedures, ulcer care, and venipuncture.16–23
Use of the mobile phone as a new platform for VR therapy has, however, now become an emerging research design (see Table 1).24,25
Methods
Procedure
Efficacy of mobile phone displays to deliver pain distraction VR was tested in comparison to two other methods of simulation delivery—the traditional head-mounted display (HMD), and a standard flat-panel display used as a baseline. Human factors testing was first done with controls, after which the VR was used with clinical chronic pain patients.
Controls
The VR distraction was first tested on a group of 20 participants with low daily pain intensity scores of <4 (0=no pain, 10=worst possible pain) to ensure that the distraction was of sufficient use to increase pain tolerance. In these studies, participants were asked to submerge their hand into a bath of cold water. We measured the amount of time they were able to keep their hand submerged in the water during baseline, HMD, and mobile device measurements.
Chronic pain participants
Thirty-one patients, aged 18–65 years, with current noncancer pain for at least 3 months and a daily average pain intensity score of ≥4 were exposed to virtual environments in a HMD or mobile device. These two conditions were compared to a baseline pain focus measurement. Data were collected during a 5 minute pain focus session, followed by either a HMD or mobile device VR exposure session of 20 minutes. Half the patients received the HMD exposure, while the other half was exposed to the mobile device first followed by the HMD exposure. During the exposure to the simulation, patients were instructed to interact with the simulation graphics and explore the virtual worlds.
Measures
A pain intensity scale questionnaire was the subjective measurement, which composed of a Simple Descriptive Pain Intensity Scale, Numerical Pain Intensity Scale, and Visual Analog Scale. During the exploration and during baseline, patients' physiological measures, including heart rate, peripheral skin temperature, respiration, and skin conductance, were continuously monitored. A paired t test was used to assess the differences in the pain intensity scale at baseline and during the mobile phone and HMD pain distraction treatments.
Results
Controls
Although VR has been successfully used for pain distraction for the past 15 years, we wanted to test the new mobile platform with controls to assure both safety and effectiveness. We did a number of studies, which included length of time exposed to an inflated blood pressure cuff and exposure to TENS unit (data not shown). In all these studies, the participants were able to withstand a greater degree of discomfort in both the mobile and HMD platforms.
For example, in the cold bath exposure study, at baseline, the mean length of time that participants tolerated the pain stimuli was 156 seconds, while the mobile phone pain distraction increased the mean length of time to 194 seconds, and the HMD condition increased it to 206 seconds (see Fig. 1). This initial study showed that pain distraction using these worlds on a mobile platform was effective. There were no adverse effects from using the simulation in controls. Specifically, there was no cybersickness, and the human factors analysis study revealed that the systems were easily operable.
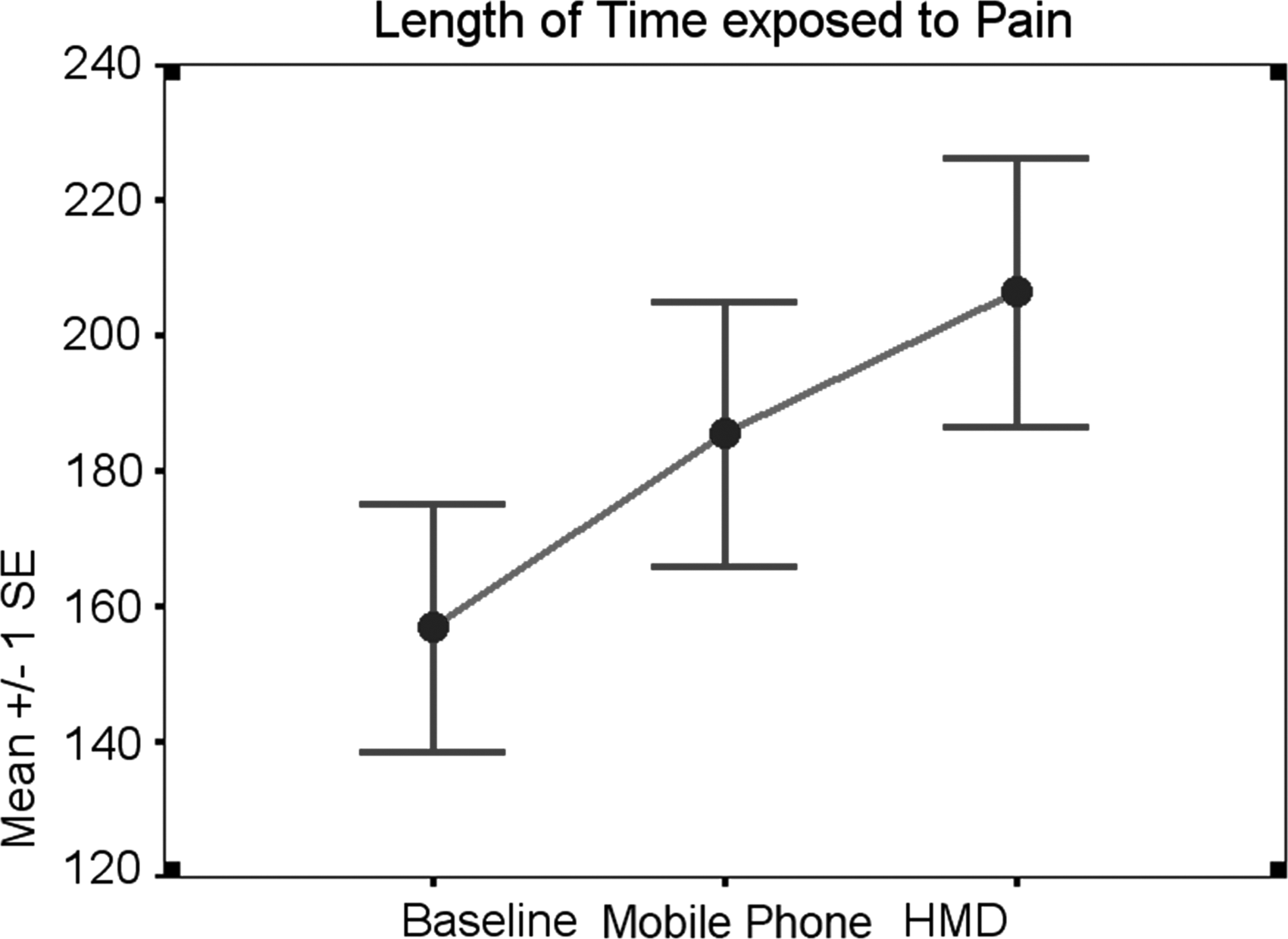
Time of pain exposure comparison. HMD, head-mounted display.
Chronic pain patients
In this study, we wanted to ensure that patients could express their pain ratings in a reliable manner. Therefore, we used the Simple Descriptive Pain Intensity Scale (see Fig. 2), the Numerical Pain Intensity Scale (see Fig. 3), and the Visual Analog Scale (see Fig. 4). All scales showed a subjective decrease in pain experienced while using both the mobile device and the HMD. While the HMD was more effective in reducing subjective pain ratings, mobile devices also were able to achieve pain reduction effectively. Half the patients experienced the HMD condition first, followed by the mobile device condition. The other half experienced the mobile device first, followed by the HMD. During these studies, patients' physiology was monitored noninvasively. Both HMD and mobile platform conditions were able to reduce the heart rate during exploration of virtual environments (see Fig. 5). The reduction in subjective pain scores correlated well with reduction in heart rate, confirming a less anxious or aroused state. In addition, patients often spontaneously reported feeling more relaxed and less stressed when using the VR.
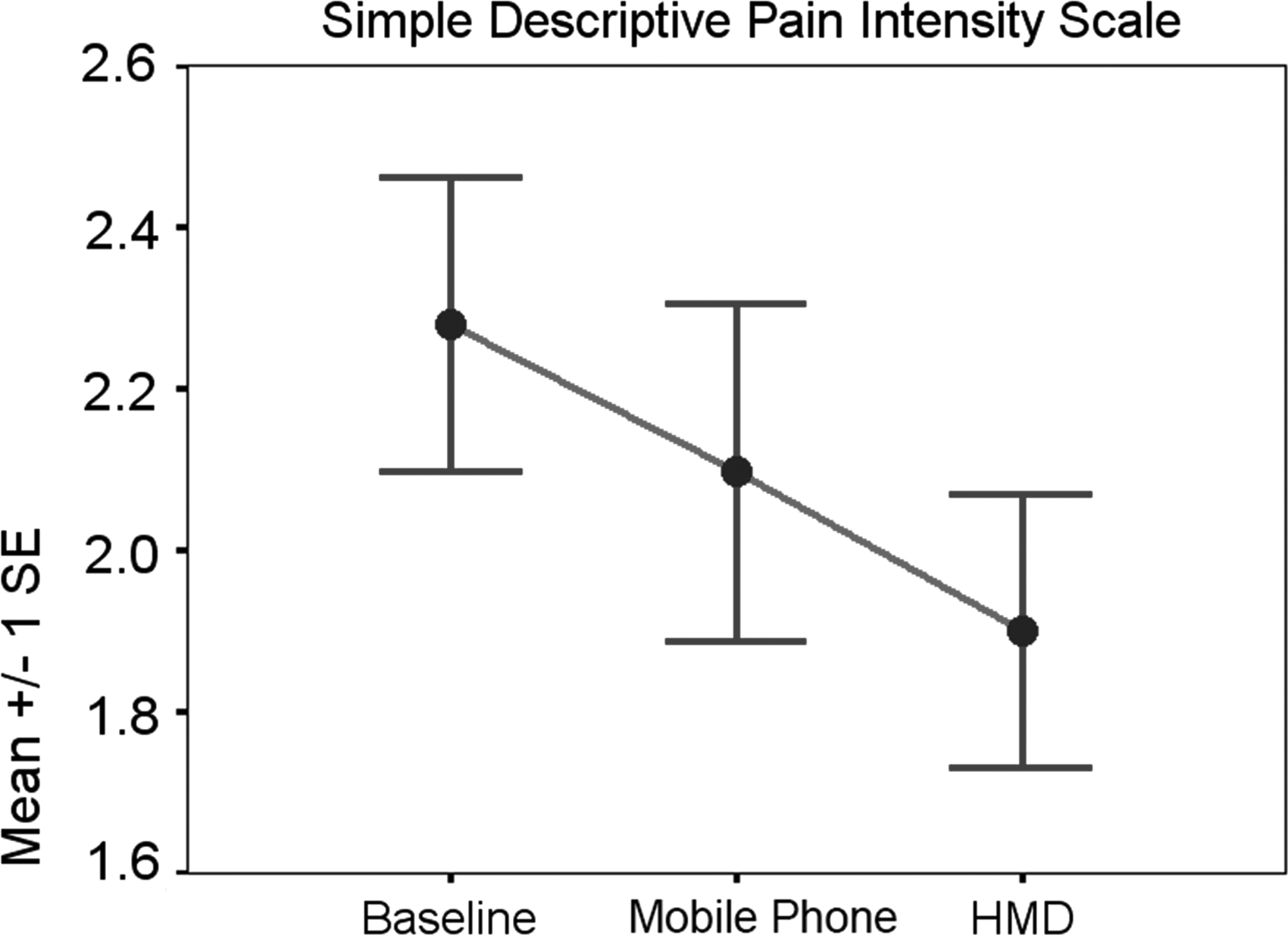
Compared to baseline, the Simple Descriptive Pain (SDP) intensity scale decreased when patients used the mobile phone (mean score decreased by 0.3). The SDP scale decreased further when patients were using the HMD (mean score decreased by 0.355, p<0.05).
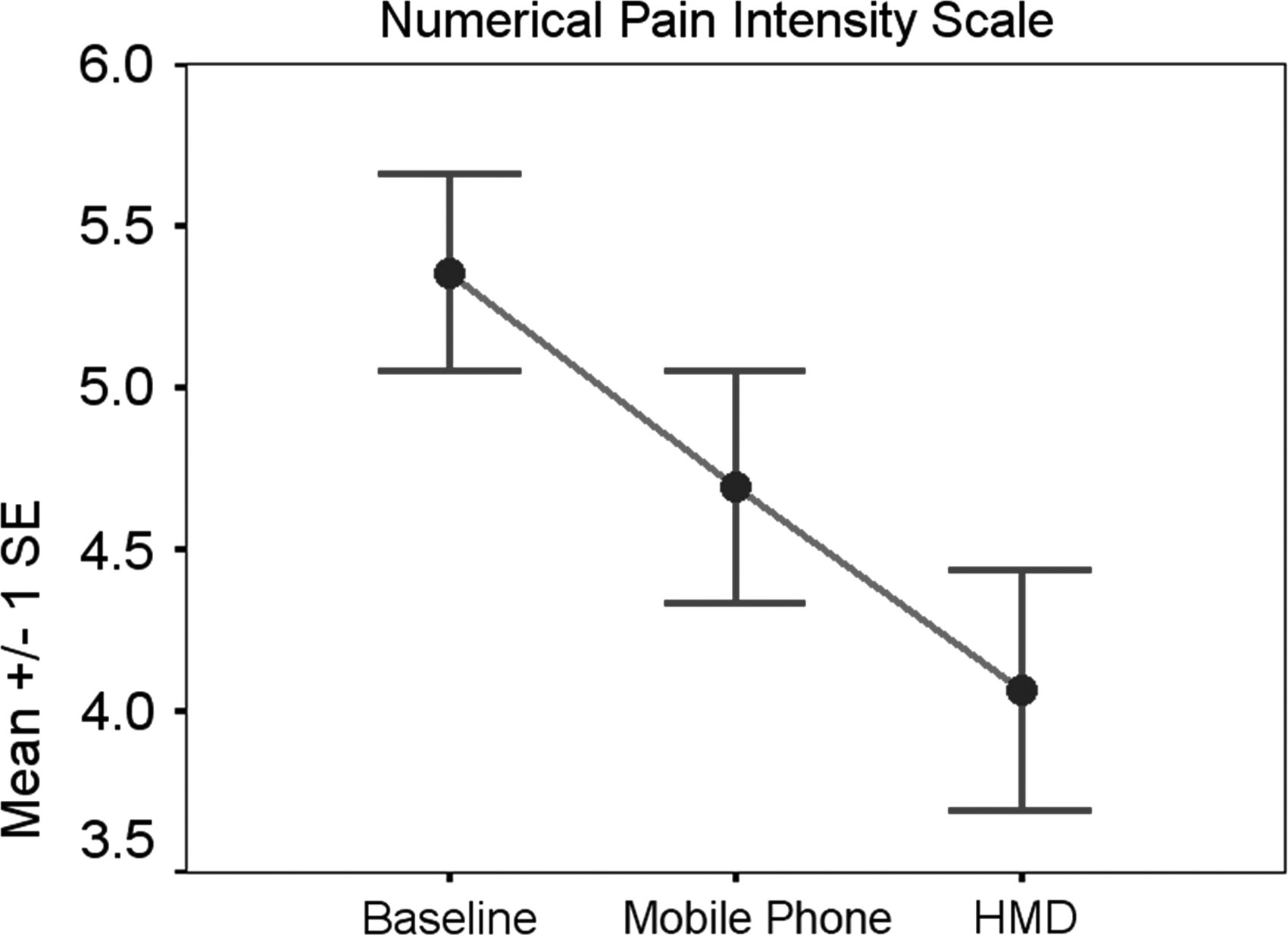
The numerical pain scale decreased when subjects were using the mobile phone (mean score decreased by 0.66, p<0.002), and it further decreased by 0.32 when patients used the HMD.
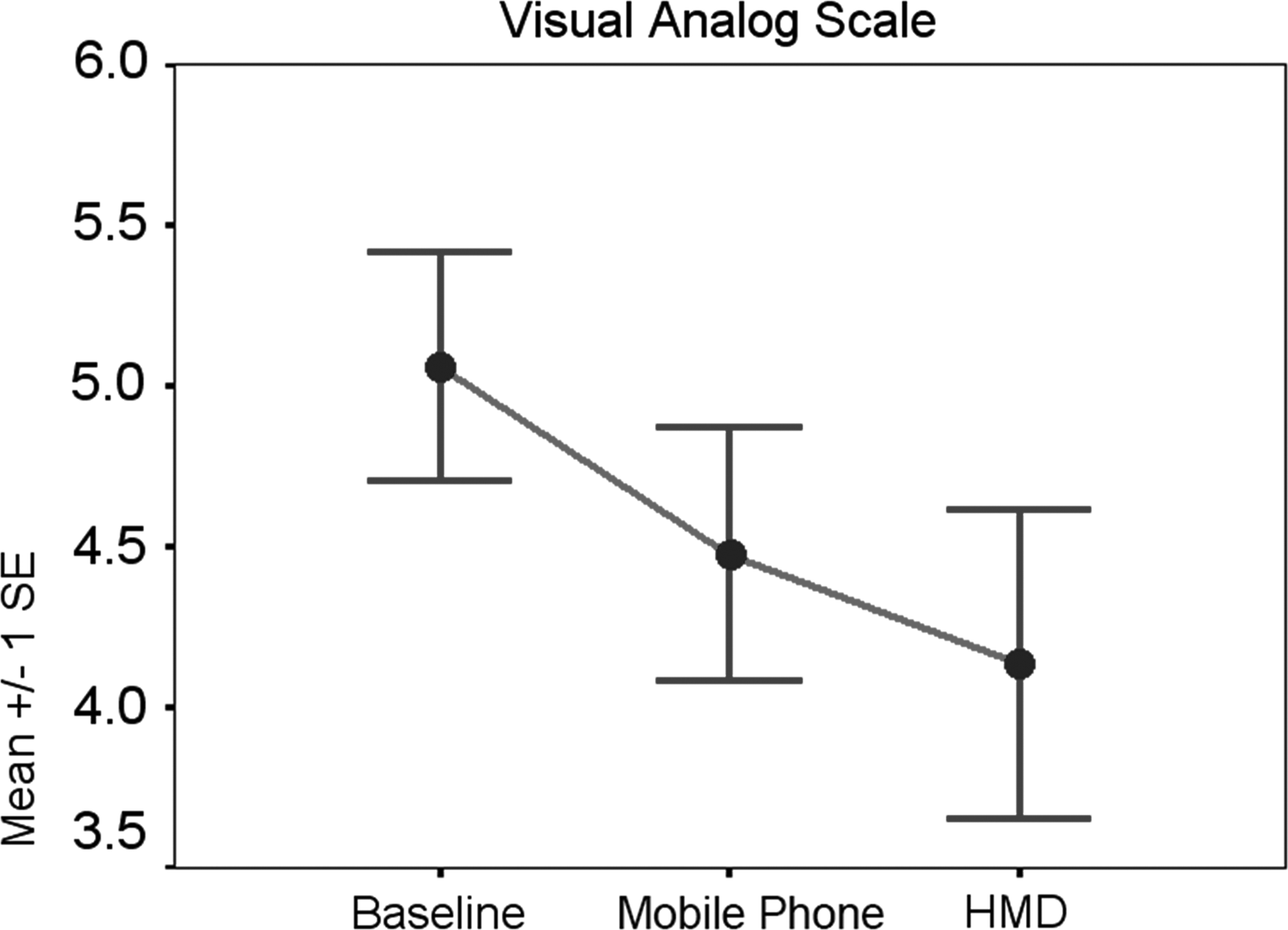
The Visual Analog Pain Scale decreased when subjects were using the mobile phone pain distraction (mean score decreased by 0.58, p<0.02), and it further decreased by 0.445 (p<0.04) when the HMD was used.
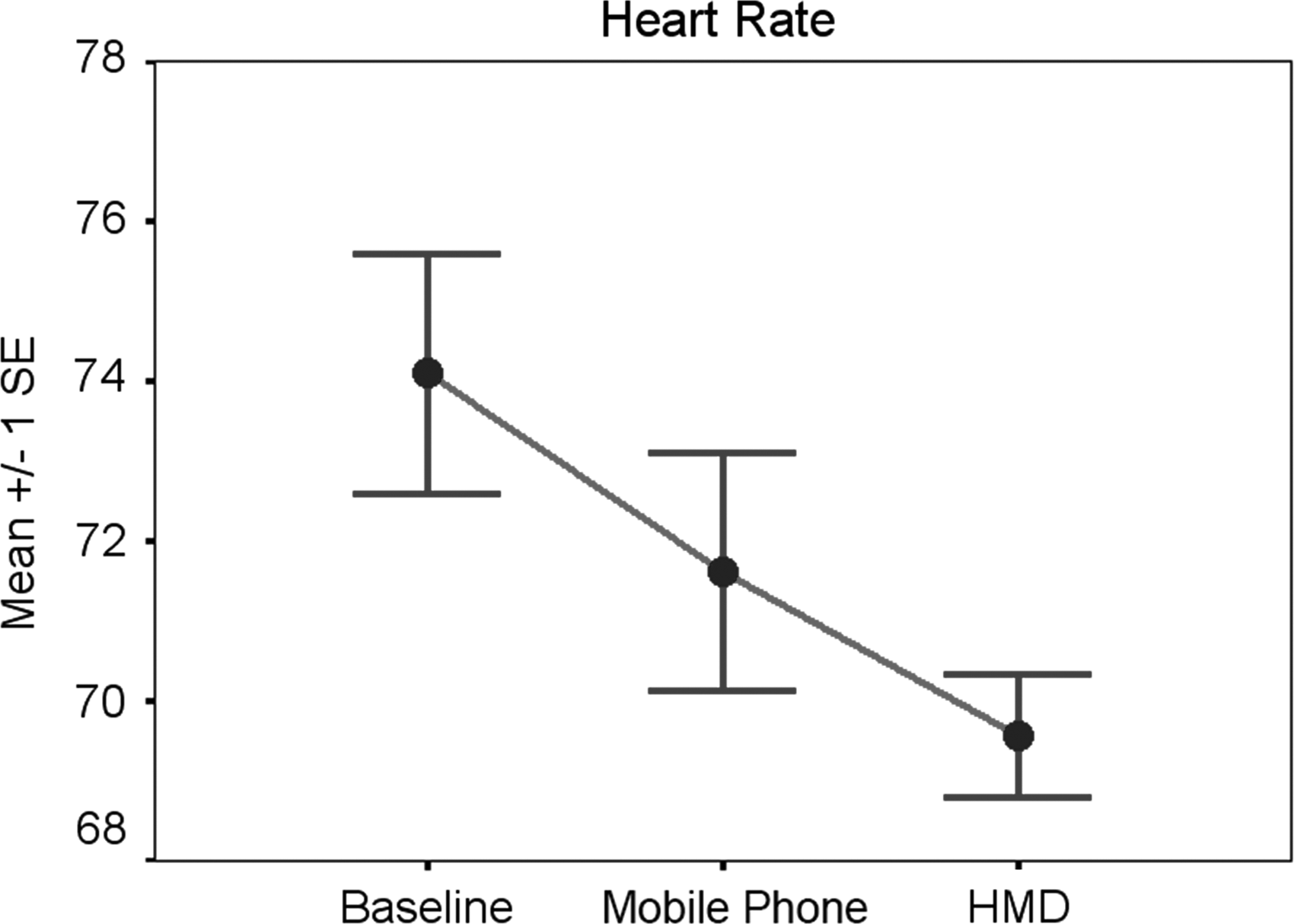
At baseline, the mean heart rate was 74 beats per minute (bpm). When subjects used the mobile phone pain distraction, the mean heart rate decreased to 72 bpm, and then decreased to 70 bpm when subjects used the HMD.
Discussion
This study demonstrated that significant reductions in pain and anxiety can be achieved using the smaller screen of a mobile device. These results were not as effective as those achieved with the full HMD immersion. From a clinical protocol point of view, it may be useful to use the HMD setting in the clinic or hospital and provide mobile devices that patients can use outside the clinic or at home. To a certain extent, there is probably a learning component that will be necessary when using the mobile device. We are currently conducting studies where we are trying to determine if initial HMD exposure results in more effective pain reduction on mobile devices. Patients who use VR for therapy often demonstrate a positive learning effect over the course of repeated sessions. The advantage of the in-clinic training is that patients are taught to recognize their levels of physiological arousal and are then taught relaxation techniques such as paced breathing and progressive muscle relaxation. We believe that the use of mobile devices should be correlated with physiological intervention to achieve the best results. In addition, the positive correlation between reduction in subjective pain ratings and improvement in physiological measures provides strong evidence that these techniques can be adapted for wider clinical use.
We are exploring the use of other mobile devices such as iPads and iPhones where real-time physiological measures are incorporated into the design of the virtual environments. In this way, the patient's own physiology will influence the visual simulation so that a feedback loop reinforces the pain reduction strategy.
In summary, we first validated the pain reduction techniques in controls and then tested them in patients with chronic pain. The mobile devices were easy to use and were not associated with any adverse effects. There was no cybersickness, and patients with chronic pain enjoyed using the systems and experienced pain relief. Larger-scale studies and longer-term follow-up are needed. These techniques, however, do appear to be both safe and effective when used in a chronic pain population.
Footnotes
Acknowledgments
We thank the National Institutes of Health and National Institute on Drug Abuse for funding this project. We also thank the participants who were willing to spend time with our clinical team to answer questions and surveys.
Author Disclosure Statement
No competing financial interests exist.