
Abstract
Public stigma associated with autism spectrum disorder (ASD) commonly stems from judgments surrounding sensory overload symptoms. As individuals try and make sense of observed disordered behaviors of those with ASD, they are quick to develop dispositional attributions instead of acknowledging situational instigators. Interventions aimed at educating the lay public that disordered actions are a result of a biological causes have been successful in lessening perceptions of responsibility, yet foster an out-group perspective allowing prejudice attitudes and discriminatory behaviors to persist. The present study examines the short-term effectiveness of engagement with a virtual simulation, Auti-Sim, to combat stigma by giving lay people a first-person experience of sensory overload. To assess Auti-Sim, a between-subject, in-laboratory experimental design was employed. A total of 123 undergraduate students were randomly assigned to 1 of 3 interventions (virtual simulation engagement, observation of simulation engagement, or reading text vignettes). Participants completed a brief pretest questionnaire, encountered the intervention, and then completed a post-test questionnaire. Engagement with the virtual simulation resulted in heightened perspective taking, which subsequently increased emotional concern, helping intentions, and willingness to volunteer compared with the observation only or text vignette intervention. Positive attitudes toward those with ASD did not differ across interventions. Fostering a different understanding of disordered action through a virtual simulation has the potential to elicit perspective taking and subsequent empathetic outcomes. Perspective taking seems to encourage perceptions of in-group belonging rather than out-group categorization and thus might be a desired outcome for stigma-reducing efforts.
Introduction
Public stigma begins when lay people identify and label differences observed in others. 1 Many of the characteristics associated with autism spectrum disorder (ASD) are visible and draw attention from the lay public and thus often lead to stigmatization. The current edition of the Diagnostic and Statistical Manual of Mental Disorder, fifth edition (DSM-5), identifies hyperresponsiveness (i.e., excessive sensitivity to sensory input), and the behaviors that often result from it, as a common characteristic of those with ASD. 2 Hyperresponsiveness occurs when your brain is unable to process the amount of input received from the senses and is described as exaggerated responses to sensory stimuli (i.e., sensory overload). 3 Sensory overload interrupts daily functioning with reactions that include difficulty focusing, extreme irritability, covering your ears or eyes, overexcitement, and high levels of anxiety, fear, and distress. 4 These reactions are often more intense than those associated with hyporesponsiveness to sensory stimuli and other ASD-related behaviors such as repetitive movements and ritualistic actions. Furthermore, given the nature of hyperresponsiveness, sensory overload often occurs in public spaces where it is difficult to control (and protect oneself or another from) overwhelming external stimuli. Indeed, sensory overload reactions are regularly viewed by lay people without prior knowledge as senseless tantrums or meltdowns and thus have been a consistent source of stigma for those diagnosed with ASD. 5 As a result of these and other observed differences, parents of children with ASD have reported various types of rejection experiences by peers (i.e., being regarded as weird, having difficulty making friends, being left out of activities, and being avoided). 6
The consequences of such stigmatization include emotional trauma, mental and educational difficulties, and diminished self-perceptions. Caretakers and family members are also affected (e.g., feelings of isolation, social exclusion, guilt, extreme levels of distress, and lower subjective well-being),7–9 increasing the risk of delayed intervention and developmental progress 10 or leading to avoidance of treatment altogether (i.e., label avoidance). 11 These outcomes are detrimental to those with the disorder and result in greater health care costs globally. 12 The current study examines an emerging and potentially powerful intervention (i.e., virtual simulations) that can combat stigma by giving people firsthand experience of sensory overload from the perspective of someone with ASD (i.e., perspective taking). This shared understanding should foster empathetic responses (i.e., emotional concern, positive attitudes, and helping behaviors) to stigmatized targets that are contrary to the negative affective and behavioral manifestations of stigma.13,14
Perspective-taking interventions
Taking the perspective of a stigmatized actor can provide people with a more holistic understanding of their disordered actions. In these cases, perspective taking encourages a layperson to shed their own identity for a stigmatized one in an effort to better understand the disordered actor's perceptual, cognitive, affective, and behavioral experiences. However, the self-concept is not disengaged by trying on a new identity, but rather one's self-concept is applied to the stigmatized identity.15,16 Thus, perspective taking helps illuminate the mental states and reasons behind disordered actions by putting a layperson in the proverbial shoes of a disordered actor and thus fostering a realization that their own motives for actions align with those of a stigmatized individual. 17
There are multiple ways to foster perspective taking. Perhaps the most common method is simply asking people to imagine the thoughts and feelings of another person in a particular scenario (i.e., imagination prompts), which has been shown to increase inclusive intergroup categorization, positive attitudes, and helping behaviors.18,19 Other researchers have used films to portray the perspective of a stigmatized target, which have resulted in social acceptance and perceptions of in-group belonging.20,21 However, there is an emerging and consequently less studied method of illustrating a disordered actor's perspective—virtual simulations. These simulated experiences allow an individual to become a virtual stigmatized actor and attempt to control disordered actions in real time. Indeed, an individual's brain should begin regulating and controlling the stigmatized actor's behavior in a similar manner as its own body, by creating its own embodied simulation of the relevant environment (virtual or real). 22 Representing and predicting actions, concepts, and emotions in real and virtual environments through the same mechanisms in the brain 22 should encourage perspective taking in virtual simulations.
Such technology has been utilized to simulate first-person experiences of stigmatized individuals and although perspective taking has not been examined, research suggests that such interventions may be an effective method for inducing perspective taking and combating stigma. For instance, engaging in a virtual simulation of color blindness increased participants' perceived oneness (i.e., overlap between the self and other) and voluntary helping behaviors toward a color-blind person.
23
Likewise, exposure to a virtual simulation of schizophrenic symptoms resulted in greater empathy and more positive attitudes toward schizophrenics than a no-treatment condition.
24
Therefore, the current study predicts that virtual simulations will promote positive responses to those with ASD by first inducing high levels of perspective taking.
Materials and Methods
Participants
Participants were 123 undergraduate students from a southwestern university who were recruited through a college-wide participant pool and received extra course credit for their involvement. a
Procedure
Participants were seated in individual cubicles and completed the study on personal computers (PCs) with 2D monitors. They first completed a brief pretest questionnaire using Qualtrics software, were then randomly assigned to one of three sensory sensitivity interventions for 5 minutes, and completed a post-test questionnaire afterward. Participants were given headphones to remove distractions and ensure uninterrupted audio.
Stimuli
All interventions began by providing participants a description of ASD and sensory sensitivity as the medical cause for sensory overload.
Virtual simulation experience
Auti-Sim was used to simulate sensory sensitivity, specifically hyperresponsiveness, which people with ASD may experience (n = 43). Auti-Sim is a free, publicly available computer simulation that is run on PCs with 2D monitors. It requires a human operator and the experience features 3D graphics and sensory (e.g., visual and audio) feedback. This type of computer simulation is a form of virtual reality and is often referred to as an interactive simulation or human-in-the-loop simulation.
25
This particular simulation places users in the body of a child with ASD on a playground with other children. As users move closer to other children talking and playing, the screen becomes blurred and distorted, while the voices of the children become jumbled and overly amplified. However, the visual and auditory distortions quickly dissipate as the user moves farther away from other children (
Observational simulation experience
In the comparison intervention, participants watched a video of another person controlling the computer simulation, Auti-Sim, described above (n = 36). This provided participants exposure to a noninteractive version of the computer simulation. The video that participants watched briefly shows someone sitting at a laptop with a pair of headphones while using Auti-Sim. The video then quickly takes the first-person perspective of the Auti-Sim character (being controlled by someone else) for the remainder of the video (Supplementary Data, Supplementary Video S1; see also Appendix Figure A2 for images of what participants observed during the video).
Text vignette experience
The control intervention provided participants a nonsimulated exposure to sensory overload reactions. This condition comprised written accounts of sensory overload episodes experienced by people with ASD (n = 44).26,27 Overall, four vignettes were used in an effort to provide participants with enough content to fill the time period designated for the other two conditions. Three of the vignettes were adapted from real descriptions of sensory overload reactions used in previous research,26,28,29 while the last vignette was adapted from an editorial piece on Auti-Sim. 30 Each vignette is between 127 and 174 words and the 4 vignettes totaled 608 words (Appendix A3).
Measures
All response options ranged from 1 (strongly disagree) to 7 (strongly agree) and example items, reliability alphas, and descriptive statistics are reported in Table 1.
Example Items and Descriptive Statistics for Study Measures
ASD, autism spectrum disorder.
Perspective taking
Perspective taking was measured using a six-item scale 31 that was originally modified from Cohen's Identification scale. 32 Researchers have utilized this scale to assess the perspective-taking process that occurs with mediated characters from films and games.20,31,33
Emotional concern
Emotional concern was measured using four items of a sympathy scale, 26 which was specifically adapted for addressing stigma related to ASD from the Pity subscale of the Attribution Questionnaire (AQ). 34 Although these scales are often referred to in previous research by one particular emotional reaction (i.e., pity or sympathy), each includes items that assess pity, sympathy, concern, and care. Thus, to achieve more accurate face validity, the present study references the variable measured as emotional concern.
Positive attitudes
Attitudes toward those with ASD were measured using 15 items from the 16-item b Societal Attitudes subscale of the Societal Attitudes Towards Autism (SATA) scale. 35
Helping intentions
Helping intentions were measured using a modified version of the six-item Helping Behavioral Intention scale, 26 which was specifically adapted for addressing stigma related to ASD from the Helping subscale of the AQ.34,c The present study had participants respond to the same six hypothetical helping scenarios, but as if they were a friend of someone with ASD instead of a teacher (i.e., “If I were a friend of the autistic person in the sensory overload situation”).
Willingness to volunteer
Participants were given a brief description of the Autism Society of America and were asked to rate their agreement with the statement “I would be willing to volunteer at the Autism Society of America.”
Familiarity with ASD
The Level of Contact Report 36 was originally constructed to examine people's experiences and familiarity with mentally ill others. Participants are asked about their familiarity with situations involving mentally ill others of varying intimacy. The current study adapted 10 situations from this report to involve people with ASD and asked participants to rate their agreement with the situation.
Results
The macro PROCESS 37 (applying model 4) was used to conduct four path analyses, one for each dependent variable measured (i.e., emotional concern, positive attitudes, helping intentions, and willingness to volunteer). Each model determined the direct effect of the intervention condition on perspective taking (H1) and the indirect effect on each dependent variable through perspective taking (H2). Bootstrapped, 95 percent, bias-corrected confidence intervals were produced to determine the statistical significance of these indirect effects. Given that intervention condition was a multicategorical predictor, indicator coding (Table 2) was used to set the proposed comparisons between conditions: virtual simulation and observational simulation (X1) as well as the virtual simulation and text vignettes (X2). Familiarity with ASD was included as a covariate in these analyses given its established association with lower levels of stigma in previous research.34,38,39
Representing the Three Conditions with Indicator Codes for Two Comparisons
Direct and indirect effects associated with perspective taking
Hypothesis 1 proposed that the virtual simulation should evoke higher levels of perspective taking compared with the observational simulation or text vignettes. Indeed, specific regression coefficients from the path analyses showed significantly higher reported perspective taking for participants from the virtual simulation compared with observational simulation [b = −0.98, t(119) = −4.73, p < 0.001] or text vignettes [b = −0.66, t(119) = −3.37, p < 0.01] (Fig. 1).
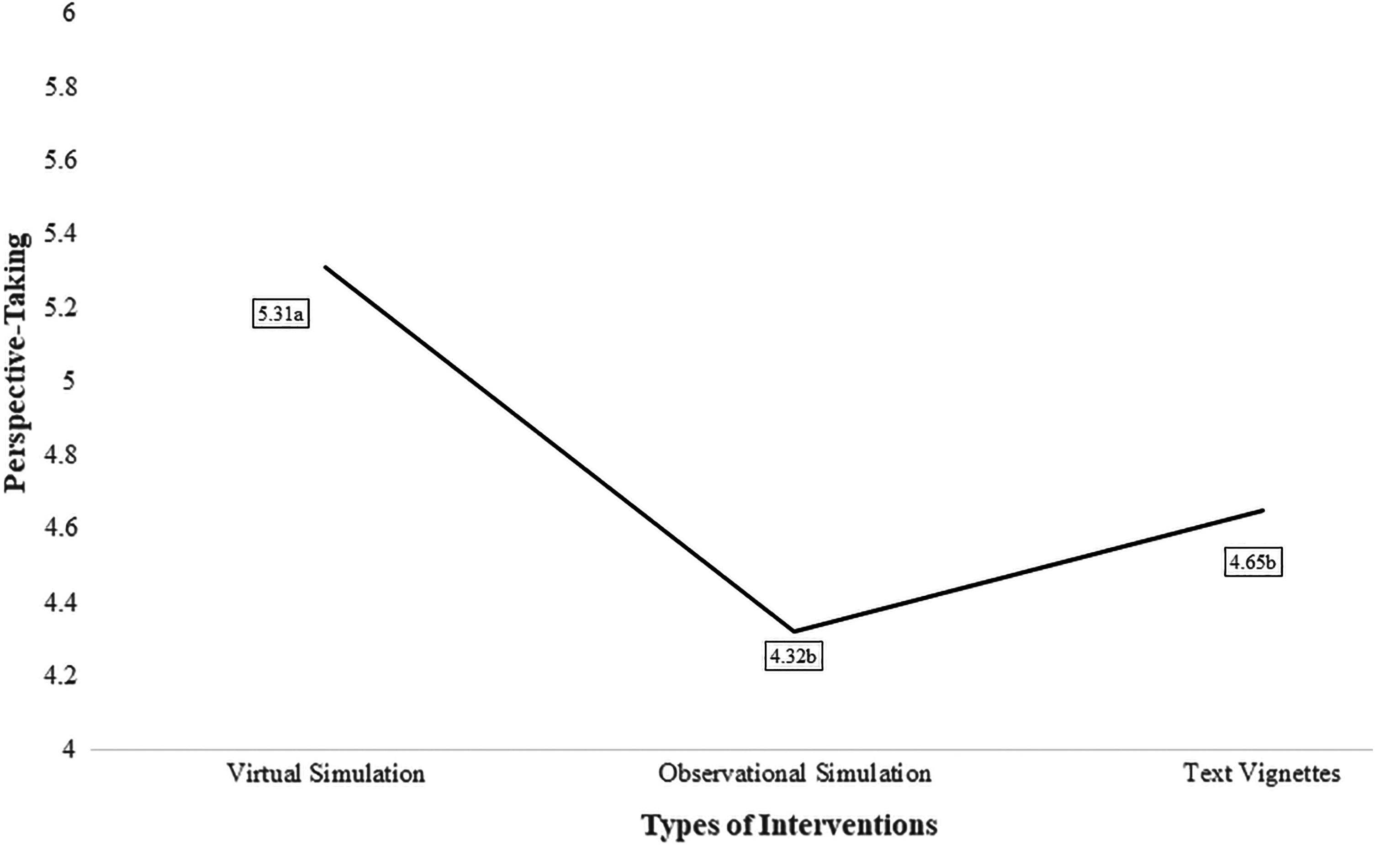
Estimated marginal means for perspective taking across intervention types. The covariate, familiarity, appearing in the model was evaluated at 4.07.
Hypothesis 2 proposed that exposure to the virtual simulation would produce more empathetic responses to those with ASD compared with the observational simulation or text vignettes as a result of the heightened perspective taking. The path analyses revealed significant indirect effects of intervention type through perspective taking on emotional concern, helping intentions, and willingness to volunteer, but not positive attitudes. Tests of the indirect effects revealed that exposure to the virtual simulation compared with the observational simulation (X1) and text vignettes (X2) produced statistically higher levels of perspective taking, which subsequently increased emotional concern, H2a: bX1 = −0.27, CI [−0.51 to −0.09]; bX2 = −0.18, CI [−0.36 to −0.05], helping intentions, H2c: bX1 = −0.21, CI [−0.40 to −0.05]; bX2 = −0.14, CI [−0.28 to −0.03], and willingness to volunteer, H2d: bX1 = −0.37, CI [−0.71 to −0.11]; bX2 = −0.25, CI [−0.51 to −0.05]. Counter to what was hypothesized, attitudes were not impacted through the perspective taking, H2b: bX1 = −0.11, CI [−0.26 to 0.02]; bX2 = −0.07, CI [−0.18 to 0.01]. Beta coefficients and model summary information for each path analysis are provided in Figures 2–5.
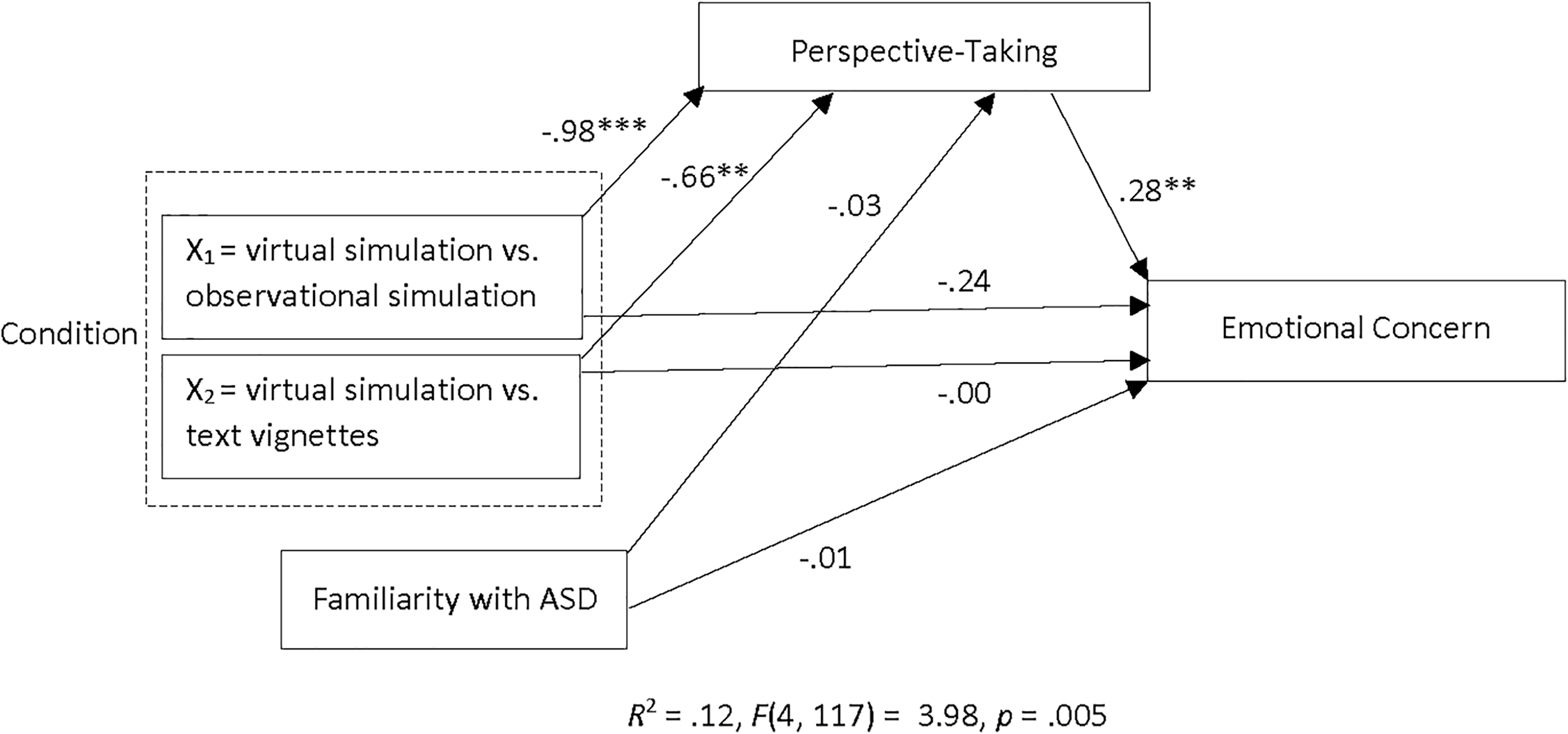
A path diagram of the simple mediation model with intervention condition as the multicategorical predictor, with three categories (virtual simulation, observation simulation, and text vignettes), and emotional concern as the outcome variable. **p < 0.01, and ***p < 0.001.
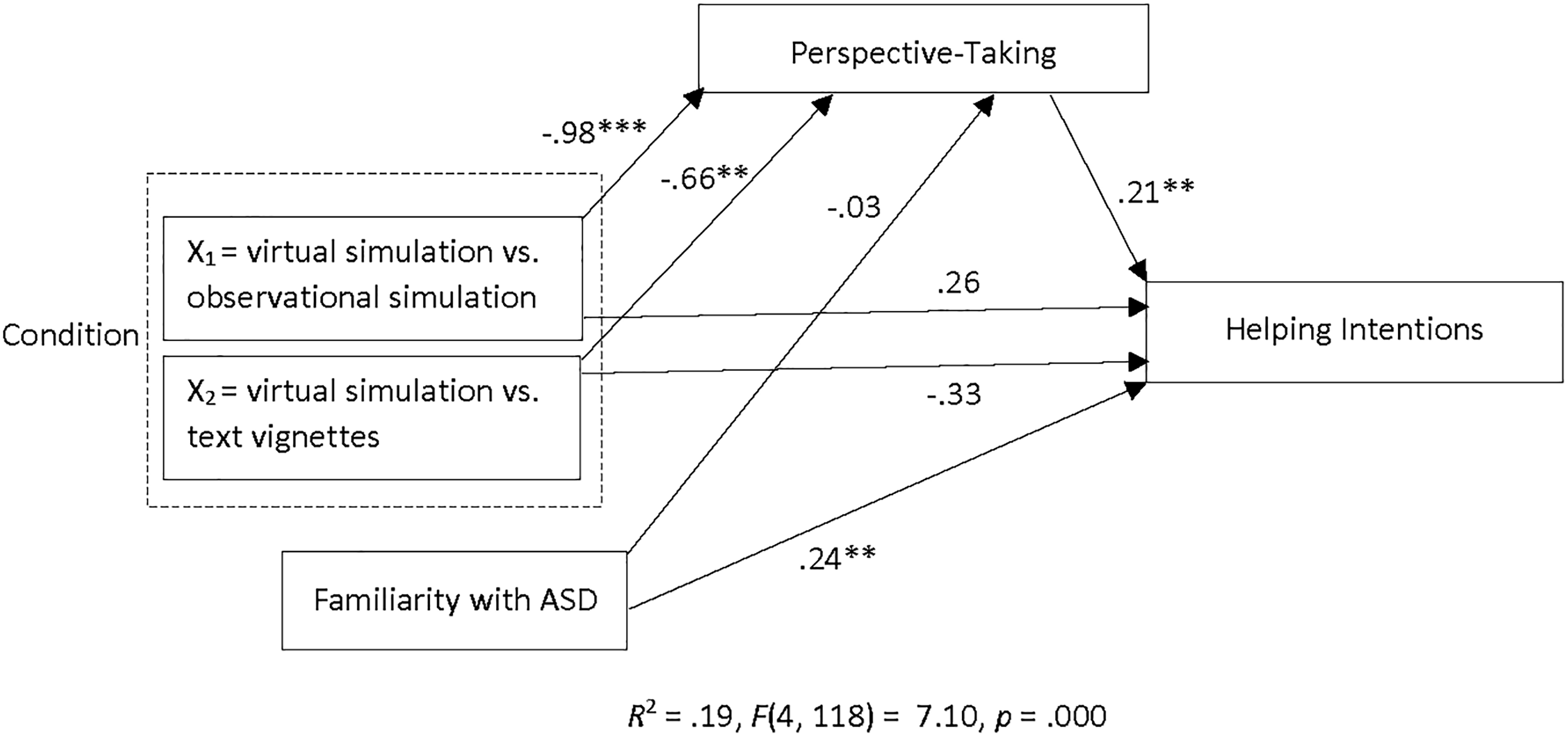
A path diagram of the simple mediation model with intervention condition as the multicategorical predictor, with three categories (virtual simulation, observation simulation, and text vignettes), and helping intentions as the outcome variable. **p < 0.01, and ***p < 0.001.
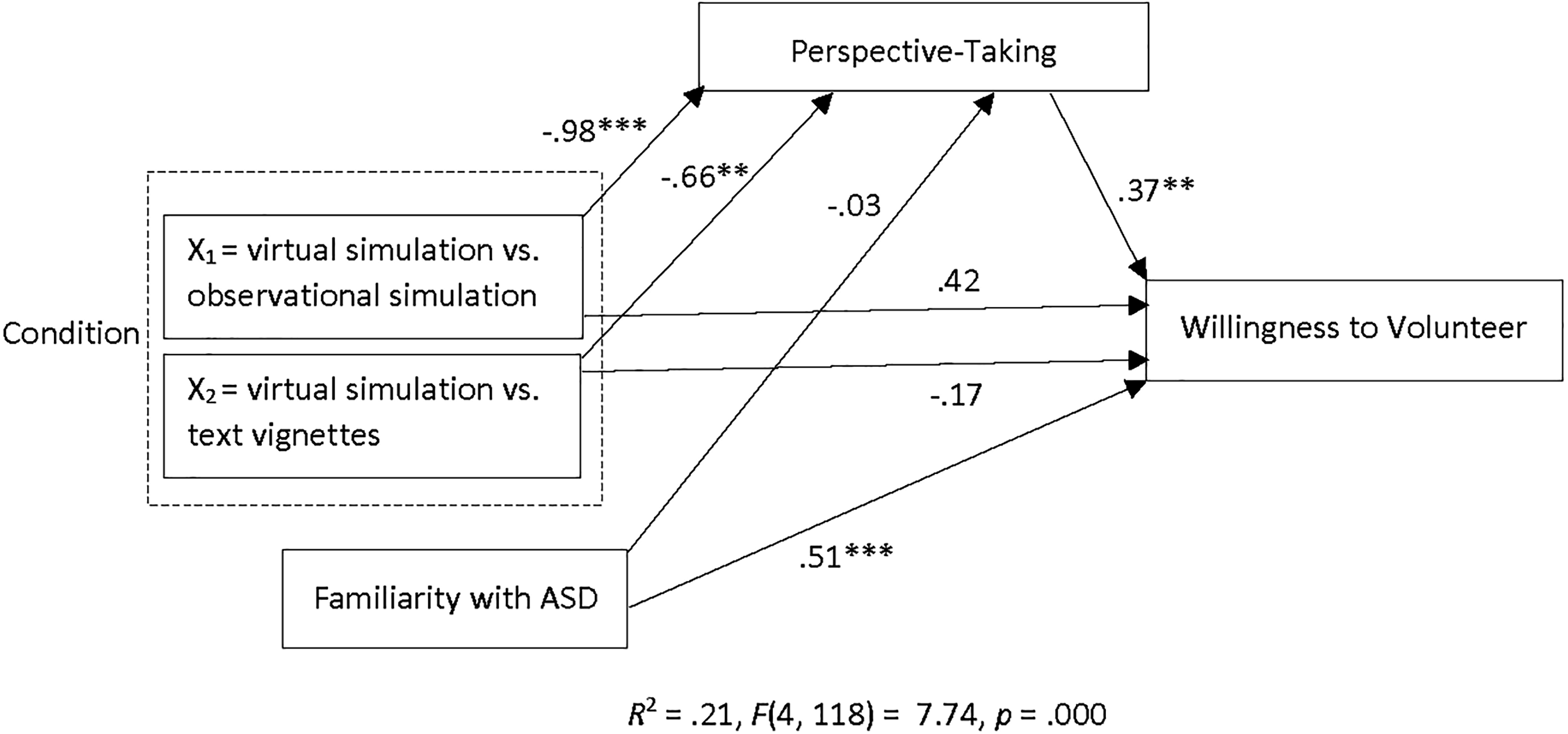
A path diagram of the simple mediation model with intervention condition as the multicategorical predictor, with three categories (virtual simulation, observation simulation, and text vignettes), and willingness to volunteer as the outcome variable. *p < 0.05, **p < 0.01, and ***p < 0.001.
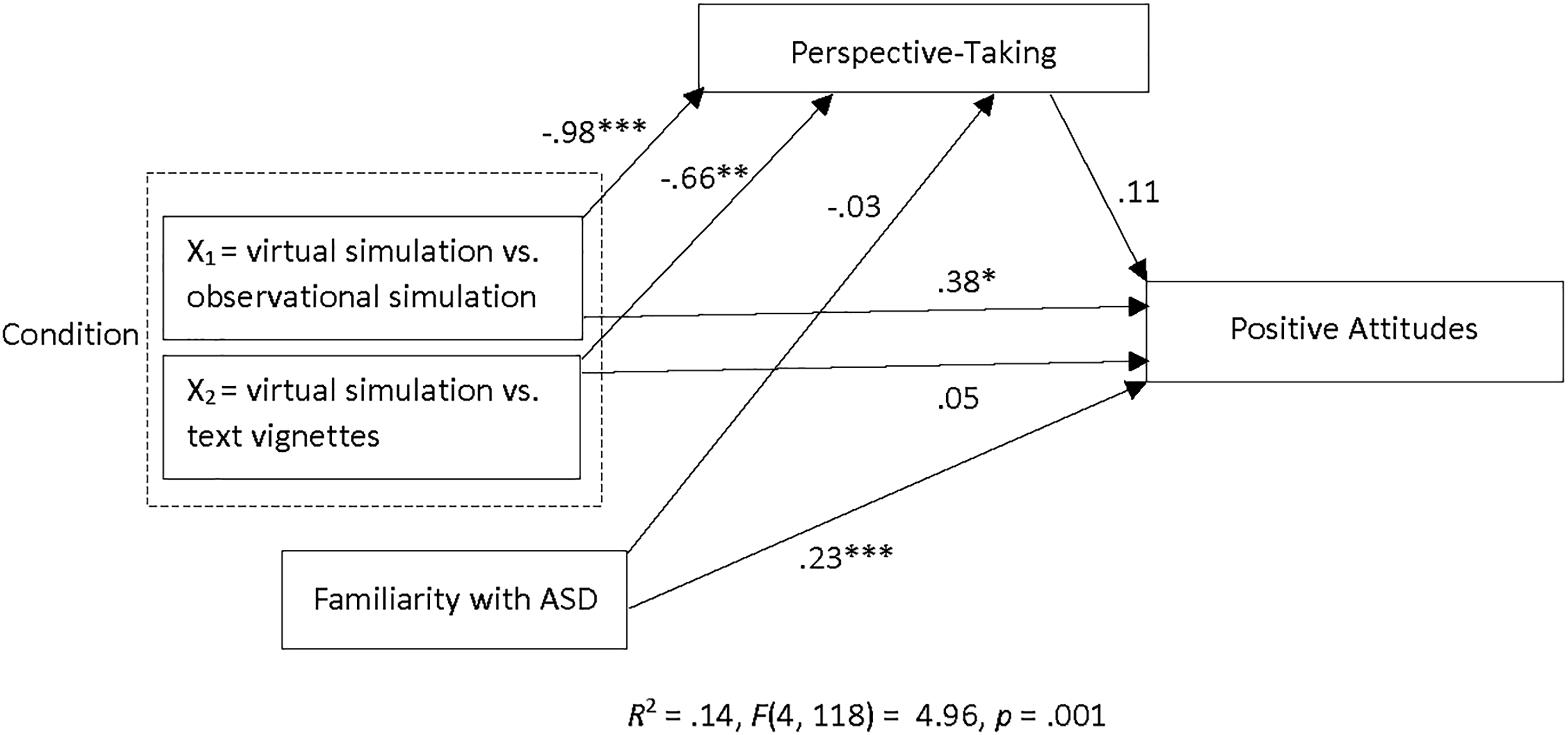
A path diagram of the simple mediation model with intervention condition as the multicategorical predictor, with three categories (virtual simulation, observation simulation, and text vignettes), and positive attitudes as the outcome variable. *p < 0.05, **p < 0.01, and ***p < 0.001.
Discussion
Reducing stigma through interventions is a difficult process, particularly when disorders carry with them symptoms (such as sensory sensitivity) that draw negative attention in public spaces. The current study examines the ability of virtual simulations to illuminate the mental states of disordered actors and thereby allow others to understand their motives for action. Findings from H1 suggest that virtual simulations can accomplish this through a perspective-taking process. Indeed, participants who interacted with a virtual simulation reported higher levels of perspective taking than watching a simulated experience or simply reading vignettes. Of particular importance is the comparison between the virtual simulation and the observational simulation condition in which participants were still exposed to the simulation, but did not control the character. This comparison helped support the notion that differences observed in perspective taking were due to first-person engagement in the simulation. Such interactive simulations virtually place lay people in scenarios, such as those experienced by disordered actors, allowing their own motives and mental states to direct their actions and reactions to the virtual environment. 22
The findings from hypothesis two showed that greater emotional concern for those with ASD as well as helping and volunteering intentions resulted from heightened levels of perspective taking. These results identify a potential route through which positive affective and behavioral responses toward stigmatized others are constructed. Although the present study did not measure specific reductions in stigma (i.e., negative affective and behavioral responses), the empathetic responses elicited by the virtual simulation's perspective taking have been associated with weaker manifestations of stigma (i.e., inhibition of aggression and antisocial behavior and improved intergroup relationships) 14 and negative emotions that fuel prejudice attitudes and discriminatory behavior toward stigmatized targets. 6 Thus, it is unclear whether the present study's positive outcomes could reduce broader stereotyped beliefs or prejudice attitudes that were already formed regarding ASD generally, but these outcomes may prevent lay people from reacting negatively to future sensory overload encounters and instead encourage helpful reactions.
Unexpectedly, positive attitudes toward those with ASD were not associated with greater levels of perspective taking and did not differ across interventions. It is possible the attitude items were subject to social desirability bias given their overt prejudicial nature and thus implicit measures may be the best method for capturing shifts in attitudes in this context. 40 Indeed, one of the most extreme items pertaining to the institutionalization of those with ASD led to unacceptable reliability in the current study and needed to be removed. On the other hand, it is possible that perspective taking encouraged by virtual simulations may only impact emotional and behavioral aspects of stigma that are more visceral, as opposed to cognitive components.
Limitations and future research
Before advocating for the use of virtual simulations for health initiatives, it is important to keep in mind the limitations of the current study and highlight the future research that can be advanced by it. First, the present study utilized a university student population. While this is a commonly studied population for public stigma interventions because many students are being exposed to new experiences and people, such as those with ASD, they may also start out with more accurate knowledge and positive attitudes and behaviors regarding ASD than the general population.41,42 Future research should replicate this work with a general population sample to see if larger differences across conditions emerge. Additionally, this initial investigation was conducted with a cross-sectional experimental design, which limits our findings to short-term effects resulting from only one dose of the intervention. Future research could adopt a longitudinal design that would track whether these positive outcomes associated with the virtual simulation are long lasting and whether multiple exposures to the virtual simulation overtime strengthen these findings.
Despite the study's small, yet statistically significant, differences observed across conditions, these improvements in empathetic responses to those with ASD may still have a cumulative impact on public stigma, which has been described not only as a process negatively affecting interpersonal interactions and intrapersonal evaluations (e.g., self-stigma) but also as a macro-level process fueling social stratification and its associated inequalities. 43 However, future research should rely less on self-report and aim to examine more concrete manifestations of public stigma and the ability of virtual simulations to reduce them. For instance, opportunities for social contact and nonobtrusive behavioral observations can capture a more natural response and realistic desire for social distance or avoidance, as opposed to self-report scales.44,45
While the present study examined only one disordered action experienced by some individuals with ASD, it is important to remember that there may be many stigma-inducing actions associated with any given disorder. Future research should begin identifying all possible actions that could be considered sources of public stigma for various disorders. Then, interventions can be tailored, such as those in the present study specifically focused on sensory overload, to combat all aspects of public stigma associated with a disorder. For example, repetitive/ritualistic actions are another common behavior of ASD that could be examined to determine if this type of action is another source of public stigma. It is easy to speculate that this action is already understood by a layperson as uncontrollable and thus likely elicits some of the manifestations of stigma associated with uncontrollability (e.g., feelings of frustration, perceptions of dangerousness/unpredictability, and avoidance/social distancing behaviors). With this particular source of stigma, empathetic responses produced by engagement in a virtual simulation might encourage patience rather than frustration and alleviate stigmatizing perceptions and discriminatory behavior.
Conclusions
One of the biggest advantages of virtual simulations is their customizability that allows them to be modified for specific purposes. As virtual simulations become more prevalent and accessible, practitioners will be able to craft virtual scenarios and environments that induce perspective taking with practically any disordered action. For example, the current study only explored symptoms related to auditory and visual senses, but other virtual simulations may begin to explore physical sensations as technologies provide richer experiences with haptics. Virtual simulations could even address situational circumstances such as the difficulties of navigating a health care system to receive proper treatment. Providing the lay public opportunities to become a stigmatized target (i.e., virtual simulations) enables them to take the perspective of a disordered actor and gain a shared understanding of their motives for action that should foster empathic outcomes and encourage helping behaviors.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.