
Abstract
The increasing prevalence of Internet addiction (IA) has been linked with a wide range of psychological disorders, including depression. We explored how IA was prospectively associated with effectiveness of treatment for adult patients with depressive symptoms (n = 241) in the context of a New York-based outpatient clinic. Although IA was not correlated with symptoms at intake, patients with higher IA attended fewer total sessions on average. Multilevel regression modeling also revealed that patients with higher IA scores terminated treatment with higher depression scores compared with those with lower IA scores. In addition, those with higher levels of IA were more likely to exhibit rising levels of depressive symptoms toward the end of the treatment, whereas patients with lower levels of IA maintained reduced depressive symptoms through termination. These results suggest that presence of IA may predict a less successful treatment outcome for adults with depression, as IA may slow down the process of symptom reduction and correlate with relapse.
Introduction
As the Internet advances in both complexity and accessibility, the incidence of compulsive, excessive, and harmful use termed Internet addiction (IA) is increasingly common. 1 Meta-analytic reviews and large-scale studies have correlated these dysfunctional levels of Internet use with a wide range of psychopathologies in adults.2,3 Among all the psychological disorders, depression may have a particularly strong link with IA, as a growing amount of recent research suggests that adults with IA not only have higher rates of depressive disorders but also demonstrate more characteristics associated with severe depression such as suicidal ideation 4 and maladaptive emotion regulation strategies. 5
Despite prior research indicating a close link between IA and depression, there is limited research with varied results on the effect of IA on outcomes for adult patients with depression. On the one hand, a small meta-analytic review of such combined treatment in adults found that psychological and pharmacological interventions showed high effect sizes for improving both IA and depression and that psychotherapy can effectively treat patients with IA and depression comorbidity. 6 This finding was also replicated by a recent clinical pilot indicating a high effect size for the treatment of comorbid IA and depression in adults with cognitive behavioral therapy (CBT). 7
On the other hand, one study examining the efficacy of psychotherapy for depressed adolescents with IA showed that CBT reduced symptoms of IA but not symptoms of depression, 8 which suggests that the presence of IA symptoms in depression cases may negatively impact depression treatment efficacy. Similarly, another study showed that although combined treatment of CBT and antidepressant medication reduced levels of both IA and depression among male adult patients, only the reduction in IA was maintained at the 4-week followup, whereas depressive symptoms recurred. 9 These findings suggest that IA may impact treatment trajectory and outcomes for adult patients with depression.
Despite the growing global incidence of both IA and depression, and the apparent relevance of IA to depressive symptoms and treatment,1,10 no study to this date has examined the effect of IA on treatment progress and outcome for adults seeking treatment for depression in a naturalistic setting in a Western country. Prior relevant studies were mostly conducted in Asian countries, and all either focused on a particular type of IA (e.g., online gaming), included homogeneous samples (e.g., males or college students only), were completed in a randomized controlled trial setting, or had IA rather than depression as the primary treatment target.2,6
In contrast, this study prospectively examined the effect of IA, assessed in a broad sense, on treatment progress and outcomes for adult patients of a diverse sample at a private outpatient psychotherapy clinic in greater New York City (NYC). We had three primary hypotheses: (a) higher levels of IA would be associated with more severe depressive symptoms at intake 2 ; (b) greater IA would be associated with a slower treatment response as indicated by longer duration of treatment 8 ; and (c) IA would be associated with less treatment efficacy as indicated by less change in depressive symptoms over the course of treatment.8,9
Method
Procedures and participants
Data were collected between September 2018 and January 2021 from all consenting adult patients presenting to the offices of a private NYC-based outpatient clinic that provided psychotherapy of a CBT or Dialectical-Behavior Therapy nature. At intake and at each treatment session, patients completed self-report measures of depression (described as follows). We have complied with the American Psychological Association Ethical Principles in collecting data as a quality assurance activity.
Inclusion criteria in the current analyses were as follows: ≥18 years of age; completion of depression measures at intake indicating “moderate” levels of depression (described as follows). In addition, based on previous research using similar methodology,11,12 we excluded subjects who received treatment for less than three sessions, as well as patients who experienced a gap of 30 days or more between any sessions in the midst of treatment so that trajectories modeled the effects of naturalistic psychotherapy and were not confounded by noncompliance. Our final sample included 241 patients who attended a total of 2,318 sessions over the course of the study (Table 1).
Demographic and Clinical Characteristics of the Sample (n = 241)
M, mean; PHQ, Patient Health Questionnaire Depression Scale; SD, standard deviation.
Measures
For demographic information, we assessed patients' age, gender, income (on an interval scale ranging from <$25,000 to >$250,000), and ethnicity using a standardized questionnaire administered at intake.
Depression was measured using the Patient Health Questionnaire Depression Scale (PHQ), 13 which yields a single total score between 0 and 27, and can be interpreted using four validated levels of depression severity: “Minimal” (0–4), “Mild” (5–9), “Moderate” (10–14), “Moderately Severe” (15–19), and “Severe” (20–27). 13 Cronbach's alpha = 0.89.
IA was assessed with Young's Diagnostic Questionnaire (YDQ), 14 including eight self-report items detailing criteria of problematic Internet use with binary response options (Yes or No). The measure resulted in a total score from 0 to 8. Five or more “yes” responses to the eight questions indicate a dependent user. 14
Data analytic plan for multilevel modeling
We examined the trajectory of change in depressive symptoms over the course of treatment using multilevel growth curve models with restricted maximum likelihood estimation. 15 Initial examination of treatment trajectories suggested that change in depression scores was best described by a cubic pattern with an initial period of rapid decline followed by a longer period of slower improvement. Adding random linear effect (ΔAIC = −292, ΔBIC = −281, χ2(2) = 295.94, p < 0.001), quartic effects (ΔAIC = −137, ΔBIC = −120, χ2(3) = 143.79, p ≤ 0.001), and cubic effects (ΔAIC = −93, ΔBIC = −70, χ2(4) = 101.24, p < 0.001) significantly improved model fit.
In addition, as per previous studies,16,17 we stratified our cubic model by adding the total treatment length as well as its interactions with fixed linear, quartic, and cubic effects, which significantly improved model fit (ΔAIC = −46, ΔBIC = −23, χ2(4) = 53.30, p < 0.001). This model represented our baseline model of treatment effect.
Results
Fifty-five patients reported five or higher on YDQ, suggesting dependence on Internet use. Correlations between continuous variables are presented in Table 2.
Correlation Matrix for Continuous Variables
p < 0.05; **p < 0.01.
IA, Internet addiction.
Our first hypothesis was there would be a positive association between patients' IA score and their level of depression at intake. This was not supported by our data, as there was no significant correlation between these two variables at intake or at termination (Table 2).
Our second hypothesis was there would be a positive association between IA and treatment length. This hypothesis was also not supported by our findings, since IA scores were not significantly correlated with total treatment length (r(241) = −0.07, p = 0.27) rather significantly and negatively correlated with total number of sessions (r(241) = −0.13, p < 0.05).
Finally, we expected that high levels of IA would correlate with less effective treatment, that is, less reduction in depressive symptoms. We estimated a series of conditional multilevel regression models building on the baseline model described earlier (Table 3). Results indicated that although the addition of IA as a main effect did not significantly improve model fit (M5), adding the interaction between IA and the linear slope significantly improved model fit (M6). Adding interactions between IA and quartic, cubic slopes, or treatment length (M7 and M8) did not significantly improve model fit.
Conditional Multilevel Regression Models for Internet Addiction and Treatment Length and Their Interaction
Finally, since there were significant correlations between IA and age and income separately, we first controlled for age (ΔAIC = 0, ΔBIC = 6, χ2(1) = 2.02, p = 0.16) and interactions between age and IA (ΔAIC = 1, ΔBIC = 13, χ2(2) = 2.47, p = 0.29) to the best-fit model this far (M6), which did not significantly increase model fit. We repeated the same procedure to control for income (ΔAIC = −1 ΔBIC = 6, χ2(1) = 2.50, p = 0.11) and its interaction with IA (ΔAIC = 1, ΔBIC = 19, χ2(1) = 4.83, p = 0.18) to M6, which also did not significantly increase model fit. Thus, we accepted M6 as the best-fitting model for our data.
Model coefficients of this final model (M6, Table 4) and graphs of resulting model predictions (Figs. 1 and 2) indicated that, on average, although patients with higher IA did not report higher depression at intake, they tended to display a slower decline in depression scores over the course of treatment when compared with those with lower IA scores. In addition, patients with higher IA scores tended to terminate or have their last recorded session with higher depression scores compared with those with lower IA scores, across all treatment lengths.
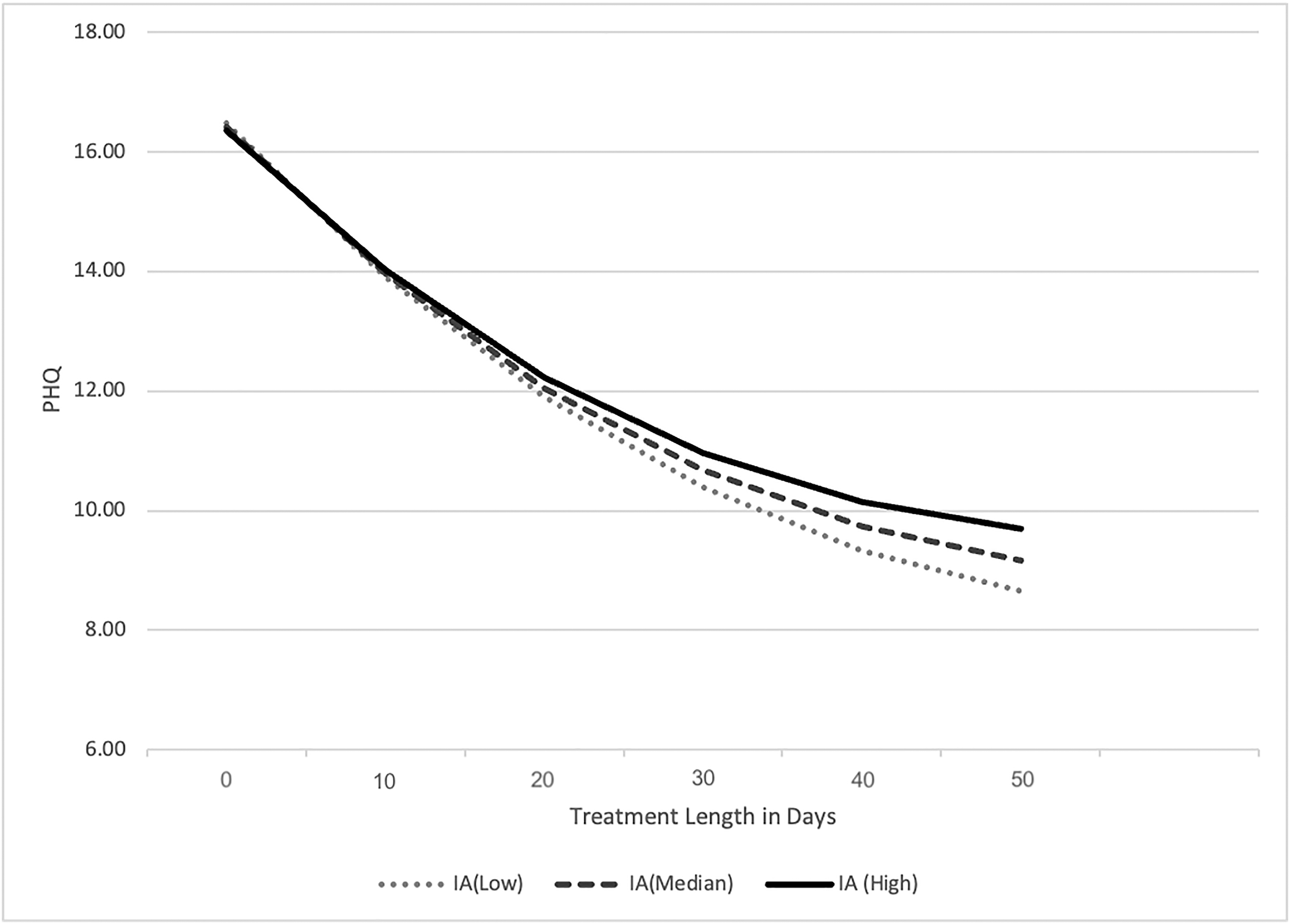
Resulting model prediction for patients receiving short-term treatments (50 calendar days from intake to final assessment). ; IA, Internet addiction; PHQ, Patient Health Questionnaire Depression Scale.
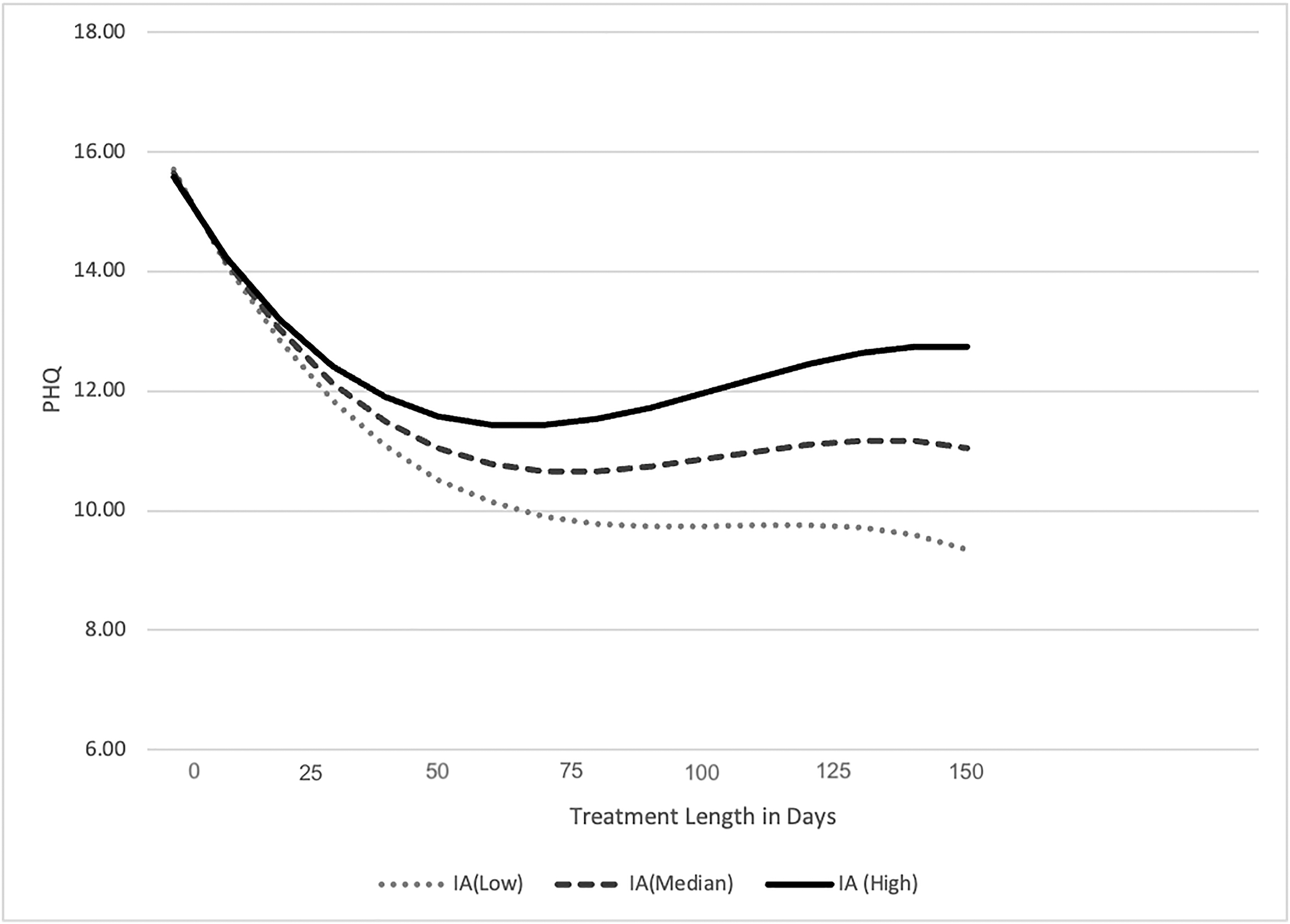
Resulting model prediction for patients receiving long-term treatments (150 calendar days from intake to final assessment).
Coefficients for the Unconditional Effect of Treatment and Internet Addiction on Depressive Symptoms (M4 and M6)
SE, standard error.
Discussion
Consistent with prior research,8,9 our results suggest that higher levels of IA might be a risk factor in predicting less successful treatment outcomes among adult patients with depression. Specifically, for patients receiving short-term treatments (50 calendar days from intake to final assessment), those with a higher level of IA tended to achieve a less noticeable reduction in depressive symptoms. Negative effects of IA on treatment trajectory were even more discernible for patients with longer-term (150 calendar days) treatment.
These findings indicate that IA may obstruct depression treatment and slow down the process of symptom reduction and correlate with eventual relapse. Although the precise mechanisms for this link remain an area for future research, these findings are consistent with the theoretical links between IA and depression. For example, if IA represents an avoidant coping strategy,18–20 it may impede behavioral activation, a commonly employed CBT treatment for depression that encourages patients to participate in active pleasure-inducing activities. 21
In addition, IA may also prevent patients from engaging in activities to build and maintain meaningful in-person social connections, the lack of which has been linked with higher depression in adults,22,23 especially during the COVID-19 pandemic period. 24 It is also possible that IA may increase engagement in behaviors that could maintain and/or magnify depressive symptoms, such as sharing risky behaviors and making self-deprecating comparisons with others. 25
Inconsistent with prior research,2,26 however, we did not find an association between IA and depression at intake or at the last session recorded. This may be a result of our research being conducted within a clinical sample, with inclusion criteria requiring patients to report at least a moderate level of depressive symptoms at the intake session. Another possibility is cultural differences, as most of the prior studies examining the association between IA and depression among adults were conducted in Asian countries with samples of college students, 2 whereas our sample was gathered in the NYC region and was more diverse in terms of race, ethnicity, age, and occupation.
Finally, our finding of negative association between age and levels of IA is consistent with prior studies indicating that a younger age of first Internet use can lead to higher levels of IA.27–29 Since younger patients are more likely to have access to the Internet at an earlier age compared with older patients, these findings suggest that IA may be a particular risk factor for younger patients with depression.
The results of the study should be considered in the context of the following limitations. First, we did not measure changes in IA across treatment, which could reveal informing details to illustrate the interplay between IA and depressive symptoms. Second, the number of recorded sessions did not fully reflect the actual number of sessions patients received, as noncompletion of session surveys resulted in some session data not being recorded. Third, our measurement of IA did not assess the content of Internet use, which may have varied impact on depressive symptoms, since different types of IA may share different risk factors 30 and, therefore, may be considered as distinct constructs. 31
Finally, this study did not collect information on the extent to which IA was targeted in treatment, which may be essential in verifying whether psychotherapy is more effective in addressing IA symptoms than depression when treating patients with this comorbidity.8,9
Despite these limitations, our results suggest there are benefits to having therapists consider levels of Internet use when planning the course of depression treatment, both in terms of noting that clients with IA may need additional sessions and that IA may be an obstacle for clients in successfully engaging in certain aspects of treatment.
Footnotes
Authors' Contributions
Writing—original draft and formal analysis by J.Z. Conceptualization and visualization by M.F. Writing—review and editing and supervision by D.H.R. Writing—review and editing, conceptualization, methodology, and supervision by S.P.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.