
Abstract
Objective:
This study assessed pulmonary safety following discontinuation and readministration of inhaled human insulin {Exubera® [EXU] [Pfizer Inc., New York, NY] (insulin human [recombinant DNA origin]) inhalation powder} in adults with type 2 diabetes (T2DM).
Methods:
Patients were randomized to receive EXU (n = 316) or subcutaneous (SC) insulin (n = 311) for 2 years (comparative phase), followed by 6 months of SC insulin (washout phase) and 6 months of original therapy (readministration). Highly standardized lung function tests were performed throughout all phases.
Results:
Small, nonprogressive treatment group differences were observed to occur early during the comparative phase for parameters such as change from baseline for forced expiratory volume in 1 s (FEV1) and carbon monoxide diffusing capacity (DLCO). These differences resolved during washout and recurred to the same small magnitude during readministration. Both treatment groups maintained similar glycemic control and hypoglycemic event rates. In the EXU group, insulin antibody (IAb) levels reached a plateau at 9 months, declined to near baseline levels during washout, and increased during readministration to levels observed in the comparative phase.
Conclusions:
FEV1 and DLCO changes observed during discontinuation and readministration of EXU therapy were consistent with a reversible, nonprogressive, and nonstructural pathologic effect on lung function in adults with T2DM. EXU readministration was not associated with an augmented IAb response.
Introduction
Clinical trials in patients with type 2 diabetes mellitus (T2DM) demonstrated that inhaled human insulin {Exubera® [EXU] [Pfizer Inc., New York, NY] (insulin human [recombinant DNA origin]) inhalation powder} was effective in patients in whom glycemic control was not achieved with diet and exercise 1 and provided better glycemic control in patients who remain inadequately controlled on either monotherapy or combination oral agent regimens. 2 –5 In addition, EXU therapy was comparable in efficacy to subcutaneous (SC) insulin therapy in patients with T2DM. 6 –8
Small but consistent, early treatment group effects in pulmonary function tests (PFTs) were observed in patients treated with EXU. 3 –7 Studies designed to specifically evaluate these effects using highly standardized PFTs found that treatment differences between EXU and SC insulin in lung function were small, developed early, were clinically insignificant, were not driven by EXU-treated subjects with large changes, and were nonprogressive for up to 2 years of therapy. 7
The primary objective of this analysis was to evaluate for the first time in T2DM patients the effects on lung function of discontinuing EXU for a 6-month washout period following 2 years of continuous EXU therapy and then readministering EXU for 6 additional months. Secondary objectives included evaluation of glycemic control and examination of the immunologic response following discontinuation and readministration of EXU therapy.
These data have been presented in part previously at the 67th Scientific Sessions of the American Diabetes Association, Chicago, IL, June 22–26, 2007. 8
Research Design and Methods
This study was originally designed as a 2-year, open-label, parallel-group comparative respiratory safety study with a 6-month washout period in patients with T2DM from the United States, Canada, and Brazil. The study protocol was subsequently amended to allow extended exposure to the initial randomized treatment following the washout phase. The study protocol was reviewed and approved by the institutional review board of each participating center, and all patients provided written informed consent. The study was conducted in accordance with the principles of the Declaration of Helsinki.
An initial interim analysis of the first 2 years of comparative treatment with EXU and SC insulin has been reported. 7 Results from the 6-month washout phase, when EXU therapy was discontinued and all patients received SC insulin, and a subsequent 6-month readministration phase when patients again received their initial randomized treatment are reported here.
Patients with T2DM for at least 1 year, 35–75 years of age, who were receiving a stable SC insulin regimen for at least 2 months and had a body mass index ≤35 kg/m2, glycated hemoglobin (A1C) levels of 5.5–11%, and fasting plasma C-peptide concentrations ≥0.2 pmol/L (≥0.6 ng/mL) were eligible for participation. Patients were excluded if they had unstable diabetes or recurrent severe hypoglycemia, poorly controlled asthma, significant chronic obstructive pulmonary disease or other respiratory disease, abnormal lung function tests (forced expiratory volume in 1 s [FEV1] <70% of predicted; carbon monoxide diffusing capacity [DLCO] >120% or <70% of predicted; total lung capacity [TLC] >130% or <70% of predicted), or had reported smoking in the previous 6 months. The predictive equations of Hankinson et al., 9 Crapo et al., 10 and Miller et al., 11 respectively, were used to establish baseline percentage predicted lung function for DLCO, TLC, and FEV1. A 12% adjustment in TLC and DLCO predicted values was applied for subjects of self-reported black race.
Following a 4-week run-in phase, during which all patients optimized SC insulin, patients were randomized at week 0 to receive either SC insulin (regular or a short-acting analog) or prandial EXU, both in combination with intermediate- or long-acting insulin (NPH insulin, ultralente, or insulin glargine). Randomization was performed using a computer-generated schedule. EXU was administered within 10 min before meals. The initial dose was based on body weight, and subsequent doses were adjusted to achieve blood glucose concentrations of 80–120 mg/dL before meals and 100–140 mg/dL at bedtime.
Primary outcome measures were change from baseline in FEV1 and DLCO during and at the end of the comparative (2 years), washout (6 month), and readministration (6 month) phases of the study. Validated and highly standardized PFTs 12 –15 were performed as described by Rosenstock et al. 7 during the comparative phase, at washout months 1, 3, and 6, and at readministration months 1, 3, and 6. All testing was performed according to American Thoracic Society guidelines. 16,17 Baseline values were defined as the means of the values collected after screening and before the first dose of randomized study drug.
Secondary end points for efficacy assessments included A1C, fasting plasma glucose (FPG), hypoglycemic events, and body weight. Baseline for A1C, FPG, and body weight was defined as the average of all measurements after screening and prior to the first dose of study drug. Baseline insulin dose was the week 0 dose of SC insulin. Hypoglycemia and severe hypoglycemia events were recorded along with insulin dose at each visit during the comparative and readministration phases only. Hypoglycemia was defined as typical symptoms without glucose measurement, but prompt resolution with food intake; typical symptoms with glucose concentrations of ≤59 mg/dL (≤3.3 mmol/L); or any glucose measurement of ≤49 mg/dL (≤2.7 mmol/L). For classification as severe hypoglycemia, all of the following criteria had to be met: (1) the subject was unable to treat himself or herself, (2) they exhibited neurological symptoms (memory loss, confusion, uncontrollable or irrational behavior, difficulty in awakening, seizure, or coma), and (3) blood glucose ≤2.7 mmol/L or, if not measured, the clinical manifestations were reversed by oral carbohydrates, subcutaneous glucagon, or intravenous glucose. Postprandial glucose measurements were not collected in this study.
Safety was assessed by monitoring adverse events and clinical laboratory tests throughout the study. Serum samples for measurement of insulin antibodies (IAbs) were collected as was done by Rosenstock et al. 7 and at washout months 1, 3, and 6 and at readministration months 1, 3, and 6.
Statistical analysis
An analysis of covariance (ANCOVA) model by visit was used to estimate the mean change from baseline PFT for each treatment group for each visit, the treatment group difference in change from baseline for each visit, and the corresponding 90% confidence interval (CI). The model included terms for treatment group, center, baseline PFT, age, gender, and baseline height. Treatment group differences and corresponding two-sided 90% CIs for continuous secondary efficacy end points were estimated using a similar ANCOVA model by visit with terms for treatment group, baseline, and center.
Analyses of PFT data collected during all three phases of the study were performed using the All Subjects Full Analysis Set (FEV1), which included all patients who received at least one dose of study medication and had a baseline measurement and at least one post-baseline (FEV1) measurement. Analyses of efficacy parameters (A1C, FPG, hypoglycemia, and body weight) and insulin dose were performed using the Extension Full Analysis Set (A1C), which included all patients who received at least one dose of study medication and had a baseline measurement and at least one (A1C) measurement during the readministration phase.
Results
A total of 635 patients were randomized, of which 316 in the EXU group and 311 in the SC insulin group were evaluated over the 2-year comparative treatment phase (Fig. 1). Of these, 315 in the EXU group and 309 in the SC insulin group entered the 6-month washout phase, and subsequently 171 in the EXU group and 170 in the SC insulin group entered the readministration phase. Overall, 85 (26.8%), 62 (19.6%), and 19 (6.0%) EXU-treated patients discontinued during the comparative, washout, and readministration phases, respectively, whereas 71 (22.8%), 69 (22.1%), and 11 (3.5%) SC insulin-treated patients discontinued during the same phases. A total of 152 patients in the EXU group and 159 in the SC insulin group completed all three phases.
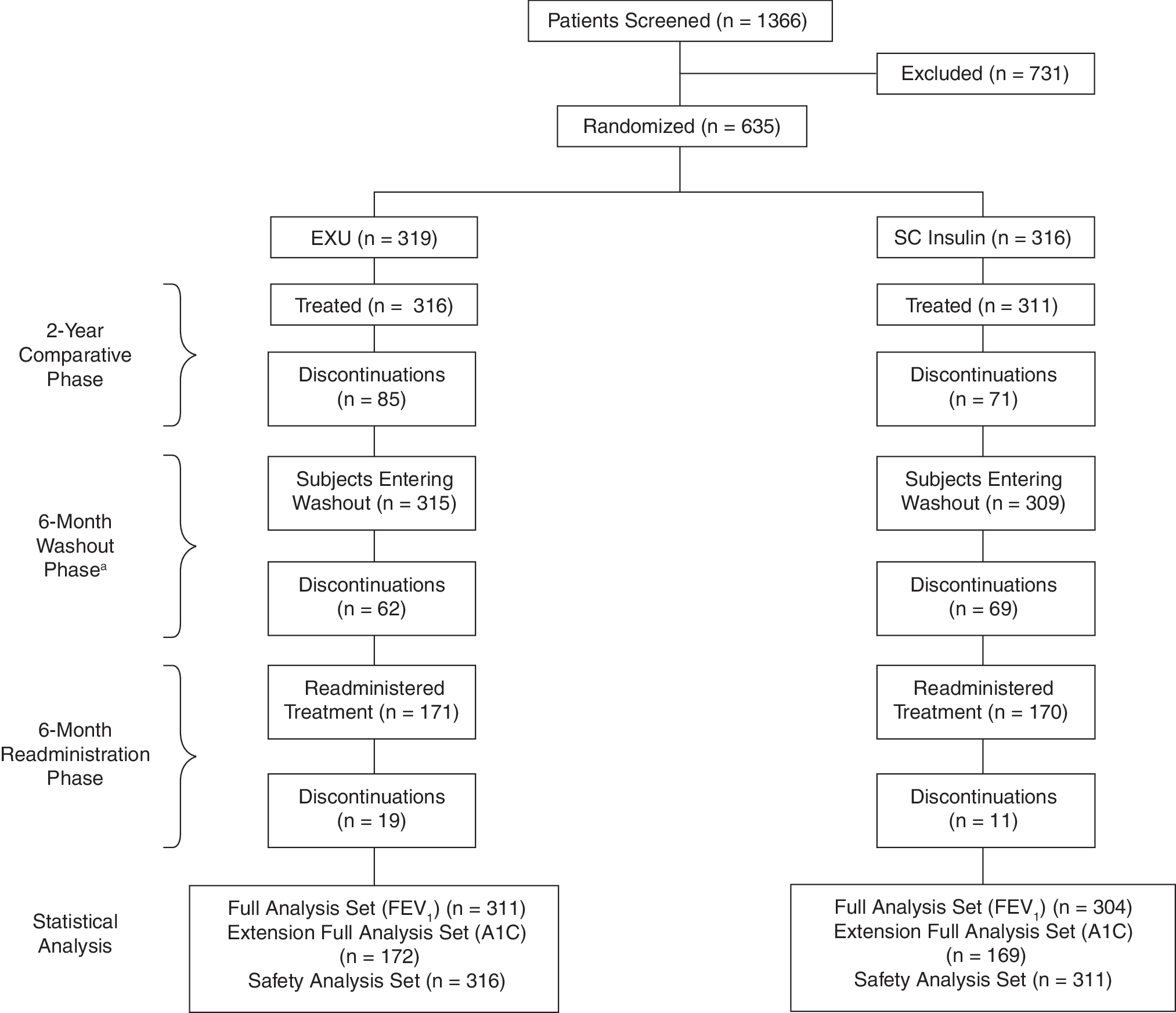
Patient disposition. Analyses of PFT data collected during all three phases of the study were performed using the All Subjects Full Analysis Set (FEV1). This set included all patients who received at least one dose of study medication and had a baseline measurement and at least one post-baseline FEV1 measurement. Analyses of efficacy (A1C, FPG, hypoglycemia, and body weight) and insulin dose were performed for the Extension Analysis, Extension Full Analysis Set (A1C). This set included all patients who received at least one dose of study medication and had a baseline measurement and at least one post-baseline A1C measurement during the readministration phase. The safety population was used to report all adverse events and included all patients who received at least one dose of study drug. aThe majority of patients who discontinued therapy during the 2-year comparative phase also entered a 6-month washout phase; however, these patients were not eligible for inclusion in the readministration phase.
As previously described, 7 demographics of patients at study entry were comparable between treatment groups. The majority of the study population was white (73%). The mean A1C level at baseline was 7.65% in the EXU group and 7.70% in the SC insulin group. Observed mean (± SD) baseline values for FEV1 and DLCO were 2.91 ± 0.68 L and 24.13 ± 5.55 mL/min/mm Hg in the EXU group and 2.93 ± 0.71 L and 23.96 ± 5.70 mL/min/mm Hg in the SC insulin group.
Pulmonary function
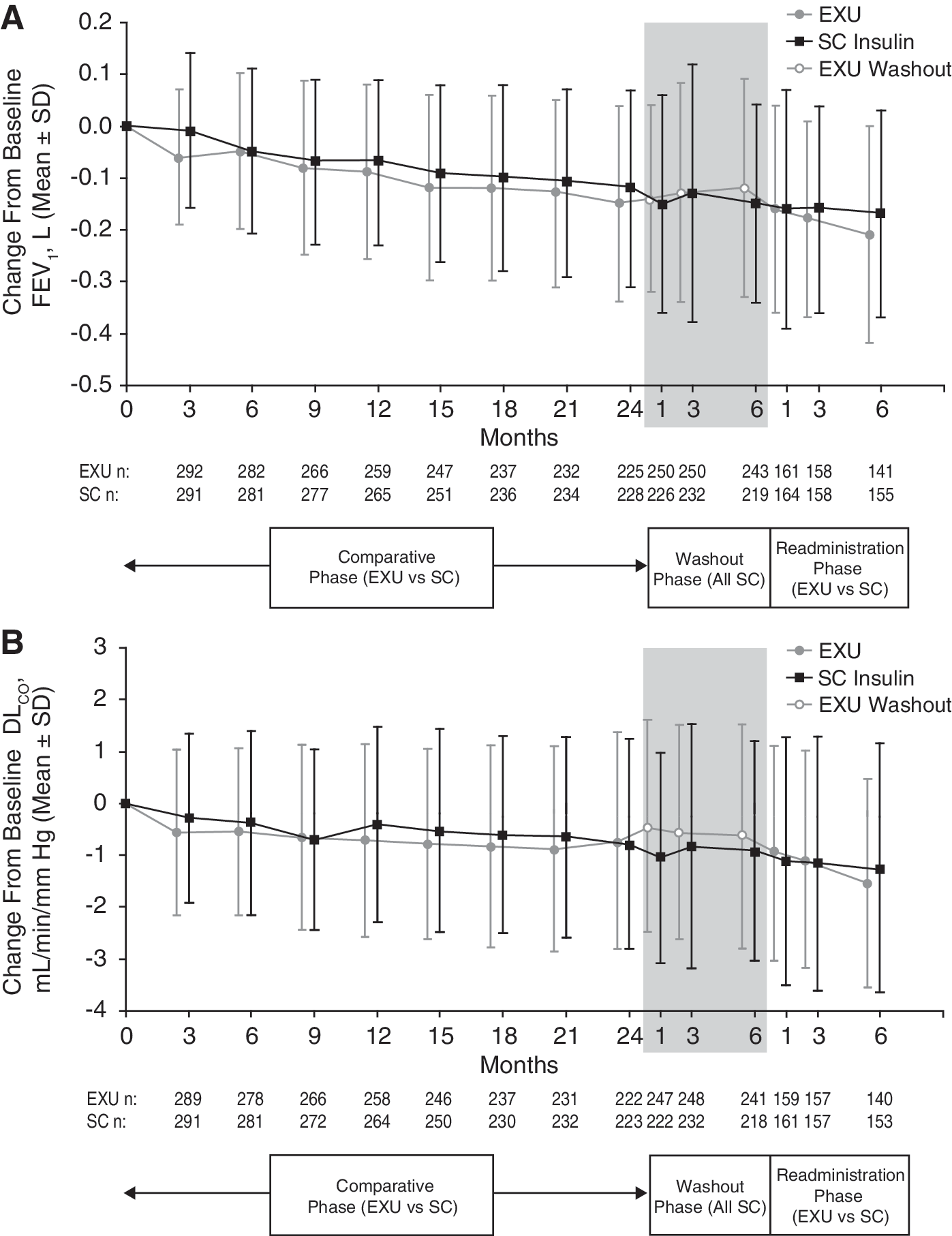
During the comparative treatment phase, FEV1 and DLCO declined from baseline in both treatment groups (Fig. 2A and B). As previously described 7 small treatment group differences in mean change from baseline in FEV1 and DLCO favoring SC insulin were observed during the first 3 months and remained stable thereafter.
Mean (± SD) change from baseline in (
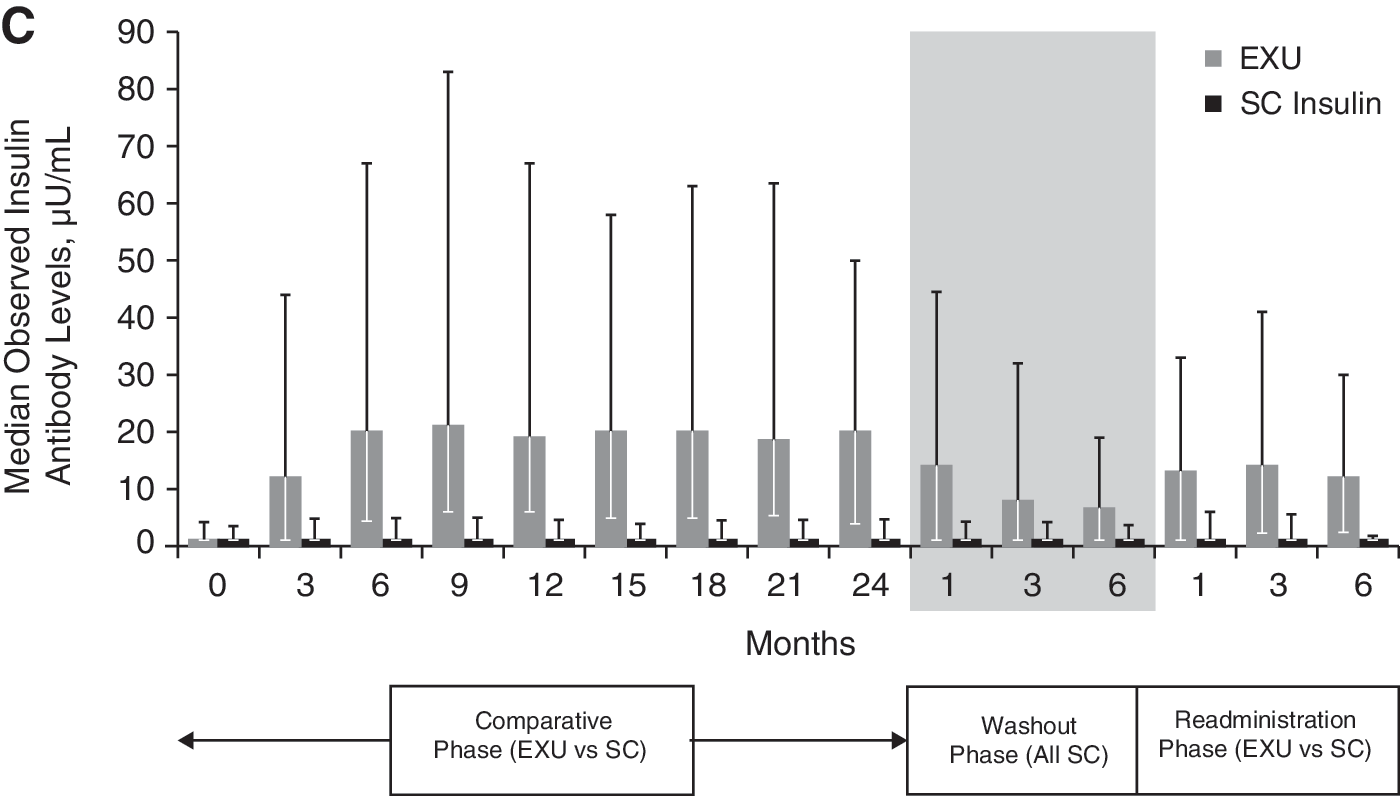
When EXU was discontinued and replaced with SC insulin during the washout phase, treatment group differences in FEV1 and DLCO resolved completely within 1 month (Fig. 2A and B). When EXU was readministered for 6 months following the washout phase, treatment group differences in FEV1 and DLCO recurred to the same small levels as observed in the comparative phase. Treatment group difference in FEV1 was 0.012 (90% CI, −0.017, 0.041) at month 1 of the washout phase and −0.045 (90% CI, −0.083, −0.006) at month 6 of the readministration phase. Treatment group difference in DLCO was 0.648 (90% CI, 0.353, 0.943) at month 1 of the washout phase and −0.277 (90% CI, −0.671, 0.117) at month 6 of the readministration phase.
Discontinuations from study did not have a significant impact on either FEV1 or DLCO. Analyses from a last-observation-carried-forward approach done at month 24 of the comparative phase and month 6 of the readministration phase showed results that were no worse (and in fact slightly better) than the corresponding completers analysis. Also, the decrease in pulmonary function observed with the EXU group at month 6 of the readministration phase was not driven by large decreases in a few outlier patients (Fig. 3). Similar results were observed throughout the comparative and readministration phases.
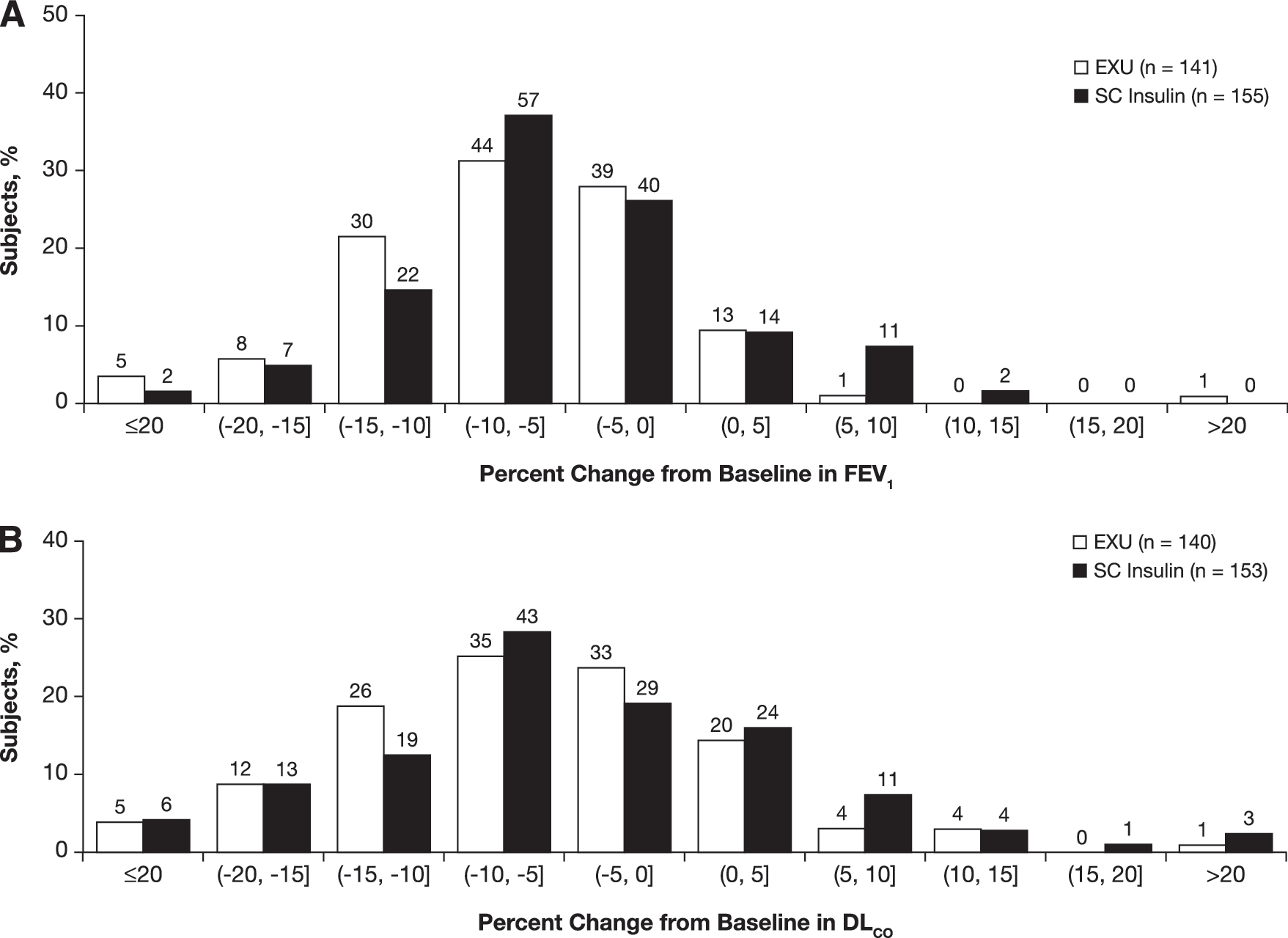
Distribution of percentage change from baseline in (
Discontinuations and adverse events
EXU was generally well tolerated throughout the study. There were 104 discontinuations (32.9%) in the EXU treatment group and 82 discontinuations (26.4%) in the SC insulin treatment group during the comparative and readministration phases. Of these discontinuations, 25 (7.9%) and four (1.3%) were related to study drug in the EXU and SC insulin groups, respectively. Nine of the drug-related discontinuations in the EXU group and three in the SC insulin group were due to lack of efficacy. The other drug-related discontinuation in the SC insulin group was for a laboratory abnormality. There were 16 discontinuations in the EXU group due to drug-related adverse events: decreased pulmonary function, two; asthma exacerbation, two; cough, four; bronchospasm/wheezing, three; other, three; weight gain, one; mouth papillomas, one.
Adverse event profiles were similar between treatment groups. The pattern of adverse events after readministration of EXU therapy was similar to the pattern seen during the original comparative phase. 7 As previously reported, 7 the incidence of cough was highest during the first 3 months of comparative treatment in the EXU group and decreased subsequently. Cough tended to occur within seconds to minutes after insulin inhalation, was predominantly mild in severity, and rarely productive.
After readministration, EXU-treated patients exhibited more cough, dyspnea, and increased sputum than SC insulin-treated patients, consistent with the original comparative phase. Most dyspnea episodes were mild, did not result in discontinuation, and did not worsen with ongoing treatment. The incidence of respiratory tract infections was similar in both groups.
Median observed IAb levels were similar at baseline in the two treatment groups (Fig. 2C). During the comparative phase, median IAb levels increased in the EXU group but not in the SC insulin group. Levels peaked at 9 months and declined thereafter. During the washout phase, IAb levels decreased to near baseline levels in the EXU group; following EXU readministration, median IAb levels increased to levels similar to those observed in the original comparative phase. IAb levels did not correlate with A1C, FPG, hypoglycemia, insulin dose, or changes in FEV1 at the end of either the comparative or readministration phases.
Efficacy
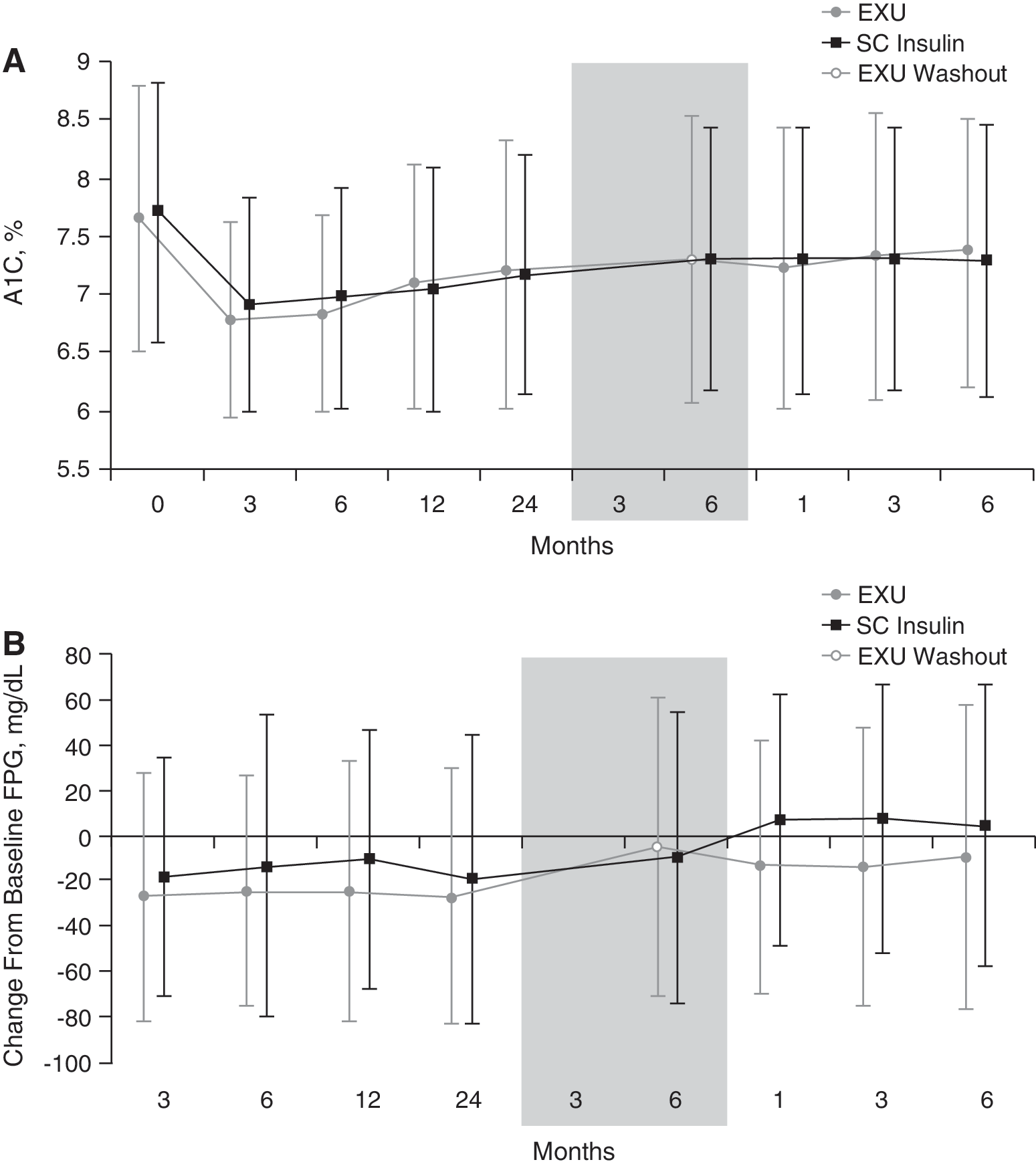
Glycemic control (A1C) was similarly maintained in both treatment groups throughout the three phases (Fig. 4A). Improvements from baseline in A1C were comparable between the two treatment groups at the end of the readministration period; adjusted mean treatment difference (EXU − SC insulin) was 0.05% (90% CI, −0.09, 0.19). Decreases in FPG were consistently greater with EXU compared with SC insulin throughout the comparative phase (Fig. 4B). Mean FPG levels increased when EXU was discontinued but decreased again when EXU was readministered.
Observed mean (± SD) values for (
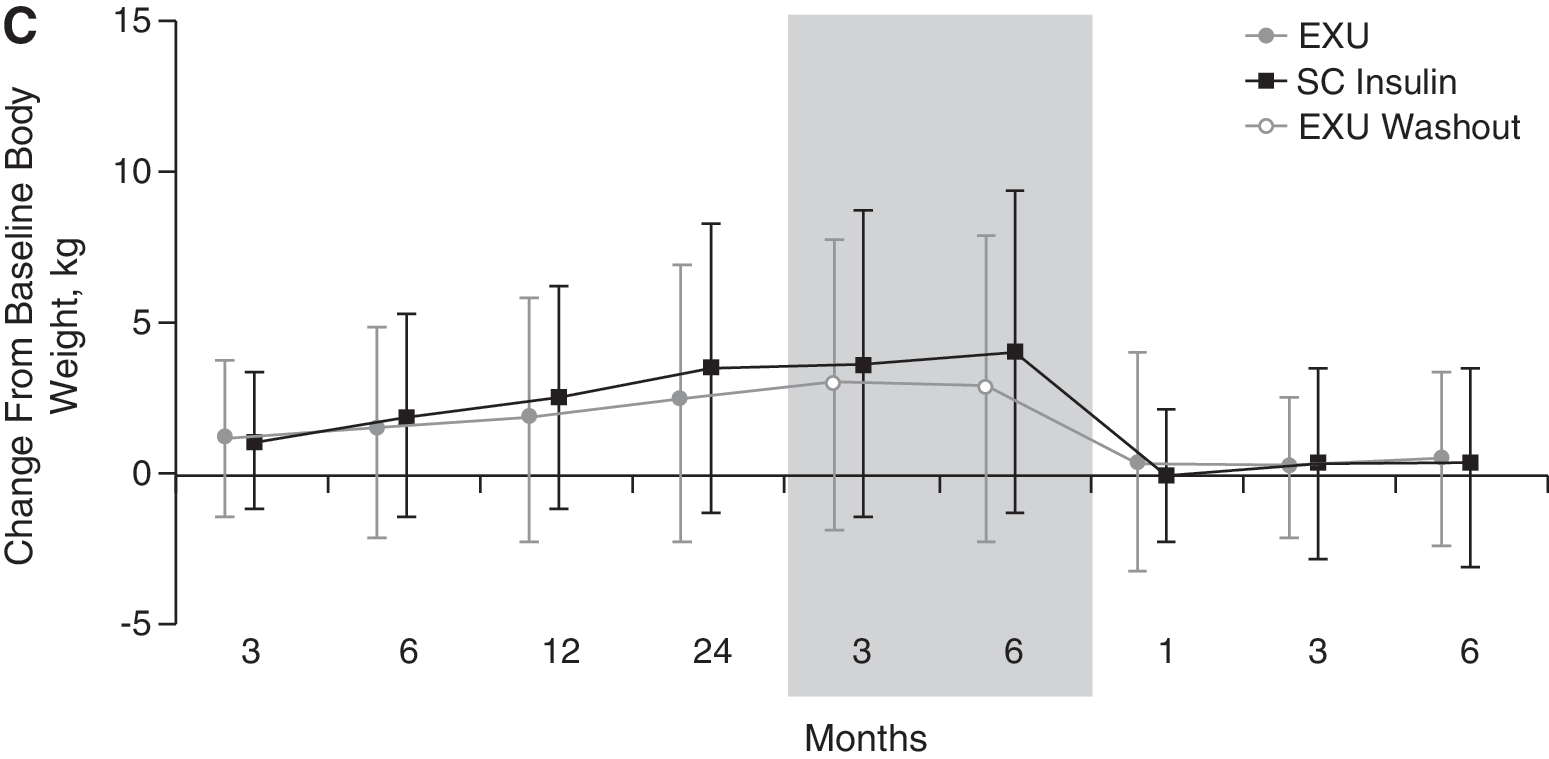
Less weight gain was reported with EXU versus SC insulin during the comparative phase (Fig. 4C). This difference was maintained throughout the washout phase but was lost by month 1 of the readministration phase.
Throughout the study, overall hypoglycemic event rates were comparable in the EXU and SC insulin treatment groups (1.0 and 1.4 events/subject-month, respectively, during the comparative phase and 1.9 events/subject-month for each group during the readministration phase). Of EXU-treated and SC insulin-treated patients, 29.7% and 42.6%, respectively, reported hypoglycemia during the readministration phase. The event rate of severe hypoglycemia was lower in the EXU group compared with the SC insulin group throughout the comparative phase (0.3 and 0.7 events/100 subject-months, respectively). Severe hypoglycemia was reported by 5.8% and 9.5% of patients in the EXU and SC insulin groups, respectively. During the readministration phase, the rate of severe hypoglycemic events was 1.8 events/100 subject-months, for both EXU and SC insulin. Severe hypoglycemia was reported by 1.2% of EXU-treated and 3.6% of SC insulin-treated patients during this time.
Of the 169 patients in the SC insulin group during the readministration phase, 33.7% used regular insulin, and 66.3% used either insulin lispro or insulin aspart as their short-acting insulin. Of those taking regular insulin, 86.0% were also taking NPH/ultralente, whereas 14.0% were taking insulin glargine. Of those taking insulin analogs, 51.8% were also taking NPH/ultralente, whereas 48.2% were taking insulin glargine. The overall hypoglycemic event rate was 2.0 events/subject-month for the regular insulin group and 2.3 events/subject-month for the insulin analog group, with hypoglycemia reported by 33.3% and 47.3% of patients, respectively. Severe hypoglycemic event rates were 2.8 and 4.4 events/100 subject-months, with severe hypoglycemia reported by 5.3% and 2.7% of patients, respectively.
Discussion
This study evaluated safety and efficacy for EXU treatment over a long-term period of observation and the impact of discontinuation and readmistration of the inhaled insulin. Although both treatment groups maintained similar glycemic control and hypoglycemic event rates, small, nonprogressive treatment group differences occured early during the comparative phase for parameters such as change from baseline for FEV1 and DLCO. These differences were noted to resolve during washout of inhaled insulin but recurred to the same magnitude during readministration. Similar results recently were obtained in a study of patients with type 1 diabetes. 18 Although the mechanisms of the lung function changes are currently unknown, this pattern of change is consistent with a physiologic, nonstructurally pathologic, effect of EXU therapy and suggests that irreversible lung injury did not occur during 2 years of continuous EXU therapy.
Consistent with the influence of age, lung function declined in both the EXU and SC treatment groups over the course of the comparative phase. FEV1 and DLCO have been observed to decline by about 1–2% and 1.3% per year, respectively, in male and female nonsmokers without diabetes. 11,19 The rate of decline may be increased in some patients with diabetes, 20,21 and histopathological changes have been reported in lungs from subjects with diabetes. 22,23 Further studies are warranted to clarify the relationship of lung function to the development of diabetes and to assess whether diabetes-related pulmonary dysfunction is potentially reversible following the re-establishment of normoglycemia.
Consistent with other randomized clinical trials, 1 –7 EXU was as effective as SC insulin at improving glycemic control. In contrast, EXU caused a greater reduction in FPG than SC insulin—a result that also is consistent with previous studies. 6,7,18 When EXU treatment was discontinued, the beneficial effects on FPG were lost, but they recurred to the same small magnitude following EXU readministration. The reasons for the beneficial effects of EXU treatment on FPG are not completely clear, but studies suggest that insulin inhalation results in a unique action on glucose clearance. 24 –26
The overall hypoglycemic event rates were comparable in the EXU and SC insulin treatment groups throughout the study. The event rate of severe hypoglycemia was lower in the EXU group compared with the SC insulin group throughout the comparative phase, but similar during the readministration phase. In addition, the pattern of adverse events after readministration of EXU therapy was similar to that seen during the original comparative phase. 7 EXU-treated patients exhibited more cough, dyspnea, and increased sputum than SC insulin-treated patients. Cough tended to occur within minutes after inhalation, was usually mild in severity, and was seldom productive; the majority of dyspnea episodes were mild, did not result in discontinuation, and did not worsen with ongoing treatment.
Weight gain is a common concern for patients during insulin therapy. In previous studies, EXU treatment was associated with significantly less weight gain than SC insulin. 27 As this study confirms prior findings that inhaled insulin attenuated weight gain in patients with diabetes, it suggests that this therapy may alter energy balance, e.g., dietary intake and/or energy expenditure, in some way or perhaps may be a reflection of less hypoglycemia and reduced “defense snacking.” However, the mechanisms for the attenuation in weight gain are not precisely known at this time. Results from this study demonstrated that the difference in weight can be maintained for 6 months following cessation of EXU therapy.
Previous studies, including a large meta-analysis of several phase 2/3 studies, have shown that IAb levels are higher after EXU than comparator treatment. 28 In the present study, IAb levels declined following discontinuation of EXU therapy, and subsequent readministration of EXU resulted in an IAb response comparable to that seen after the original initiation of EXU treatment. No clinical consequences of elevated IAb levels have been identified to date; IAbs are not related to insulin dose and do not impact insulin pharmacodynamics, glucose control, hypoglycemia, or lung function. 29,30 An anamnestic response was not seen after EXU readministration. 31
In summary, pulmonary function changes that occur in adults with T2DM following EXU treatment were consistent with a reversible, nonprogressive, and nonpathologic effect on lung function. EXU readministration was well tolerated, with a similar incidence of hypoglycemia to SC insulin treatment. EXU readminstration was not associated with an augmented IAb response.
Footnotes
Acknowledgments
These studies were sponsored by Pfizer Inc. Editorial support was provided by Ellie Ling, Ph.D. and Tom Claus, Ph.D., of PAREXEL and was funded by Pfizer Inc. Additional programming support was provided by Sharad Chhetri of Eliassen Group. We would like to thank all the patients, investigators, and coordinators who took part in this study.
Author Disclosure Statement
J.R., W.T.C., and P.A.H. have received grant support for clinical research and honorarium for having served on Pfizer Scientific Advisory Boards. S.S.K., J.R., and W.T.D. are employees of Pfizer Inc.
Addendum
On October 18, 2007, Pfizer Inc. announced that it would cease marketing Exubera because it did not meet customers' needs or financial expectations.
On April 9, 2008, Pfizer Inc announced that it was updating the Exubera product insert to include the following statement: “In studies of Exubera in people with diabetes, lung cancer occurred in a few more people who were taking Exubera than in people who were taking other diabetes medicines. All of the people in these studies who developed lung cancer used to smoke cigarettes. There were too few cases to know if the lung cancer was related to Exubera.”
This study is registered at