
Abstract
Background:
Hypertension is a major risk factor for the long-term complications of diabetes. Mobile, self-measurement of blood pressure is emerging as a method to manage blood pressure in general, but its impact in patients with diabetes is unclear.
Methods:
We randomized 137 patients with diabetes and hypertension to either mobile telemonitoring (n = 72) or usual care (n = 65). Clinic blood pressure was recorded at baseline and after 6 months. Patients in the intervention arm transmitted weekly blood pressure readings wirelessly, using adapted sensors via mobile phones to a central server. Clinicians received the data in real-time and using a web-based application provided management advice to the patient and their physicians.
Results:
Systolic blood pressure fell significantly in the patients in the intervention group (mean [95% confidence interval], −6.5 [−0.8 to −12.2] mm Hg; P = 0.027) and remained unchanged in the control group (2.1 [9.3 to −5.0] mm Hg; P = 0.57). Patients within the intervention arm of African origin seemed to benefit more from the intervention. In addition, those who achieved a systolic blood pressure of <120 mm Hg had lower average blood sugars than those with higher readings (7.8 [SD 1.6] vs. 8.9 [SD 2.2] mmol/L; P = 0.02).
Conclusions:
In patients with diabetes, mobile telemonitoring has potential for delivering intensified care to improve blood pressure control, and its use may be associated with reduced exposure to hyperglycemia.
Introduction
The remote monitoring of patients is considered an important tool in facilitating improvements in chronic disease management. A systematic review has confirmed the feasibility of this approach, although questions remain regarding its efficacy on diabetes control, and the impact on the intensification of blood pressure management is unknown. 5 Mobile health (m-Health) is an emerging concept of “connected health care” anytime and anywhere through wireless communications. 6 It is an evolution from traditional desktop telemedicine to wireless platforms that has the potential to improve chronic disease management. 7 Here we present the outcomes of a pilot study in which m-Health was compared with usual care in the management of hypertension in a sample of patients with diabetes from an inner-city population of the United Kingdom.
Patients and Methods
The study was based at the Thomas Addison Unit, St. George's Hospital, South London, UK, which serves an inner-city population characterized by a diverse ethnic mix—22% of residents belong to a non-white minority ethnic group—with a social deprivation score that is higher than the national average (see
We audited our population of patients with diabetes from the registers of general practices to establish the demography of our local population. Recruitment took place between December 2006 and July 2007 as previously described. 8 Ambulant patients >18 years of age with a known diagnosis of diabetes who were receiving pharmacological therapy for hypertension or who had an untreated sitting systolic (SBP) and/or diastolic (DBP) blood pressure of ≥130 and/or ≥80 mm Hg were eligible for inclusion. Exclusion criteria were a physical inability to self-monitor blood glucose or blood pressure, pregnancy, severe life-threatening or terminal illness, and inability to provide written informed consent.
A standardized diabetes data set was collected for each patient on proformas and transferred to an electronic database for later evaluation. Diabetic retinopathy was screened for using digital fundal photography after pupil dilatation and recorded as present (background, preproliferative, or proliferative) or absent.
Venous blood was taken from an antecubital vein after an overnight fast. Hemoglobin A1c (HbA1c) was measured by high-performance liquid chromatography (model 8140 chromatograph, Menarini, High Wycombe, UK). Total and high-density lipoprotein (HDL)-cholesterol and total triglycerides were estimated using enzymatic methods (Boehringer-Mannheim, Mannheim, Germany). The low-density lipoprotein (LDL)-cholesterol concentration was calculated using the Friedewald formula: LDL-cholesterol = Total cholesterol − (Triglyceride [in mmol/L]/2.19) − HDL-cholesterol (in mmol/L). Urinary albumin and creatinine were measured by immunoturbidimetry (Cobas Fara, Roche, Basel, Switzerland) and the Jaffe rate reaction methods, respectively.
Baseline blood pressure was measured in all patients according to British Society of Hypertension guidelines by the research nurse. In brief, after a 10-min rest, sitting blood pressure was taken using a digital monitor (model UA-767BT, A&D Medical, San Jose, CA) in the non-dominant arm with an appropriately sized cuff positioned at heart level on three occasions. The mean of the last two measurements were recorded as the study blood pressure. Patients were randomized to the m-Health group (MH group) or usual care group (UC group) according to a computer-generated random number sequence (Stat Mate™ version 1.01i, GraphPad, San Diego, CA).
m-Health monitoring
The basic architecture and technical details of the m-Health system for capturing measurements of blood glucose and blood pressure are described elsewhere. 8
The connection between mobile phone and sensor was made with a wireless Bluetooth® (Bluetooth Special Interest Group, Bellevue, WA) connection. The communication technology used to transmit the patient data was a General Packet Radio Service system (3G) with connectivity for accessing the server with secure encoded links to the internet.
Patients in the intervention arm were trained to measure their own blood pressure and transmit the recordings via Bluetooth wireless technology to a 3G mobile phone (model A-100, Motorola, Plantation, FL) once a week. Capillary blood glucose tests (OneTouch® Ultra® glucose meter, Lifescan, Milpitas, CA) were also requested between four and nine times per week and transmitted as previously described. 8
The mobile phones were configured to show the accumulated or individual measurements. These data were sent wirelessly over the internet to a web-based application (Motohealth™, Motorola) for review by clinicians. Recommendations to alter treatment were based on trends in the amalgamated readings and provided to patients and their general practitioner by letter. The patients were able to use the phones without incurring charges to contact the research nurses.
Control patients
Those allocated to the UC group did not receive any m-Health equipment. They were not required to report their blood pressure and did not receive any support from the research nurses. All of their management was provided by their local practitioners who were not involved in the study. At the end of follow-up, the patients were reviewed by the research nurse for an assessment for their clinic blood pressure.
The study was approved by the Wandsworth Ethics Committee (London).
Statistics
Based on our previous intervention studies, 9 we aimed to recruit 60 patients in each group in anticipation of a 10–20% dropout over 6 months. This strategy meant the study would have at least 80% power to detect a 7 mm Hg difference in SBP after 6 months (Stat Mate version 1.01i). The data were analyzed on an intention-to-treat basis with imputation of outcomes by carrying over the last known status of the variable for patients defaulting or lost to follow-up.
Analyses between or within the groups were performed using SPSS version 16.0 for Windows (SPSS, Inc., Chicago, IL). Continuous variables were compared using parametric or nonparametric tests, and associations were tested with Spearman's rank or Pearson's test according to their distribution. Categorical variables were compared using the χ 2 test with continuity correction or Fisher's exact test. Data are expressed as mean (SD) values unless otherwise stated.
Results
In our district-wide audit we found that 4,569 (54% male) patients with diabetes were registered in 26 practices in South Wandsworth, London. Ten percent had a diagnosis of type 1 diabetes, the mean age was 61 years, and the proportion of white (Caucasian), black (African and or Caribbean), or Indo-Asian (Indian, Pakistan, or Bangladeshi) heritage was 41%, 23%, and 35%, respectively.
Practices in our catchment area and the surrounding district provided the research team with permission to send invite letters to their patients. Many of these patients also received some of their care at the diabetes center. Therefore, the team approached consecutive attendees and undertook the initial review of those who responded positively to the letters of invite as previously described. 8
We randomized 137 patients to the MH intervention (n = 72) and UC (n = 65) control groups. The groups were well matched according to their demographic characteristics and baseline blood pressure, diabetes control determined by the HbA1c, renal function, and lipid profile (Table 1). Twenty-six patients defaulted in the MH group compared with 16 from the control group at 6 months. In each group, 29 patients had a record of diabetic retinopathy. Five percent were treated with diet alone, compared with 25% with insulin alone as the main management modality for diabetes. A greater proportion of patients was treated with combined insulin and oral hypoglycemic agents in the MH intervention than the UC control group, although this did not reach conventional statistical significance (22% vs. 11%; P = 0.27). The frequency of treated hypertension was 69% and 66% in the MH and UC groups, respectively.
DBP, diastolic blood pressure; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; LDL, low-density lipoprotein; MH group, mobile health group; SBP, systolic blood pressure; UC group, usual care group.
A total of 1,721 blood pressure and 4,099 blood glucose readings were made. The transmission rate of blood pressure recordings (4.0 [3.8]/person/month) was consistent with the protocol, whereas that for blood glucose (1.8 [1.1]/person/week) was significantly less than expected (P = 0.0001).
Patients whose averaged home SBP was <120 mm Hg also had significantly lower average capillary blood sugars (7.8 [1.6] vs. 8.9 [2.2] mmol/L; P = 0.02). As previously reported, HbA1c in the patients from the intervention group was 0.64% lower than in the control group, but this difference did not reach statistical significance. 8
SBP declined significantly in the patients in the MH intervention group but not in the UC control group in those completing the study (Fig. 1). The intention-to-treat analysis showed a significant drop in SBP of −2.9 [0.6 to −5.1] mm Hg (mean [95% confidence interval]; P = 0.013) in the MH group.
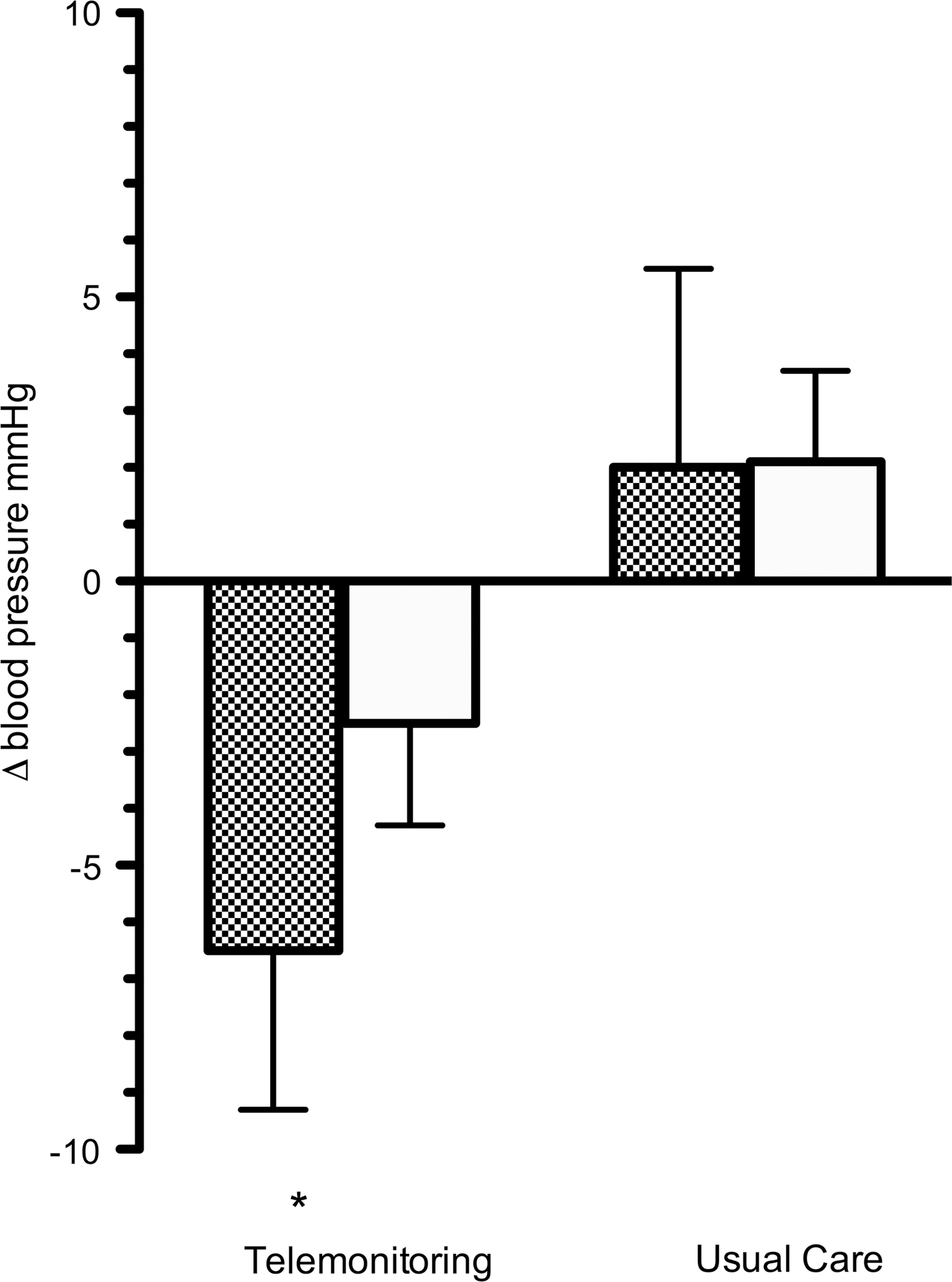
Changes in systolic (shaded bars) and diastolic (open bars) blood pressure of patients at the end of the study in the telemonitoring and usual care groups. *The fall in systolic blood pressure in the telemonitoring group was significant at P < 0.05.
Within the intervention arm, blood pressure averaged over the follow-up period was higher in patients of African origin compared with the Caucasian group (125.3 [12.6] vs. 116.8 [11.7] mm Hg; P = 0.04). The decrement in blood pressure was significant only in the group of patients of African origin using m-Health and was unchanged in all ethnic subgroups receiving usual care (Fig. 2). There were no significant changes in DBP, HbA1c, or cholesterol profile in either treatment group.
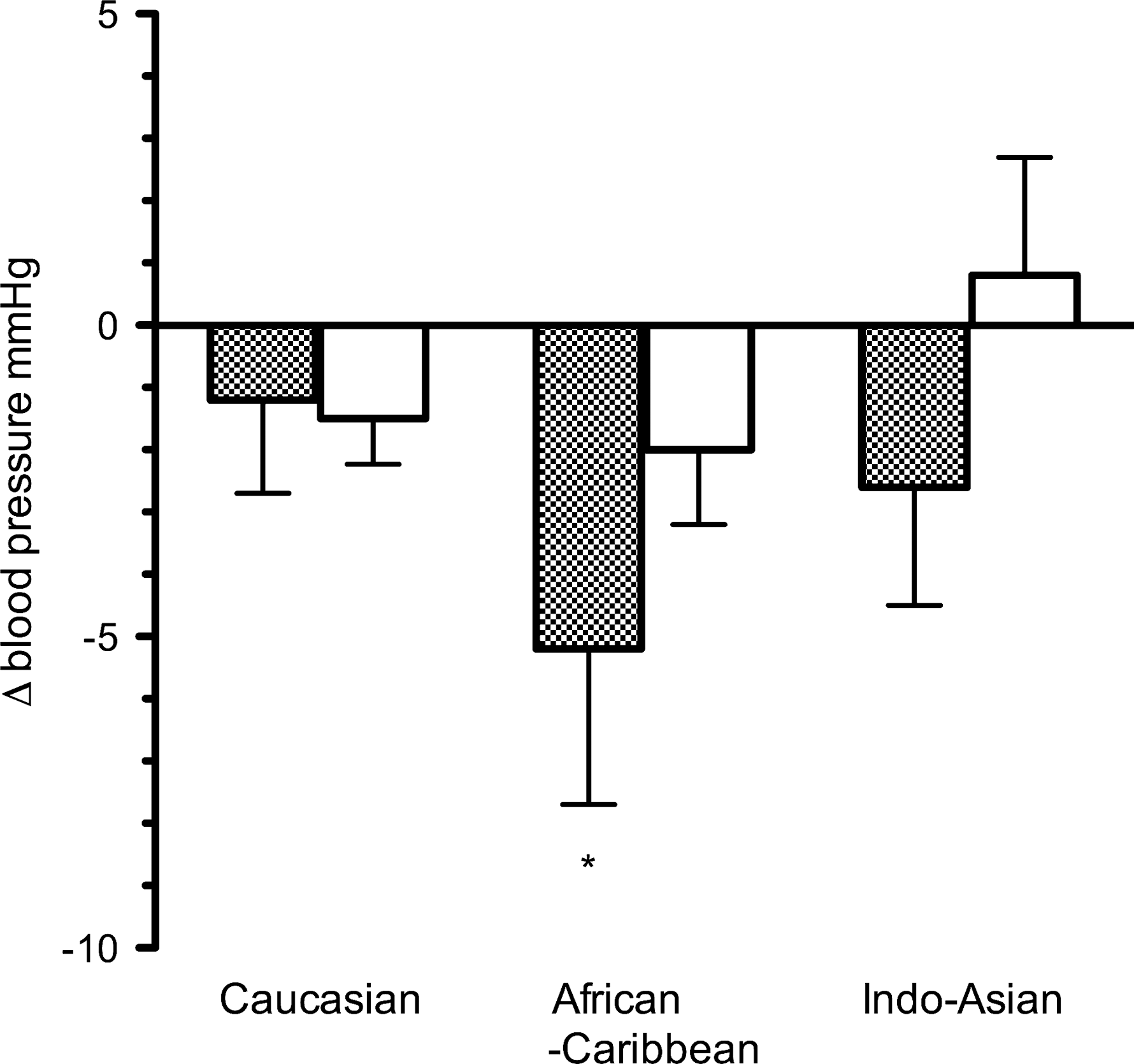
Changes in systolic (shaded bars) and diastolic (open bars) blood pressure from baseline of patients in the telemonitoring group at the end of the study according to racial heritage. *The change in systolic blood pressure in the African-Caribbean group was significant at P < 0.05.
Discussion
This study has shown that remote mobile telemonitoring is feasible as a method to intensify management of blood pressure in patients with established diabetes, hypertension, and microvascular complications. This protocol may be particularly pertinent in groups at high risk of renal and vascular events and may be associated with reduced exposure to hyperglycemia in the short term.
Previous studies trialling this technology have been in select, usually young, uncomplicated patient groups with type 1 diabetes. This study is one of the first reports to demonstrate the application of mobile technology in a representative sample of a general, inner-city diabetes population. In this cohort, one in three patients had microvascular disease, and two in three were of non-Caucasian heritage—features that are associated with “resistant hypertension” and relatively poorer outcomes. 10
In the 2006 Health Survey of England report, less than one in two of the 380 patients with diabetes treated for hypertension were controlled to <140/90 mm Hg. 11 Analyses of the United Kingdom Prospective Diabetes Study (UKPDS) data suggest that the risk of developing microvascular complications is lowest below an SBP threshold of 120 mm Hg. 4 This study also reported that blood pressure control was more efficacious than blood glucose control in reducing microvascular disease risk. 12 The risk for any diabetes complication or death in patients may be reduced by 12% for a 10 mm Hg reduction of SBP. 4 Blood pressure regulation is central to policies for targeted intervention in patients with type 2 diabetes that have been shown to reduce the risk of cardiovascular events by up to 50%. 13,14
Observational data suggest that the relationship between blood pressure and renal events extends below the current treatment threshold of 130–125 mm Hg SBP and 80–75 mm Hg DBP recommended for patients with diabetes. 15,16 Moreover, the Action in Diabetes and Vascular disease: preterAx and diamicroN-MR Controlled Evaluation (ADVANCE) intervention trial showed that patients with diabetes received protection from renal events with an achieved SBP as low as 110 mm Hg. 17
This study suggests that technologies such as m-Health could be part of the solution to help patients achieve and maintain blood pressure below the current recommended target. There were no differences in the change in treatments from baseline to final measurement in the intervention group, suggesting that the m-Health protocol per se was instrumental in improving blood pressure. The potential benefit of this approach to patients of African origin in this study is noteworthy. However, this was a small group who had higher baseline blood pressures than the other heritage groups. The study was not designed to determine whether the reasons for the improvement were related to increased accessibility to monitoring and specialist advice or inducement of changes in self-management and improved treatment compliance.
Improvements in health-related behaviors have been previously reported in association with home blood pressure monitoring. 18,19 In our study, patients who had better blood pressure control also had lower average blood sugars. This observation was not related to the number of transmissions, and we consider that this may be a reflection of better overall compliance with treatment and action on recommendations rather than habituation.
The lack of a “legacy” effect with conventional intensification methods for blood pressure control in patients with diabetes is of concern to health providers. 20 That is, discontinuation of intensification regimens for blood pressure is associated with a loss of benefit. Therefore technologies that have short-term benefit need to be shown to have long-term usefulness. The default rate in the control arm was not atypical of this population in the “real world” of diabetes care. However, the higher than expected default rate in the intervention arm was largely the result of technological problems with the use of the hardware and the patient's ability to transmit data. In particular, patients reported unreliability of the equipment and that the troubleshooting support systems were not intuitive. Others have shown that in selected patients without diabetes, home blood pressure monitoring with web-based feedback does not result in significant lowering of blood pressure compared with usual care unless this was combined with personal, professional healthcare input. 21,22
Our work suggests that the m-Health approach to managing blood pressure has potential benefits in patients with complicated diabetes. A similar but more patient-focused system has achieved similar results, strengthening the suggested potential role for mobile phone blood pressure monitoring. 23 Intelligent and intuitive system design is a key issue to limit high dropout rates for the monitoring of vascular disorders. 24,25 Further quantitative and qualitative analyses will be insightful in understanding the attitudes, compliance with, and future and longer-term use of this developing technology by the patient with diabetes.
Footnotes
Acknowledgments
The authors would like to acknowledge the financial and technical support from the IDEN Group, Motorola Inc., USA and the Motohealth team in the United Kingdom. We thank Mr. Jose Lacal, Sir David Brown, and Prof. David Oliviera for their support of this project. This study was funded by Motorola Inc., USA.
Author Disclosure Statement
The institutions of the principal investigators, K.A.E. and R.S.H.I., received funding from Motorola Inc., USA for part of the salaries of K.Z., A.S., and B.T. to conduct this study.
This study is registered with