
Abstract
Background:
We designed a system for diabetes patients treated with glargine, a long-acting insulin, to make an automatic adjustment of insulin dose based on glucose level data and to provide the patients with the needed insulin dose by using a short message service (SMS). We also compared diabetes patients who used our system with patients who received the conventional titration scheme.
Methods:
Included were 100 type 2 diabetes patients whose blood glucose was suboptimally controlled on their previous antidiabetes treatment. Each participant was assigned to either the intervention or control group, each with 50 patients, using adaptive randomization. We applied our system to the intervention group for 12 weeks, whereas the control group received a conventional titration scheme, seeking a target fasting blood glucose of <120 mg/dL.
Results:
The fasting and postprandial glucose levels of the intervention group declined earlier than those of the control group. Lastly, a greater (P = 0.023) reduction in hemoglobin A1C from baseline to the end point was observed in the intervention group (from 9.8 ± 1.3% to 7.4 ± 0.7%) than in the control group (from 9.8 ± 1.2% to 7.8 ± 0.8%). The incidence of symptomatic, asymptomatic, and nocturnal hypoglycemia was similar in both groups. There was a small increase in body weight from baseline to the end point with both the intervention (2.4 ± 3.0 kg) and control (2.2 ± 2.8 kg) groups.
Conclusions:
This study demonstrated that SMS based on our specialized Internet-supported system is an effective and safe approach to long-acting insulin dose adjustments in patients with type 2 diabetes.
Introduction
In the management of diabetes, it is important to maintain an intimate and continuous doctor–patient relationship. To achieve an optimal glucose level and to prevent complications of diabetes, frequent contact with a medical doctor is recommended, but this causes an increased amount of medical expense. In recent years, web and phone deliveries of self-management programs have emerged as popular approaches to the management of diabetes. 4 –6 The major focus of the system was support for blood glucose monitoring with substantive feedback from an expert to help interpret results of glucose level values. 7 Moreover, with this system, the patients could be advised to determine the amount of insulin required. 8 However, despite the use of these programs, it can take a significant amount of effort and time for physicians to look over each patient's data, formulate an appropriate message, and send it to that patient. Accordingly, computerized, knowledge-based medical treatment advice systems will provide more abundant medical advice 9 and can be more economical than the previous systems, in which medical personnel were required for the same process.
Recently we designed an Internet-based diabetes patient management using short message service (SMS) that was automatically produced by a knowledge matrix. Moreover, we reported this unique system has shown the great efficacy in glucose control. 10 In this study, we designed the system for patients treated with glargine, a long-acting insulin, to make an automatic adjustment of insulin dose based on glucose level data and to provide the patients with the needed insulin dose by using an SMS.
Patients and Methods
Subjects
Patients with type 2 diabetes whose blood glucose was suboptimally controlled on their previous antidiabetes treatment were targeted. Inclusion criteria included age ≥18 years, taking antidiabetes treatment (any oral and/or insulin therapy) for >6 months, requiring a long-acting insulin therapy for the control of hyperglycemia in the opinion of the investigating physician, hemoglobin A1C (HbA1C) levels >7.0% and <12.0%, body mass index values <35 kg/m2, and confirmed written informed consent.
Hypertension was defined as a systolic blood pressure at least 130 mm Hg and/or a diastolic blood pressure at least 80 mm Hg, the presence of antihypertensive drug treatment, or a combination of these. Hypercholesterolemia was defined as a total cholesterol level ≥220 mg/dL, the use of lipid-lowering drugs, or both. We defined nephropathy for this study as an albumin excretion rate of ≥30 mg/24-h period in two or more of these three exams. Retinopathy was defined by at least one retinal microaneurysm with or without hemorrhages, venous beading, soft exudates, or intraretinal microvascular abnormalities. Neuropathy was defined as the presence of delay in nerve conduction and/or abnormal finding in current perception threshold and/or diminished heart rate variation and/or absent tendon reflexes and/or neuropathic symptoms.
Exclusion criteria were as follows: type 1 diabetes, renal dysfunction (defined as serum creatinine level >2.0 mg/dL), hepatic dysfunction (defined as alanine aminotransferase and/or aspartate aminotransferase blood level >2.5 times the upper normal limit), hypoglycemic unawareness, pregnancy, severe retinopathy, illiteracy, and elderly over 70 years. Other exclusion criteria were in accordance with the manufacturers' prescribing information. The protocol was approved by the Ethics Committee of the Hallym University Sacred Heart Hospital, Anyang, Republic of Korea. Written informed consent was obtained from each participant.
A knowledge matrix development
We developed the system to produce an automatic adjustment of insulin dose based on the mean fasting glucose level for 3 consecutive days. Moreover, with the technical assistance from UBCare (Seoul, Republic of Korea), we created a website program (
According to the mean fasting blood glucose (FBG) level for 3 consecutive days ≥180 mg/dL, 140–179 mg/dL, and 120–139 mg/dL, patients were asked to increase the daily glargine dose by 6 units, 4 units, and 2 units, respectively. If the mean FBG level for 3 consecutive days was between 80 and 119 mg/dL, patients were asked to maintain the current dose. In addition, the insulin dose was decreased by 2 units for a blood glucose level between 60 and 79 mg/dL and 4 units for a glucose level below 60 mg/dL. If daily FBG was not measured, the insulin dose was adjusted based on the mean FBG level of the latest 3 days.
For the prevention of hypoglycemia, if patients showed decreasing glucose levels for 3 consecutive days, the insulin dose was adjusted based on the last glucose level measured. If one glucose level was higher than 60 mg/dL compared with other two levels measured within 3 consecutive days, the mean glucose level of the other two was used for insulin dose adjustment.
In addition to the insulin dose adjustment function, if patients did not measure glucose three times within a week, an information message was sent to patients automatically. Also, if any hypoglycemia was documented, an emergency SMS was delivered to the patient and any caregiver designated by that patient.
Study protocol and treatment
One hundred type 2 diabetes patients treated with any antidiabetes agents, including insulin, during a period of at least 6 months were recruited from the outpatient clinic of Hallym University Sacred Heart Hospital between May and September 2008.
Insulin glargine was administered once daily at bedtime (9 p.m. until 12 a.m.). The starting dose for insulin-naive subjects was 10 U/day or 0.2 U/kg/day. For subjects on oral agents, the investigator decided whether to continue each agent. Dose and regimen of oral agents remained unchanged throughout the study.
Patients being treated with insulin had their previous insulin discontinued at study entry. When switching from once-daily NPH or long-acting insulin to glargine, the same dose was recommended. For patients switched from twice-daily NPH insulin, a reduction of 20–30% in the total NPH insulin dose was recommended. 11 Prandial insulin was not added because the main aim of the study was to optimize basal insulin.
We provided overall orientation to each participant on diabetes management (including how to inject insulin) as well as nutritional and exercise education. It consists of a general overview of the diabetes (endocrinologist, 20 min), exercise control (diabetes nurse, 20 min), nutritional education (diabetes dietitian, 20 min), and insulin therapy (pharmacist, 20 min). This is based on the Korea Staged Diabetes Management Guideline. Each participant was assigned to either intervention or control group, each with 50 patients by a computer-generated allocation sequence using adaptive randomization. 12 Patients in the intervention group were taught how to use our specialized system. They then used this system for 12 weeks. Patients in the control group self-adjusted their basal insulin according to daily self-monitored capillary FBG measurements using glucometers (model GAM-2200, All Medicus Co., Ltd.) that provide values corresponding closely to laboratory measurements of plasma glucose. A forced titration scheme was used, seeking a target FBG of <120 mg/dL. If the mean fasting glucose level for 3 consecutive days was over 120 mg/dL, patients were asked to increase daily glargine dose by 2 units. In addition, insulin dose was decreased by 2 units for FBG between 60 and 80 mg/dL and by 4 units for FBG below 60 mg/dL. Patients' dose adjustments were reviewed by the investigator at 4- and 8-week clinical visits. Subjects were encouraged to check their FBG before breakfast every morning. When patients failed to measure FBG at least three times in 20 days, they were dropped out from the study.
Self-monitoring of blood glucose was done by all the participants. In the intervention group, glucose profiles were reviewed from data recorded on the website, and in the control group, they were from the diabetes notebook and glucometer.
We measured anthropometric data, blood pressure, and biochemical profiles of the participants after 8 h of fasting at the start of the study and at 12 weeks. In addition, all subjects visited the outpatient clinic at 4 and 8 weeks and underwent the following: laboratory test for fasting and 2-h postprandial glucose, review of glucose level data recorded by patients, and evaluation of hypoglycemia and adverse events.
Statistical analysis
The sample size calculated based on the previous study 5 was sufficient for 80% power and 5% significance level. We assumed a dropout rate of 10% in this study. The primary objective was to compare the mean changes of HbA1C from baseline to end point between the two groups. Secondary objectives included the proportion of patients to achieve HbA1C level below 7.0%, incidence of symptomatic (symptoms of hypoglycemia responding to ingestion of carbohydrate or an episode associated with a blood glucose level <70 mg/dL), nocturnal (hypoglycemia occurring while the subject was asleep and associated with a blood glucose level <70 mg/dL but without symptoms), asymptomatic (associated with a blood glucose level <70 mg/dL), and severe (presence of symptoms consistent with hypoglycemia during which the subject required the assistance of another person and either a glucose level <50 mg/dL or prompt recovery after oral carbohydrate, intravenous glucose, or glucagon) hypoglycemia, change in body weight, and insulin dose. This glucose threshold was chosen because lower levels can induce hypoglycemia unawareness. 13
Descriptive statistics are presented as mean ± SD values. To assess the significant changes of the glycemic control observed within each group between the baseline and follow-up, we used the paired-sample t test. Comparison of the intervention and control groups was based on the independent t test or χ 2 test as appropriate. The significance of difference between the intervention and control groups was evaluated by analysis of covariance, which tested changes between the two groups from the preintervention to postintervention period while controlling the different baseline values on the outcomes of interest. Statistical analyses were conducted using SPSS for Windows, version 11.5 (SPSS Inc., Chicago, IL, USA), and P < 0.05 was set as the level of significance.
Results
Of the 50 patients in the intervention group, two patients were excluded because of the violation of the study protocol, and another patient was excluded because of not visiting our hospital after 12 weeks. Three patients in the control group were excluded for not revisiting our hospital after 12 weeks, and two patients were excluded because of violation of the study protocol. Consequently, we report data from 47 patients in the intervention group and 45 patients in the control group who completed the study protocol.
Subject demographics and baseline characteristics were similar between the two treatment groups (Table 1). The test results from the beginning of the study showed that there were no significant differences between the two groups with respect to age, sex, duration of diabetes, body mass index, blood pressure, HbA1C, FBG, postprandial blood glucose, total cholesterol, triglyceride, high-density lipoprotein-cholesterol, or low-density lipoprotein-cholesterol. Moreover, diagnoses of hypertension, hypercholesterolemia, and diabetes-related complications were equally distributed in both groups. There were no differences in the currently used diabetes-related medications between groups. There was no drug modification in either group during the study period.
Data are mean ± SD values. BMI, body mass index; CAD, coronary artery disease; CVD, cerebrovascular disease; HDL, high-density lipoprotein; LDL, low-density lipoprotein; PAD, peripheral arterial disease.
Overall, there was a significant reduction in HbA1C from 9.8 ± 1.2% to 7.6 ± 0.8% (P < 0.001). A significantly greater (P = 0.023) reduction in HbA1C from baseline to end point was observed in the intervention group (9.8 ± 1.3% to 7.4 ± 0.7%) than in the control group (9.8 ± 1.2% to 7.8 ± 0.8%). At end point, 25.5% of subjects in the intervention group reached the target HbA1C level of <7% compared with 15.6% of subjects in the control group, with no significant difference between the groups (P = 0.235).
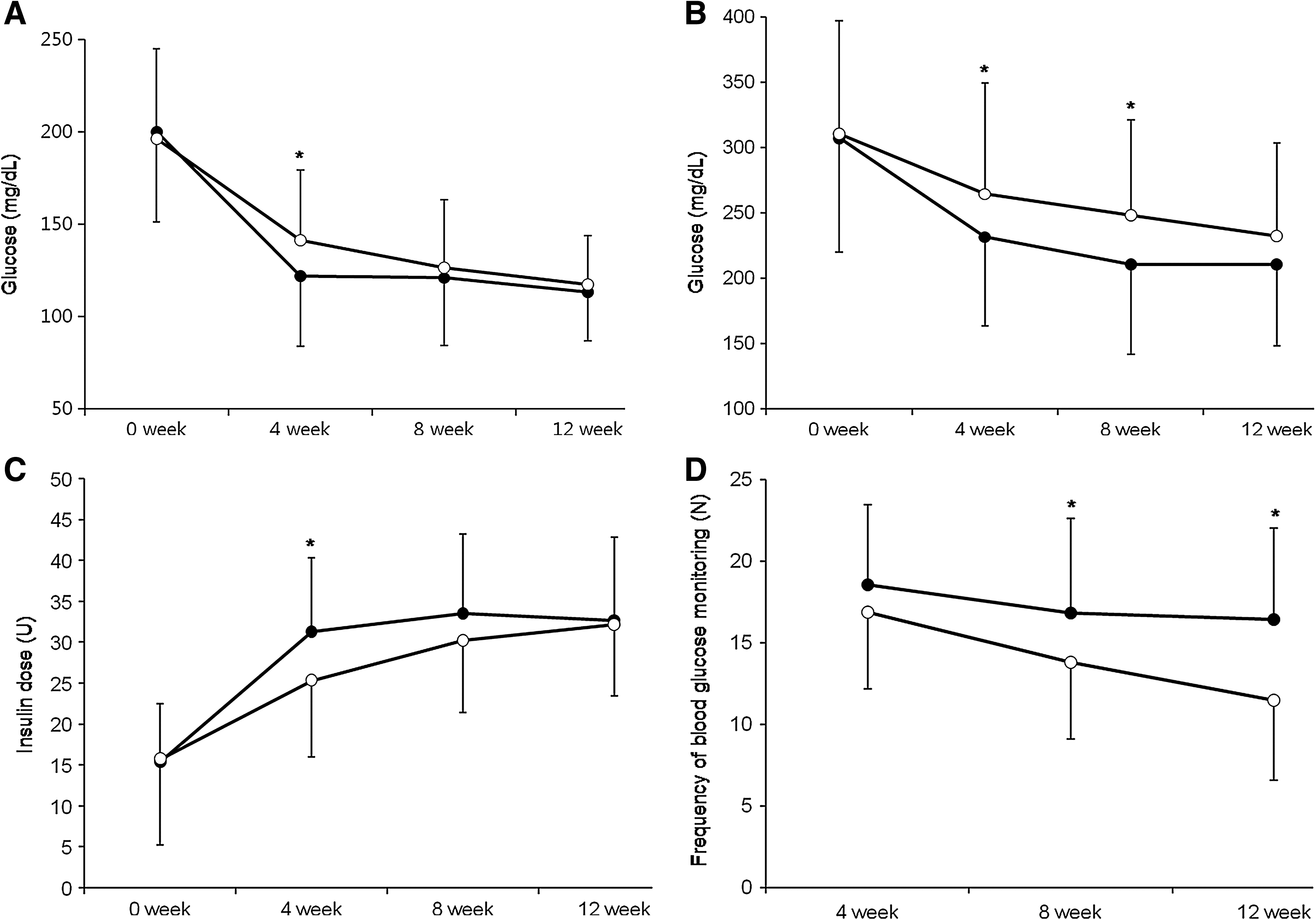
Overall, FBG significantly decreased (P < 0.001) from 198.3 ± 51.2 mg/dL to 115.2 ± 21.5 mg/dL. The FBG of the intervention group declined earlier than that of the control group. However, the FBG after 8 weeks was similar between the two groups (Fig. 1a). Moreover, the reduction of postprandial blood glucose occurred faster than that of the control group, but postprandial blood glucose levels after 12 weeks became similar in both groups (Fig. 1b).
Change of (
No severe hypoglycemic event was reported during the trial in either group. The total number of symptomatic hypoglycemia episodes was similar (P = 0.943) in the intervention group (n = 42 or 0.89 events/subject) and the control group (n = 39 or 0.87 events/subject). The incidence of asymptomatic hypoglycemia (10.6% vs. 11.1%) and nocturnal hypoglycemia (12.8% vs. 11.1%) was low in both the intervention and control groups, with no significant difference between the groups (P = 0.943 and P = 0.749, respectively). Moreover, 42 patients in the control group and 41 in the experimental group were taking medications that can cause hypoglycemia in our study. The incidence of hypoglycemia was as follows: the total number of symptomatic hypoglycemia episodes was similar (P = 0.994) in the intervention group (n = 36 or 0.88 events/subject) and the control group (n = 37 or 0.88 events/subject). The incidence of asymptomatic hypoglycemia (12.2% vs. 11.9%) and nocturnal hypoglycemia (12.2% vs. 7.1%) was low in both the intervention and control groups, with no significant difference between the groups (P = 0.968 and P = 0.833, respectively).
The insulin glargine dose after 4 weeks was higher (P = 0.003) in the intervention group (31.2 ± 9.1 mg/dL) than in the control group (25.3 ± 9.4 mg/dL). However, the doses after 8 (33.5 ± 9.7 vs. 30.2 ± 8.7 mg/dL, P = 0.090) and 12 (32.6 ± 10.2 vs. 32.2 ± 8.7 mg/dL, P = 0.807) weeks were similar between the two groups (Fig. 1c).
There was a small increase in body weight from baseline to end point with both the intervention (2.4 ± 3.0 kg) and control (2.2 ± 2.8 kg) groups with no significant difference (P = 0.653).
The frequency of blood glucose monitoring during the study period in the intervention group was 51.8 ± 16.1 checks, which was significantly higher (P = 0.002) than that of the control group (42.2 ± 13.2 checks). The blood glucose monitoring in the intervention group was conducted in a relatively steady manner for 12 weeks, whereas it was reduced in the control group as time passed (Fig. 1d).
Discussion
A lifetime of strict self-care, along with regular visits to physician's office, is necessary in the management of diabetes. 14,15 However, there is an obvious limitation to meeting these needs in the current healthcare system. 16,17 Because the number of diabetes patients is increasing very rapidly, introduction of a new system that can cover mass blood glucose control is required. Therefore, various approaches such as web- and phone-based healthcare systems have been created to improve the efficiency and quality in managing diabetes patients. 4,18,19
Wireless technology is a universal communication system that enables an individual to be in contact with others ubiquitously. Thus, patient–doctor communication becomes possible anywhere at any time with the use of this system. 20 Nowadays, almost all adults own a cellular phone in many countries and use SMSs in their everyday lives. Telemedicine-based diabetes management systems that provide interactive components have already been proven to be effective in glucose control. 21 Many computerized decision support systems improve practitioner performance. However, to date, their effects on the clinical effectiveness remain understudied. 9
Initiation of insulin therapy in type 2 diabetes can be relatively straightforward, but the follow-up care and essential need for titration can be hugely time consuming. Therefore, we designed the system for type 2 diabetes patients treated with insulin glargine to make an automatic adjustment of insulin dose based on real-time glucose level data and to provide the patients with the needed insulin dose by using an SMS. We have demonstrated that our specialized system is an effective and safe approach to insulin dose adjustments in patients with diabetes. This result has significant clinical implication because our study is exclusive in that clinical advices were made “automatically” through the computerized system, whereas clinical advice was composed by the medical personnel in other telemedicine intervention studies. 7,18
There are some reasons for the better glucose control in the intervention group. Primarily, our specialized system is designed to attain a target glucose level early and has a safety device to prevent or reduce a hypoglycemia episode. With the patient-driven insulin dose titration algorithm, patients can increase an insulin dose by 2 units to minimize a hypoglycemia episode. However, the patients can increase an insulin dose by up to 6 units safely with our algorithm. Moreover, the patients had more frequent contacts with medical advice than those in the control group. In addition, the patients in the intervention group received medical feedback according to their most recent data, thus confirming their current state of blood glucose. These factors may have encouraged the patients to more actively modify their lifestyle for a better glucose control. Indeed, the average frequency of blood glucose monitoring during the study period in the intervention group was significantly higher than that of the control group. Moreover, there was a significant correlation between the number of blood glucose monitoring and the decrease of HbA1C (r = 0.286, P = 0.006) in our study. This tendency was more evident in the experimental group. Therefore, our system not only lowered the patients' blood glucose levels but also helped sustain the decreased levels because the system could continuously prompt the patient's motivation to control his or her glucose levels. More frequent blood glucose monitoring is associated with better metabolic control in insulin-treated type 2 diabetes patients. 22 Whereas blood glucose monitoring in the intervention group was conducted in a relatively steady manner for 12 weeks, it was reduced in the control group as time passed. This study also proved that the system could provide a motivation for patients to manage their diseases. In this study, the frequency of blood glucose monitoring in the control group cannot be enough to yield appropriate insulin dose titrations. However, the dose of insulin tends to be determined at the beginning. As shown in Figure 1d, the average number of blood glucose monitoring checks during the first 4 weeks was 18.6 in the experimental group and 16.9 in the control group, which means that the blood glucose level was checked at least every other day. Therefore, we feel that it is sufficient for adjusting the insulin dose.
Of the 50 patients in the intervention group, 47 patients completed the study. Of three patients withdrawn from the study, one used our system throughout the study period but did not revisit our hospital at 12 weeks. Therefore, at the end of this study, patient compliance with our new system was 96% (48 of 50), suggesting that this regimen was easy to follow. One of the most important determinants of computerized clinical decision support system success is usability. 9 Our system is very simple and easy to use and thus can lead to good results.
In this study, the significant decrease in HbA1C was accomplished with a minimal incidence of hypoglycemia and a small increase in body weight. These findings have important suggestions: insulin therapy is often delayed in type 2 diabetes for many reasons, including fear of hypoglycemia and weight gain, 23,24 despite its apparent metabolic benefits. In this study, although the number of patients was not large enough to compare the frequencies of hypoglycemia in the two groups, a difference regarding hypoglycemia frequencies in the two groups was not found.
The patient-driven insulin dose titration algorithm is simple and effective for improving glycemic control with a low incidence of hypoglycemia. 3 However, in the study patients who used our system had the same incidence of hypoglycemia as patients who used the conventional method. Because our system could increase up to 6 units of insulin dose at once, there was a possibility to have more frequent hypoglycemia; however, there was no difference regarding the incidence of hypoglycemia between the two groups since our system had a protective program to prevent hypoglycemia that may occur often in diabetes patients. Moreover, there was no case of hypoglycemia after 8 weeks in the intervention group (data are not shown). We can infer that the incidence of hypoglycemia could have been more reduced if we had continued to use the system. The lower rates of hypoglycemia with insulin glargine were accompanied by less variability of FPG, which presumably contributed to this advantage.
In this study, the difference of insulin dose in both groups was not observed after 12 weeks. The insulin dose in the intervention group was higher at 4 weeks, suggesting that patients in the intervention group were closer to the optimal dose first. In addition, no difference in terms of weight gain in the two groups was found. Therefore, to our opinion, the application of the system is effective and safe.
We believe our system, which provides medical advice (to optimize the insulin dose) formulated from an automated algorithm, is far more economical than the previous systems, 3 in which medical personnel were required for the same process. We suggest that our system is an effective and probably more economical approach to diabetes management, allowing for application to large groups of patients.
Additionally, if the effectiveness of the system to adjust insulin dose regimen and manage diabetes patients is established, the development of a system having artificial intelligence from advanced computer, web, and mobile phone based on the data accumulated systemically will follow. New medical systems using these functions can be implemented to clinical practice in the future and can have positive impacts on diabetes patients. In addition, once this system is begun to be applied to diabetes patients in clinical practice, it will be implemented rapidly and used widely for the management of chronic diseases such as hypertension, dyslipidemia, and obesity.
In our study, patients were encouraged to adjust their insulin doses to achieve target glycemic control (FBG between 80 and 119 mg/dL). However, by the end of the study, the mean HbA1C value and the percentage of patients with HbA1C <7% in this study population were not optimal, although FBG achieved the target goal. The main reason for not achieving optimal glycemic control may be that the trial was not designed as a treat-to-target (below 7.0% HbA1C) study, and therefore insulin glargine dose titration was not enforced. Although the mean FPG values at the end of the study were still at the upper target range (113.1 mg/dL in the intervention group, 117.4 mg/dL in the control group), the insulin glargine dose adjustments were considerably smaller in the later part of the 12-week study. The insulin dose increase from baseline to week 12 was 0.244 U/kg for the intervention group and 0.243 U/kg for the control group. If the titration target had been strictly lower (80–100 mg/dL), the percentage of patients with HbA1C <7.0% would have been higher. Moreover, baseline HbA1C was relatively high (9.8 ± 1.2%) in this study.
In conclusion, this study demonstrated that use of an SMS automatically produced by a knowledge matrix is an effective and safe approach to long-acting insulin dose adjustments in patients with type 2 diabetes. Moreover, this study provides insight into a widely applicable treatment strategy for insulin glargine, which can easily be translated into clinical practice. However, more studies are required before it can be universally used.
Footnotes
Acknowledgments
We thank the UBCare Company for its large contribution to development of the insulin dose titration system using a short messaging service automatically produced by a knowledge matrix.
Author Disclosure Statement
No competing financial interests exist.
This work was previously presented as a poster presentation at the 45th European Association for the Study of Diabetes Annual Meeting in Vienna, Austria, September 29–October 2, 2009.