
Abstract
Background:
No study of transition from intravenous to subcutaneous insulin after cardiac surgery with dose based on percentage of intravenous total daily insulin (TDI) has reported a clearly superior regimen for achieving target blood glucose. We compared three first-dose transition strategies for insulin glargine: two based on TDI alone and one that also took body weight into account.
Methods:
Mostly obese, type 1 and type 2 diabetes patients (n = 223) undergoing cardiac surgery were randomized to receive insulin glargine subcutaneously at 60% or 80% of TDI or in a dose based on TDI and body weight.
Results:
Transition to subcutaneous insulin occurred 27.4 ± 6.6 h after surgery. Over the study period, mean proportion of blood glucose values within target range (80–140 mg/dL) were 0.34 ± 0.24, 0.35 ± 0.24, and 0.36 ± 0.22 in the 60% TDI, 80% TDI, and weight-based groups, respectively. This difference was not significant. Significantly more insulin corrections were needed in the 60% TDI group than in the weight-based group. There was only one incidence of hypoglycemia (blood glucose <40 mg/dL).
Conclusions:
No subcutaneous insulin regimen implemented approximately 1 day after cardiac surgery showed significantly better control of blood glucose over the 3-day study period. Further studies are needed to determine optimal formulae for effecting an early transition to subcutaneous insulin after cardiac surgery or whether it is preferable and/or necessary to continue intravenous insulin therapy for an additional period of time.
Introduction
No study has yet found a clearly superior dosing protocol for transition from intravenous insulin infusion to subcutaneous insulin in patients after cardiac surgery. Yeldandi et al. 5 compared a dose of once-daily glargine with twice-daily NPH and found no significant differences between the two in mean blood glucose after transition to subcutaneous insulin. About 60% of patients in both groups achieved blood glucose values between 80 and 140 mg/dL. Schmeltz et al. 6 found no significant differences in achieving a predetermined blood glucose target (80–140 mg/dL) using three different doses of insulin glargine: 40%, 60%, and 80% of the intravenous total daily insulin (TDI). In that study, the proportion of patients achieving blood glucose values between 80 and 140 mg/dL ranged from 35% to 48% with no difference between the groups. In these studies, the infusion rate of intravenous insulin was used to calculate the dose of basal insulin during the transition. This approach assumes a relatively stable insulin drip rate in the hours used to determine the presumed TDI at the time of transition.
In the present study, we compared three dosing strategies for insulin glargine—two based on pretransition extrapolated TDI alone and one that took into account both insulin drip rate prior to transition and patient body weight—to evaluate the mean proportion per patient in each study group of blood glucose values in the target range during the 3-day study period.
Subjects and Methods
This prospective, randomized clinical trial received institutional review board approval and was conducted in two urban, tertiary-care teaching, cardiac specialty hospitals in two U.S. cities within the same healthcare system. All participants gave informed consent.
From April 2006 to April 2008, all patients were screened for inclusion if they had type 1 or type 2 diabetes, had undergone uncomplicated cardiovascular surgery, and were being treated with intravenous insulin therapy in the cardiovascular recovery intensive care unit postoperatively. The stated blood glucose target range during intravenous insulin therapy was 80–120 mg/dL. Patients were invited to participate if they were expected to need subcutaneous insulin to maintain blood glucose control after intravenous insulin therapy was discontinued, were extubated, were off vasopressors for >4 h, were afebrile, had no evidence of infection, and were scheduled for transfer out of the intensive care unit. Exclusion criteria were use of high-dose glucocorticoid therapy (>20 mg of prednisone/day or equivalent) and serum creatinine level >2.0 mg/dL. The duration of the study period was 72 h.
Patients were randomized to one of three different dosing regimens (Fig. 1). Estimated TDI was calculated based upon the total number of units of intravenous insulin delivered during the 4 h immediately prior to randomization, multiplied by 6 to extrapolate 24-h TDI. The study was nonblinded. Participants in two groups were randomized to receive 60% or 80% of estimated TDI as insulin glargine. The third group was randomized to receive an insulin glargine dose based on a graded multiplier × body weight (in kg) (Fig. 2). The multiplier ranged from 0.25 to 0.75 units and was assigned based on the mean hourly drip rate in the 4 h prior to transition. Therefore, the dose of glargine in this group was determined by the same assumption used to determine the TDI in the first two groups with a factor added to account for patient body weight as a marker of insulin resistance.
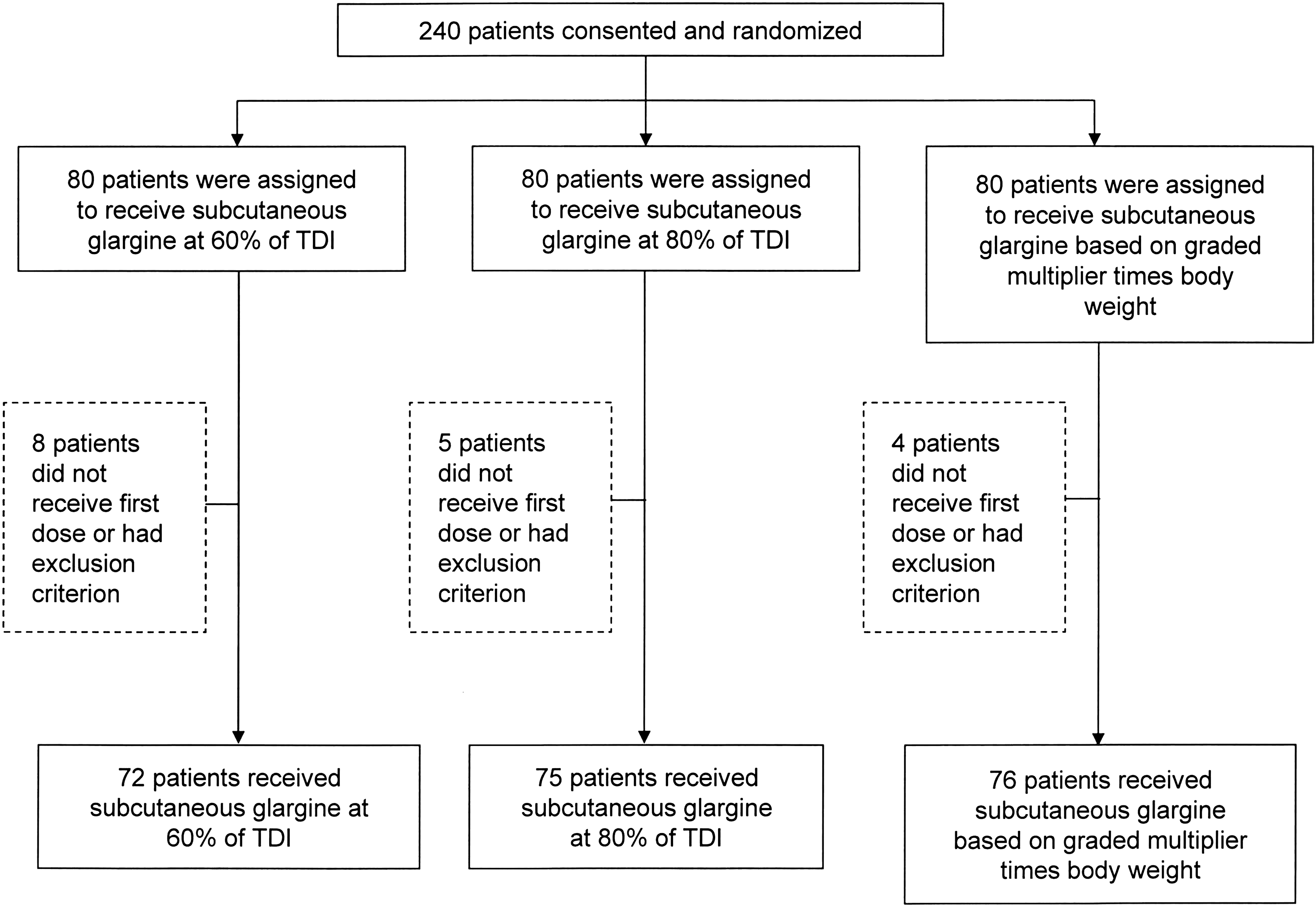
Randomization of patients. Exclusion criteria are listed in Subjects and Methods. TDI, total daily insulin.
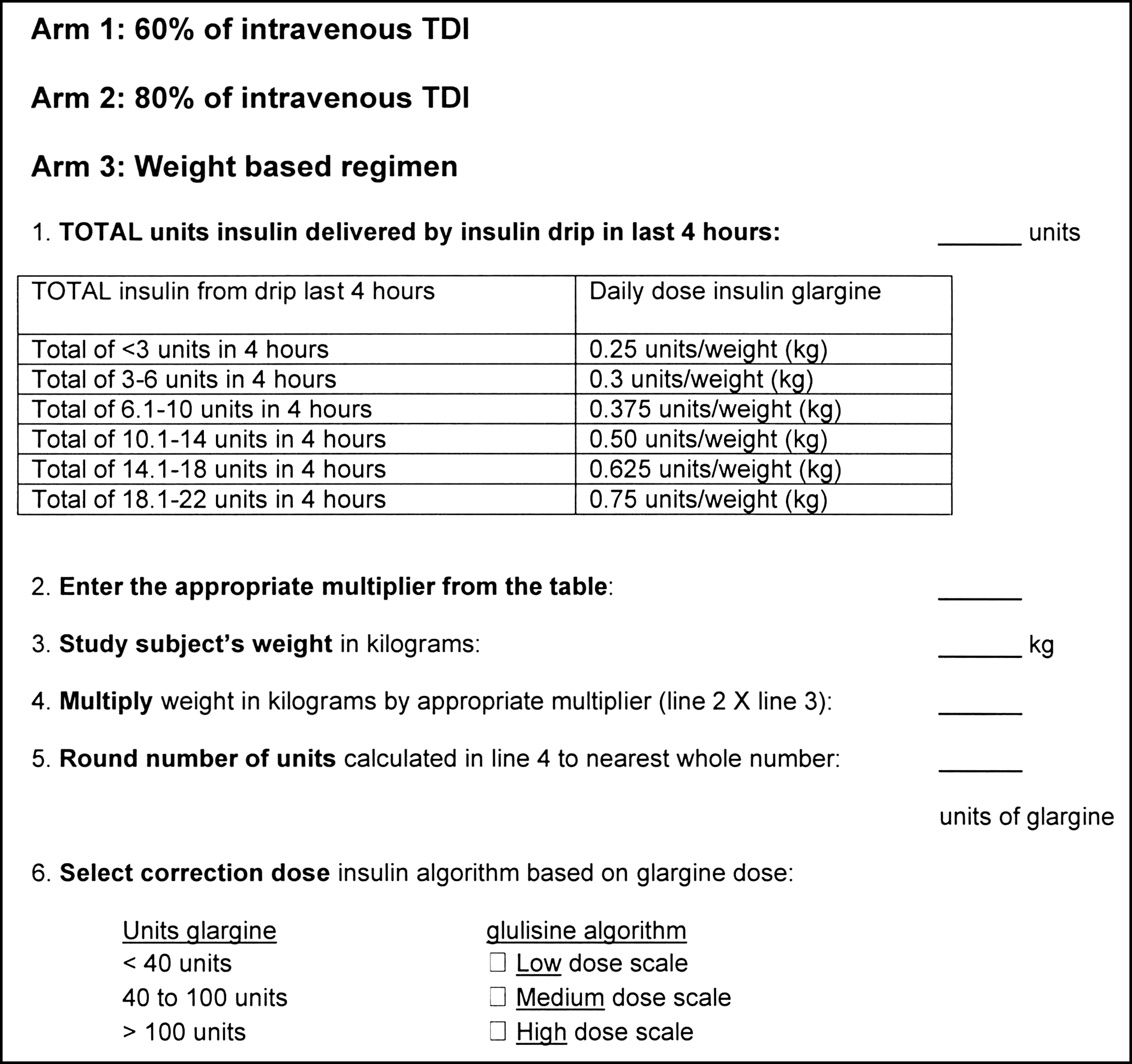
Summary of treatment regimens. TDI, total daily insulin.
When patients began to eat, prandial rapid-acting insulin glulisine was administered before each meal at 10% of the daily glargine dosage. When premeal hyperglycemia was present, patients were also prescribed a correction dose of glulisine that was added to the prandial insulin dose. IIT was discontinued 2 h after the first subcutaneous dose of glargine was given. If the patient was to receive a meal at the time of transition, the first doses of insulin glulisine and glargine were both given at the start of the meal, and the IIT was discontinued at that time. Blood glucose data were collected for each subject for 72 h after the transition. A four-point fingerstick blood glucose profile was measured daily for each patient, before meals and at bedtime if the patient was eating discrete meals or every 6 h if not. A fasting plasma glucose measure was obtained on each study day. Medical providers on the cardiac surgery service were free to adjust the insulin dosing per standard care after the initial glargine dose had been administered. Oral antihyperglycemic medications were allowed prior to discharge.
The primary outcome was proportion per patient of blood glucose values within the target range of 80–140 mg/dL over the 3-day study period. Secondary outcomes were mean blood glucose during the 3-day study, proportion of first-morning postoperative day 2 blood glucose within range, number of correction doses of rapid-acting insulin administered, total mean daily doses of glargine and glulisine, and occurrence rates of severe hypoglycemia (blood glucose <40 mg/dL).
Statistical analysis
The sample size calculation was based on the primary outcome of mean percentage of blood glucose values within the target range over the 3-day study period. Based on data obtained for 26 patients in a pilot study, it was determined that 80 patients per group would give an 80% chance to detect an absolute difference of 0.16 in percentage of total blood glucose values within target at a 0.05 probability, assuming a group mean for one group of 0.24 and an SD of 0.32 using analysis of variance. nQuery (Statistical Solutions, Saugus, MA) was used for the sample size calculations. Two hundred forty subjects were randomized (n = 80 per group).
Baseline characteristics represented by continuous variables, such as age, were compared using analysis of variance or the Kruskal–Wallis test, where applicable. Baseline characteristics represented by categorical variables, such as race, were summarized as percentages and compared using a χ 2 test or the Fisher's exact test for small counts.
The proportion of first-morning day 2 blood glucoses within target range was analyzed by Cochran–Mantel–Haenszel test controlling for site. The remaining study outcomes were analyzed for group differences via generalized linear models. Age, gender, race, and site were included as covariates in all models. For continuous variables, such as mean blood glucose over the study period, adjusted means based on the models are reported. For count variables, such as number of glulisine corrections, the magnitude of group effect is represented as an “event ratio,” the ratio between the expected counts in one category versus the reference category. All analyses were conducted on an intention to treat basis.
A P value of ≤0.05 was considered statistically significant. All P values are two-sided. All statistical analyses were done using SAS 9.1 (SAS Institute, Inc., Cary, NC).
Results
Of the 240 patients consented and randomized, 17 were withdrawn either because they did not receive the first dose of subcutaneous glargine and/or they were found to have an exclusion criterion after randomization. Patient characteristics did not differ except in age (Table 1). No differences were observed among groups by sex, race/ethnicity, hemoglobin A1c (A1C), renal disease, heart failure, or prior thiazolidinedione, sulfonylurea, meglitinide, or preoperative insulin therapy. Mean body mass index was above 30 kg/m2 in all patient groups. A high proportion of patients in all groups had A1C >6.5% (Table 1).
Data are mean ± SD values or percentages as indicated.
The 60% total daily insulin (TDI) group was significantly older than the 80% TDI group.
A1C, hemoglobin A1c; BMI, body mass index; NA, not applicable.
Transition from IIT to the first dose of subcutaneous glargine was made at a mean of 27.4 ± 6.6 h from the time surgery started, and mean duration of intravenous insulin therapy was 20.1 ± 8.4 h. At transition, adjusted mean blood glucose for all groups was above the stated target range of 80–120 mg/dL (Table 2).
Only significant P values for pairwise comparisons are reported here. Adjusted means are adjusted for age, gender, race, and site.
60% TDI group significantly lower than weight-based group (P < 0.05).
60% TDI group significantly lower than 80% TDI group (P < 0.06).
60% TDI group significantly lower than 80% TDI group (P < 0.05).
80% TDI group significantly higher than 60% TDI group and weight-based group (P < 0.06).
60% TDI group significantly lower than 80% TDI group (P < 0.05).
60% TDI group significantly higher than weight-based group (P = 0.04).
SC, subcutaneous; TDI, total daily insulin.
Mean blood glucose at study entry did not differ among groups (Table 2). Over all 3 days, there was no significant difference among groups in mean proportion of within-target blood glucoses or in mean blood glucose. Only 21% of all patients achieved day 2 first morning blood glucose in the target range, and the percentage of patients achieving this goal did not vary significantly among groups. As expected, the mean first dose of glargine was significantly lower in the 60% TDI group compared with the 80% TDI group. Multivariate analysis showed that older age was associated with use of fewer units of glargine.
Patients in the 60% TDI group received a higher mean number of corrections of glulisine insulin over the study period compared with the weight-based group. One patient on the weight-based algorithm had one episode of severe hypoglycemia (blood glucose <40 mg/dL) on day 3.
Discussion
In this large group of obese patients with uncontrolled diabetes undergoing cardiovascular surgery, only a small proportion of within-target blood glucose values were observed in all groups over the 3-day period after transition to one of three subcutaneous basal bolus plus correction dose insulin regimens. No significant difference in this primary outcome was observed between the groups. A low percentage of blood glucose values fell within the target range at first measurement on day 2 in all groups, and the groups did not differ significantly. The first morning day 2 blood glucose reflects the action of the first dose of basal insulin administered at the time of transition on day 1. The weight-based group required fewer doses of correction insulin compared with the 60% group, suggesting a possible role for basal insulin glargine dosing regimens that take body weight into account. Overall, these findings suggest it is challenging to achieve effective control of blood glucose using the tested formulae with subcutaneous insulin dosing introduced at approximately 1 day after cardiac surgery.
The proportion of patients achieving mean blood glucose in the target range was lower than that observed in previous studies, which ranged from 35% 6 to about 60%. 5 We speculate that our results differed from those of the earlier studies for at least two possible reasons. First, our patients were transitioned to subcutaneous insulin at about 1 day after surgery, when the postoperative stress response is still strong and insulin requirements are still high and subject to considerable variability. We are not able to compare these findings with the earlier studies because those studies did not report time from surgery to transition. Second, our study population all had diabetes, and a high proportion of our patients had A1C values at baseline consistent with uncontrolled diabetes prior to surgery (baseline mean A1C >6.5%, ranging from 73% to 85% across groups) with mean A1C values of 8.0%. Yeldandi et al. 5 reported lower mean A1C values of 6.3–6.6%. Schmeltz et al. 6 reported only 35% of patients with diabetes. Also, most patients in the current study were being treated with oral agents and a few with insulin on admission to the hospital. Most were discharged from the hospital with a prescription for insulin. It is possible that preexisting diabetes that was suboptimally controlled prior to cardiac surgery also adversely impacted perioperative glycemic control in our study population. Further study of this question is warranted.
In addition, blood glucose levels at the time of transition to subcutaneous insulin were above the study period intensive care unit target range of 80–120 mg/dL in all groups. This suggests that the transition insulin glargine dose determination based on IIT rate per hour prior to the transition underestimated the insulin requirement at the time.
As in previous reports, 5,6 insulin glargine dosage in units/kg/day decreased over the study period. It is generally held that reduction in TDI will occur with resolution of the acute stress-related factors that cause increased insulin requirements after surgery. However, considering that blood glucose levels were not at goal and severe hypoglycemia rates were low, providers appear to have been making anticipatory reductions in insulin dosage prematurely as recovery progressed, thus further contributing to inability to reach target blood glucose levels.
Use of the tested protocols was safe with respect to hypoglycemia, despite a first dose of insulin glargine over 0.5 units/kg in the 80% TDI group. This is similar to the insulin dose requirement of 0.4–0.5 units/kg administered by Umpierrez et al. 7 to insulin-naive hospitalized nonsurgical patients on a general medical service. Patients in the current cardiac surgery study represent a population resistant to insulin and subject to substantially higher stress of cardiac surgery during the peri-transition period. The subjects in this study appear to have needed incrementally higher subcutaneous insulin doses than they received. How to safely and effectively attain glycemic control at about 24 h following uncomplicated cardiac surgery remains to be determined. It appears reasonable to conclude that transition should occur later, after the stress response has further diminished. Indeed, Furnary et al. 3 and Furnary and Braithwaite 4 recommend 3 or more days of continuous intravenous insulin infusions to control blood glucose in patients after cardiac surgery.
If one is to make the transition to subcutaneous insulin during this earlier postoperative time frame, particularly in the interest of facilitating timely discharge when appropriate, further studies will be needed to determine the optimal apportioning of insulins to meet the patient's transition TDI requirement. It remains to be determined whether it is preferable to administer a higher initial dose of a long-acting basal insulin or to use a basal bolus plus correction dose strategy that relies on higher doses of bolus rapid-acting insulin to allow more flexibility in insulin dosing, in view of quickly changing insulin requirements as the stress response wanes rapidly in the subsequent 24 h. One additional approach for consideration would be application of a higher weight-based factor in determination of the transition basal insulin dose.
In conclusion, none of the three formulae for determining a first dose of basal insulin for transition from intravenous to subcutaneous insulin at approximately 1 day after cardiac surgery tested demonstrated significantly better control of hyperglycemia over the 3-day study period. Further studies are needed to determine optimal formulae for effecting an early transition to subcutaneous insulin after cardiac surgery or to establish whether it is preferable and/or necessary to continue intravenous insulin therapy for an additional period of time.
Footnotes
Acknowledgments
Funding for this study was received from Sanofi-Aventis, which had no role in this investigator-initiated study. We thank Dr. Jennifer P. Holst for her work in early development of the study insulin dosing algorithms. We also thank Flossine Brown, B.S., Sarah K. Driggers, R.N., MSN, and Sharon Taylor-Pannock, N.P., for research coordination and Lyn Camire, M.A., ELS, of the Department of Medicine, Union Memorial Hospital, for editorial assistance.
Author Disclosure Statement
M.E.S. and M.F.M. have received honoraria from Sanofi-Aventis as speakers and consultants and have received research and community education support via funding grants to their institutions. The other authors report no relationship with any manufacturer or other entity in this study that could represent a conflict of interest.