
Abstract
Background:
The present study investigated the enhancement efficiency between liposomes and microbubbles for insulin pulmonary absorption.
Methods:
Two types of phospholipid-based vesicle—liposomes and microbubbles—were prepared, and the 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyl-2H-tetrazolium bromide (MTT) cytotoxicity test was used to evaluate their in vitro toxicity in A549 cells. Cellular uptake of insulin combined with liposomes or microbubbles was determined using A549 cells. With intratracheal insufflation of Sprague–Dawley rats, an insulin mixture with liposomes or microbubbles was administered to assess its potential for promoting drug pulmonary absorption.
Results:
Both liposomes and microbubbles had a narrow and monodispersed size distribution with average diameter of 3.1 μm and 1.0 μm, respectively. From the MTT cytotoxicity test, a phospholipid-based vesicle concentration of <25% (vol/vol) in the final volume was the safe dosage range that could avoid severe cytotoxic effects. The intracellular uptake amount of insulin in the insulin–microbubble mixture was significantly higher than that in the insulin–liposome mixture. The minimum reductions of the blood glucose concentration produced by insulin–microbubble and insulin–liposome mixtures were 60.8% and 35.0% of the initial glucose levels, respectively, and their bioavailabilities relative to subcutaneous injection were 48.6% and 30.8%, respectively.
Conclusions:
Microbubbles have much better efficiency than liposomes in the rate and extent of insulin pulmonary absorption. Microbubbles might be recommended as a potential agent for enhancing protein intrapulmonary absorption.
Introduction
Liposomes are concentric bilayered vesicles in which an aqueous volume is entirely enclosed by a membranous lipid bilayer mainly composed of natural or synthetic phospholipids. 11,12 The utilization of liposomal drug formulations has many potential advantages, including aqueous compatibility, sustained release to maintain therapeutic drug levels, and facilitated intracellular delivery. 10,13 Furthermore, drug–liposomes may prevent local irritation and reduce toxicity both locally and systematically. Increased potency with reduced toxicity is characteristic of many drug–liposomal formulations. 14,15 As a type of promising vehicle, liposomes are widely used for drug pulmonary delivery. Darwis and Kellaway 16 tried to nebulize beclomethasone dipropionate liposomes from the nebulizer for drug pulmonary deposition. Lu and Hickey 17 studied the feasibility of liposomal dry powder aerosols for protein pulmonary delivery. Liu et al. 18 studied the effect of liposomes on increasing the insulin pulmonary absorption. However, the experimental results showed that there was no difference in bioavailability between liposome-entrapped insulin and insulin administered with blank liposomes.
Lipid-coated microbubbles are widely used in biomedical imaging and protein delivery. With the structure of lipid shell and gas core, a lipid monolayer shell will form spontaneously around a newly entrained gas bubble. 19,20 Phospholipid-based microbubbles are bioinspired and compliant of lung surfactant because of their shell component. Indeed, lung surfactant was discovered based on the observation of stable microbubbles formed from lung lavage. The ability of lung-derived fluid to form stable microbubbles is being pursued as a clinical means of assessing lung surfactant viability in neonates. 21,22 Cavitation of microbubbles in an ultrasound field can increase the permeability of an endothelial vasculature, allowing small molecules to enter into tissue from the bloodstream. 23 Juffermans et al. 24 suggested that microbubble oscillation near a cell membrane surface could cause hyperpolarization of the membrane, which might promote endocytosis of external macromolecules. Considering all these characteristics, microbubbles have the potential of enhancing drug pulmonary absorption. Zhou et al. 25 tried to use ultrasound-mediated microbubble cavitation to enhance gene transduction in rat pulmonary endothelial cells in vitro. Although anticancer drug-loaded phospholipid microbubbles as a novel way of targeted tumor therapy have been popular, there have been few reports about improving drug pulmonary absorption by microbubbles in experiments in vivo.
As enhancement agents for drug pulmonary absorption, liposome- and phospholipid-based microbubbles are similar in the form of the shell, the shape of vesicles, and a component of shell membrane. Therefore, the aims of this study were to present (1) the preparation and characterization of liposome- and phospholipid-based microbubbles, (2) a comparative analysis of their in vitro cytotoxicity and enhancement of cellular uptake, and (3) a preliminary evaluation of the effect of liposomes and microbubbles on improving insulin pulmonary absorption.
Materials and Methods
Preparation of phospholipid-based liposomes and microbubbles
Liposomes were prepared by the thin film hydration method as previously described. 26 In particular, 15 mg of a mixture of hydrogenated phosphatidylcholine (>99%) (Doosan Corp. Biotech BU, Kyonggi Do, Republic of Korea):cholesterol (Sigma Chemical Co., St. Louis, MO) (2:1 wt/wt) was dissolved in chloroform (analytical grade) (Beijing Chemical, Beijing, China), in a 250-mL round-bottom flask containing glass beads. The solvent mixture was removed from the lipid phase by rotary evaporation at 50–60°C (model RE52-AA rotary evaporator, Shanghai Yarong Biochemistry Instrument Inc., Shanghai, China), to obtain a thin film of lipids on the wall of the flask and the surface of beads. Subsequently, the flask was kept overnight under vacuum to ensure the complete removal of residual solvent. The dry lipid film was hydrated with physiological saline solution at a temperature of 60 ± 2°C. The dispersion thus obtained was vortex-mixed for about 2 min. The dispersion was left undisturbed at room temperature for 2–3 h to allow complete swelling of the lipid film and hence to obtain the liposome vesicular suspension.
Phospholipid-based microbubbles were prepared by the sonication–lyophilization method reported in our previous study. 20,27 In brief, preparation was as follows: hydrogenated phosphatidylcholine (>99%), polyethylene glycol 1500 (Qingming Chemical, Wenzhou, Zhejiang Province, China), and poloxamer 188 (Shenyang Chemical, Shenyang, Liaoning Province, China) were dissolved in normal butanol (analytical grade) (Beijing Chemical Plant) and sonicated at 30°C (JY 92-II ultrasonic processor, KunShan US Instrument Inc., KunShan, China) at a frequency of 40 kHz and power of 160 W for 3 min. The solution was stored at 0°C for 30 min and at −20°C for 1 h. Then, the coagulated solution was lyophilized at 5 × 10−4 Pa pressure for 20 h (primary drying at −48°C for 15 h, and then the temperature was gradually raised to 10°C within 5 h). Lyophilized powder was put in 10-mL penicillin vials (100 mg per vial) and saturated with perfluoropropane (electronic grade) (Institute of Special Gas, Tianjing, China).
Microbubble suspension was obtained by dissolving 100 mg of gas-saturated lyophilized powder in 1 mL of physiological saline followed by gentle shaking to form an emulsion-like solution.
Characterization of phospholipid-based microbubbles
Morphologic characteristics of liposomes and microbubbles were determined using transmission electron microscopy (model H-600 transmission electron microscope, Hitachi, Tokyo, Japan) and optical microscopy (model YS100 microscope, Nikon, Tokyo). Both the liposome vesicular suspension and microbubble suspension were gently shaken before one drop was applied to the microscope slide. A coverslip was used to cover the sample before the sample was examined under ×400 magnification.
Particle size and concentration of liposomes and microbubbles were analyzed on a Coulter counter (Coulter Corp., Hialeah, FL). For each sample, 10–15 μL of lipsome or microbubble solution was analyzed. The Coulter unit aperture was flushed with distilled water before and after use.
Cytotoxicity assay
The cell lines used for evaluation were the human lung adenocarcinoma epithelial cell line A549 (a gift from the Institute of Biological and Natural Medicine, Wenzhou Medical College, Wenzhou). A549 cells were propagated in Dulbecco's modified Eagle's medium (Genom Inc., Hangzhou, Zhejiang Province, China) containing 10% fetal calf serum, 100 IU/mL penicillin, 100 mg/mL streptomycin, and 2 mmol/L
Considering blank liposomes, microbubbles, and drug might cause cytotoxic action, experiments were designed to investigate their influence on cell viability. Both blank liposomes and microbubble suspension were used at five levels—3%, 6%, 12%, 25%, and 50% (vol/vol) concentration in the final volume—with the insulin used at six concentrations—0.02, 0.2, 2, 5, 10, and 20 IU/mL. Cytotoxicities of liposomes, microbubbles, and drug were evaluated with the 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyl-2H-tetrazolium bromide (MTT) assay as in our previous study. 28 A549 cell suspension (100 μL, 0.5 × 104 cells per well) was seeded to a 96-well cell culture plate (Costar®, Corning Inc., Corning, NY) and incubated at 37°C in a CO2 incubator for 24 h. Various concentrations of liposomes, microbubble suspension, and insulin solution were added to the designated wells, mixed thoroughly, and incubated for 1 day; then 50 μL of MTT solution (5 mg/mL) was added into each well, including the cell-free blank wells. Cells were incubated for 4 h at 100% humidity. After 4 h, MTT solution was removed and replaced with 100 μL of dimethyl sulfoxide. The plate was further oscillated for 10 min at room temperature, and the absorbance (A) of each well was determined using a spectrophotometer (model SMP500-13732-UJRK, MDC, Sunnyvale, CA) at a test wavelength of 550 nm. Cell viability was determined with the following formula: Cell viability (%) = (experimental group A value/control group A value) × 100%.
Insulin cellular uptake study
Based on the toxicity study results, an insulin concentration of 2 IU/mL was used in the drug cellular uptake study. Insulin permeation into A549 cells was performed in 24-well cell culture plates (Costar Inc.) in which cell suspension (300 μL, 8 × 105 cells per well) was previously seeded. After cells were incubated for 24 h, 100 μL of 2 IU/mL insulin solution in Dulbecco's modified Eagle's medium, insulin–liposome mixture, and insulin–microbubble mixture was added, respectively. The medium was removed at different intervals (0, 30, 60, 90, 120, 180, and 240 min), and cells were washed four times with phosphate-buffered saline at 4°C. Cells were than resuspended and digested by incubation with 500 μL of 0.1% Triton X-100 overnight at 4°C. This mixture was filtered (pore size, 0.45 μm), and the content of insulin uptake into the cells was determined by electrochemiluminescence immunoassay.
Pulmonary absorption study
Dosage design
For the insulin solution, the insulin injection (40 U/mL, Wangbang BioPharma Corp., Jiangsu, China) was diluted with physiological saline to a concentration of 2 U/mL.
For the insulin–liposome mixture solution, the liposome vesicular suspension was mixed with an equal volume of insulin injection (4 U/mL). The insulin–microbubble mixture solution contained the same concentration of insulin as the insulin solution.
For the insulin–microbubble mixture solution, the microbubble suspension was mixed with an equal volume of insulin injection (4 U/mL). The insulin–microbubble mixture solution contained the same concentration of insulin as the insulin solution.
Animal experiments
Male Sprague–Dawley rats (weighing 200–300 g) (Slac Laboratory Animal Corp., Shanghai) were kept under a 12-h day–night cycle at 20°C and a relative humidity of 50% for 7 days. The animals were fasted but allowed free access to water for 12 h prior to each experiment. The insulin solution, insulin–liposome mixture, or insulin–microbubble mixture were administered by the modified Schanker's intratracheal instillation. 29 Following anesthesia with intraperitoneal injection of 350 mg/kg chloral hydrate, rats were placed in a supine position on a surgical board. With the animal hanging from the upper incisors, the trachea was subjected to a incision longitudinal along the ventral aspect of the neck. A needle was gently inserted into the exposed trachea between the fifth and sixth tracheal rings. Then the needle was removed, and a tube was inserted smoothly and rapidly until slight resistance was felt. After 200–300 μL of treated solution followed by an equal volume of air was administered to the lung at the vertical through a pipette directly into the tube, the tube was removed immediately, and rats were held gently upright (vertical) by holding their anterior paws and moving them gently. The incision in the skin was sutured with a sterile 4/0 silk suture and swabbed with betadine solution. For evaluating the effect of penetration on insulin pulmonary absorption, insulin doses were 2 IU/kg of body weight, and the doses of liposomes and microbubbles were 25% (vol/vol). The glucose concentrations of blood samples withdrawn from the tail vein at appropriate intervals were measured with the Pro doctor® blood glucose monitoring system (HMD BioMedical Inc., Chunghwa, Hsinchu, Taiwan). The bioavailability of pulmonary administered insulin was calculated relative to that by the subcutaneous route. In brief, an insulin solution for subcutaneous injection (1 U/kg) was given on the nape of the neck of normal rats in the pulmonary absorption study. These animal experiments were approved by the ethical committee for treatment of laboratory animals of Wenzhou Medical College.
Data analysis
To estimate the effect of insulin pulmonary absorption, the blood glucose concentration was measured with the Pro doctor blood glucose monitoring system at the indicated time intervals. The percentage minimum reduction of the blood glucose concentration (% MRBG) at the time of maximum glucose reduction was derived directly from the each group blood glucose level. The percentage blood glucose level (BG %) was calculated as BG % = (BG t /BG0) × 100%. BG0 was the fasting blood glucose level at zero-time, and BG t was the blood glucose level at any time t. 30 The decrease in the blood glucose concentration (D%) was calculated by the method of Leng and Kong 31 with the following equation: %Dx h = (BG0 − BG t )/BG0 × 100%.
The bioavailability relative to subcutaneous injection was calculated by F = AUC x × Dosesc/AUCsc × Dose x , where AUC0→12h is the area under the curve of D% for 12 h and was calculated by the linear trapezoidal rule. 29
Statistical analysis
Statistical significant of differences for multiple groups was determined using a one-way analysis of variance with a Newman–Keuls post hoc test. Statistical significance between individual groups was determined using a Student's t test. All testing was done using SAS version 8.01 software (1999–2000, SAS Institute Inc., Cary, NC). The difference in data was considered to be statistically significant when the P value was <0.05.
Results and Discussion
Characterization of insulin–liposome and insulin–microbubble solutions
As reported above, liposomes were prepared by the thin film hydration method, and microbubbles were prepared by the sonication–lyophilization method we described previously. 20,27 Micromorphology of liposomes and microbubbles was observed via transmission electron microscopy and optical microscopy, respectively (Fig. 1). As shown in Figure 1, both liposomes and microbubbles were characterized by spherical vesicle morphology. Especially for microbubbles, the shape of vesicles remained unchanged, and no aggregation or fusion was observed. Table 1 shows the size of vesicles (liposomes or microbubbles) and vesicle-associated insulin. Because the insulin–liposome mixture or insulin–microbubble mixture was prepared with a simple blending method, little change was observed between blank liposome/microbubble solution and insulin–liposome/microbubble mixture solution.
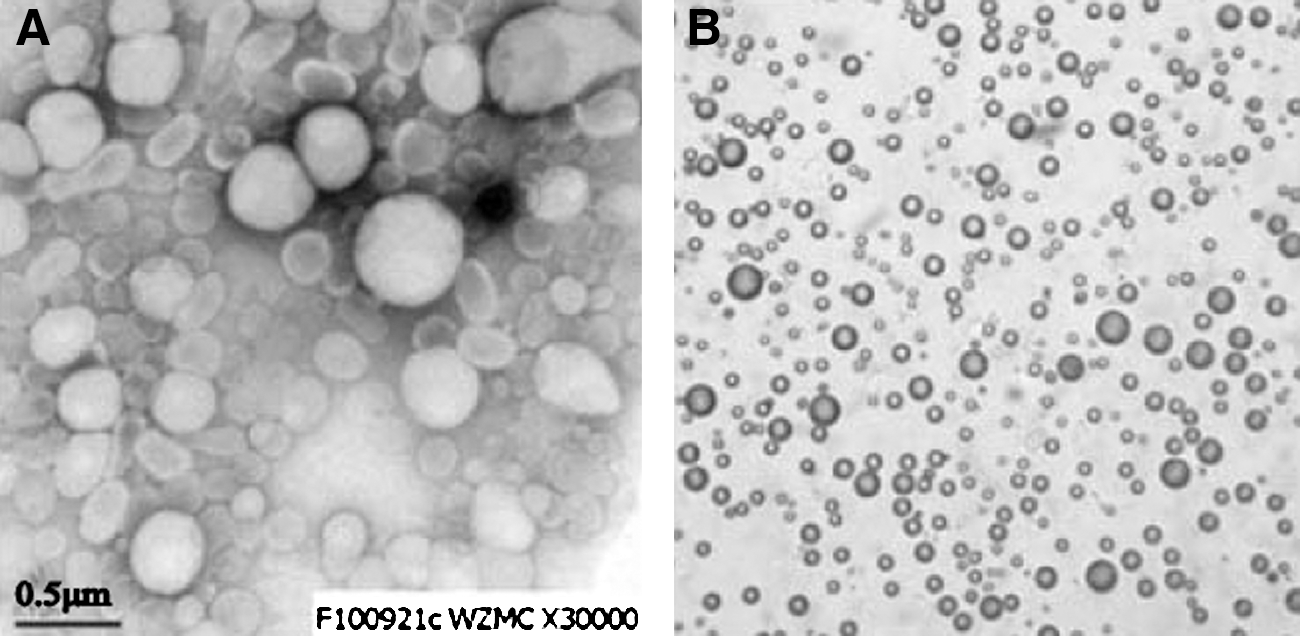
Photomicrographs of (
Data are mean ± SD values of five independent tests.
Polydispersity index (PI) = SD/d, where SD is the SD of the particle size and d is the mean particle size.
Cytotoxicity assay
The cytotoxicities of vesicles in both liposomes and microbubbles were dependent on the vesicle concentration by the MTT test. As seen in Figure 2, high vesicle concentration caused low cell viability. No significant difference of cytotoxicity was observed between the insulin–liposome mixture and the insulin–microbubble mixture. Vesicles caused no decrease in viability of A549 cells in 96-well plates at a concentration of <25% (vol/vol). At high vehicle concentration (50%, vol/vol), microbubbles caused almost half of the cells to die (55.3% cell viability). However, the viability of liposomes at 50% concentration (vol/vol) was 68.8%, which was much higher than that of microbubbles. Based on these results, liposomes have a relative wider safe dosage range for cells than microbubbles. In order to avoid any severe cytotoxic effects of vesicles, the cellular uptake study and the insulin pulmonary absorption study were conducted using a vesicle content of <25% (vol/vol). The insulin concentration was set at six levels to evaluate the influence of drug concentration on cell viability, as shown in Figure 3. The viability of A549 cells in the 96-well plates was dramatically decreased in the presence of the ≥10 IU/mL insulin solution. Accordingly, 2 IU/mL insulin solution was recommended as the optimum vehicle concentration in the subsequent insulin cellular uptake study.

Viability of A549 cells in 96-well plates after exposure to a 3–50% (vol/vol) concentration in the final volume of liposomes and microbubble suspensions as measured with the 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyl-2H-tetrazolium bromide test. Data are mean ± SD values (n = 5).
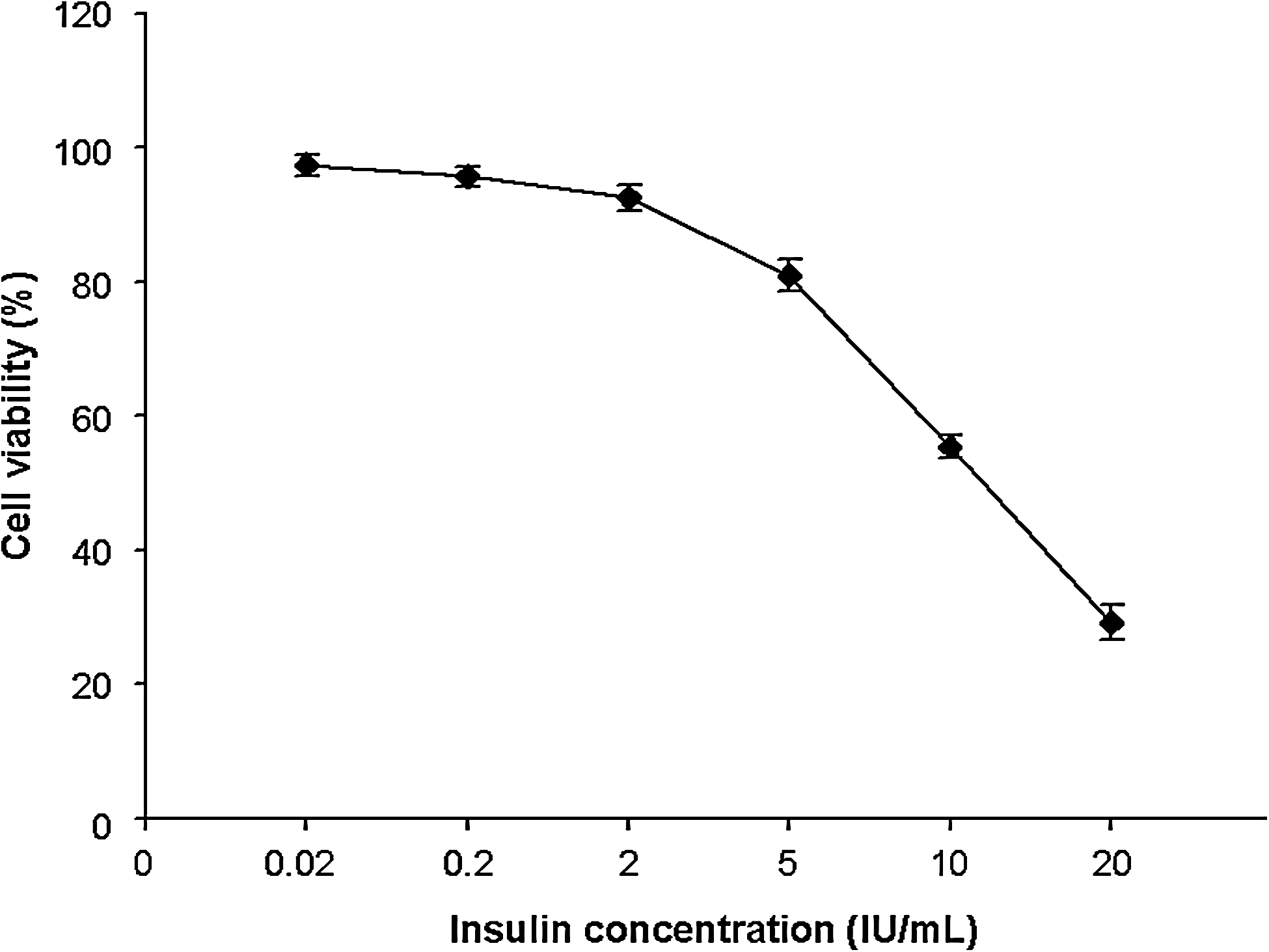
Viability of A549 cells in 96-well plates after exposure to a 0.02–20 (IU/mL) insulin concentration as measured with the 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyl-2H-tetrazolium bromide test. Data are mean ± SD values (n = 5).
Insulin cellular uptake
Figure 4 shows that the cellular uptake of insulin from the insulin–microbubble mixture solution was significantly higher than that from the insulin–liposome mixture solution after 1 h of incubation (P < 0.05). Compared with the liposome- and microbubble-associated mixtures, the amount of insulin uptake into the A549 cells from insulin solution was very low (P < 0.01), which was similar to the result of the group given Dulbecco's modified Eagle's medium without added insulin.
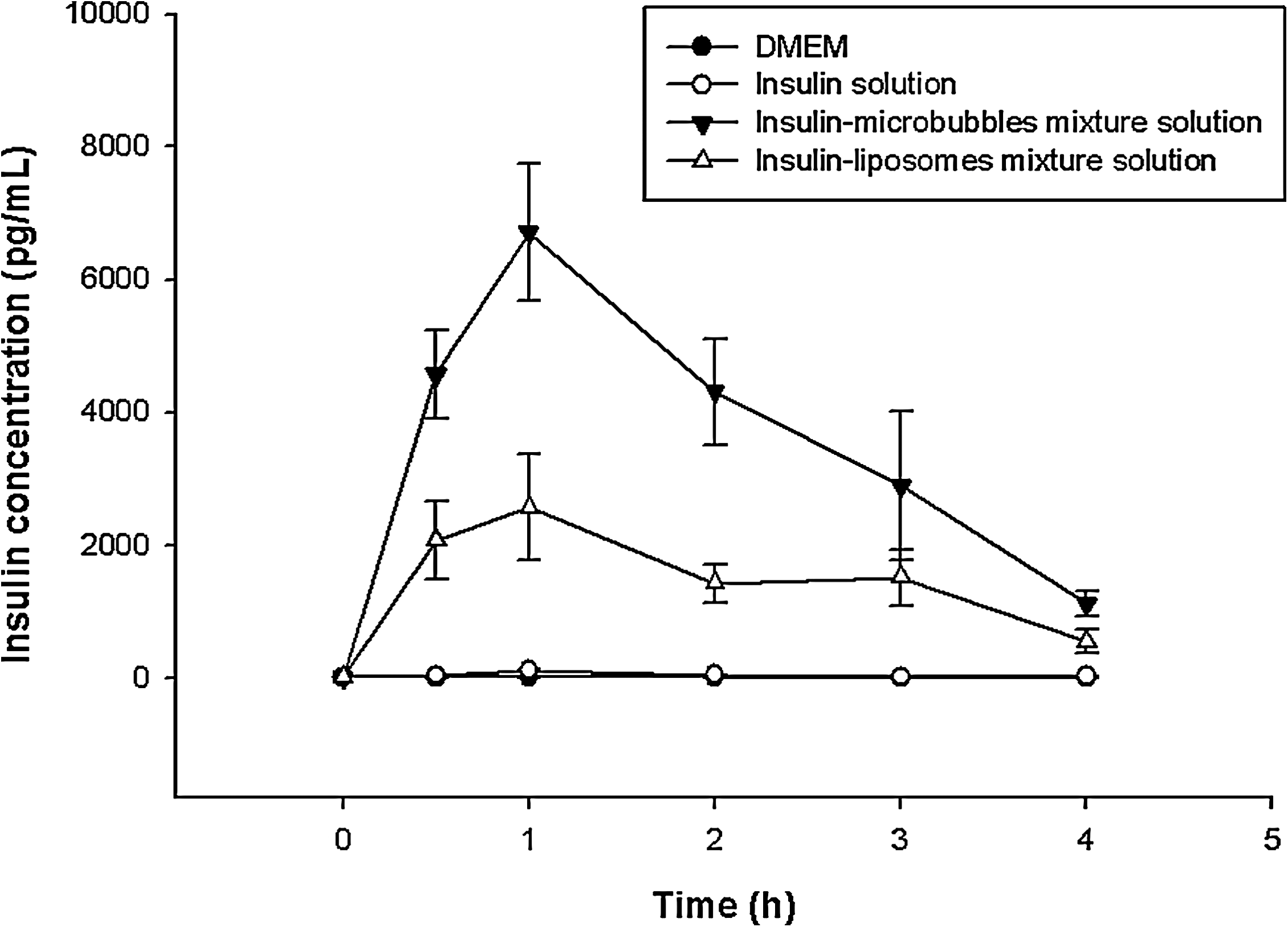
Comparative cellular uptake of insulin after administration of liposomes, microbubbles, and drug solution to A549 cells. Data are mean ± SD values (n = 3). DMEM, Dulbecco's modified Eagle's medium.
Insulin content transported into cells appeared to have a parabolic tendency, which was in accordance with the plasma insulin concentration versus time profile following nasal administration. 32 As shown in Figure 4, insulin cellular uptake for the liposome- and microbubble-associated mixture groups peaked at 1 h and then declined during the next 3 h of observation. This phenomenon might result from the short half-life of insulin (4–6 min) and cell degradation. 33 From the area under curve shown in Figure 4, microbubbles exhibited a better cellular uptake of insulin than liposomes.
Blood glucose level in vivo
According to the optimum conditions based on the cell experiment in vitro, pulmonary absorption in vivo was further studied to compare the enhancement efficiency between liposomes and microbubbles for insulin pulmonary absorption. The decrease in the blood glucose concentration following intrapulmonary administration of the insulin–liposome mixture solution (2 units/kg) and the insulin–microbubble mixture solution (2 units/kg) is shown in Figure 5. The traditional insulin solution for subcutaneous injections (1 unit/kg) was used as the control. Related values of the pharmacodynamic parameters in the different groups are listed in Table 2. The blood glucose levels in the rats receiving different treatments decreased with time and reached minimum values at the following time points: 4 h for intratracheal insulin–microbubble mixture solution (% minimum blood glucose concentration [MBGC], 39.2%), 5 h for intratracheal insulin–liposome mixture solution (% MBGC, 65.0%), 6 h for intratracheal insulin solution (% MBGC, 65.4%), and 2.5 h for subcutaneous insulin solution (% MBGC, 24.7%). Microbubbles showed better efficiency and a higher rate of decreasing blood glucose concentration than liposomes. The % MRBG produced by the insulin–microbubble mixture solution (60.8%) was greater than that of the insulin–liposome mixture solution (35.0%) and insulin solution (34.6%) for the initial glucose levels with pulmonary administration.
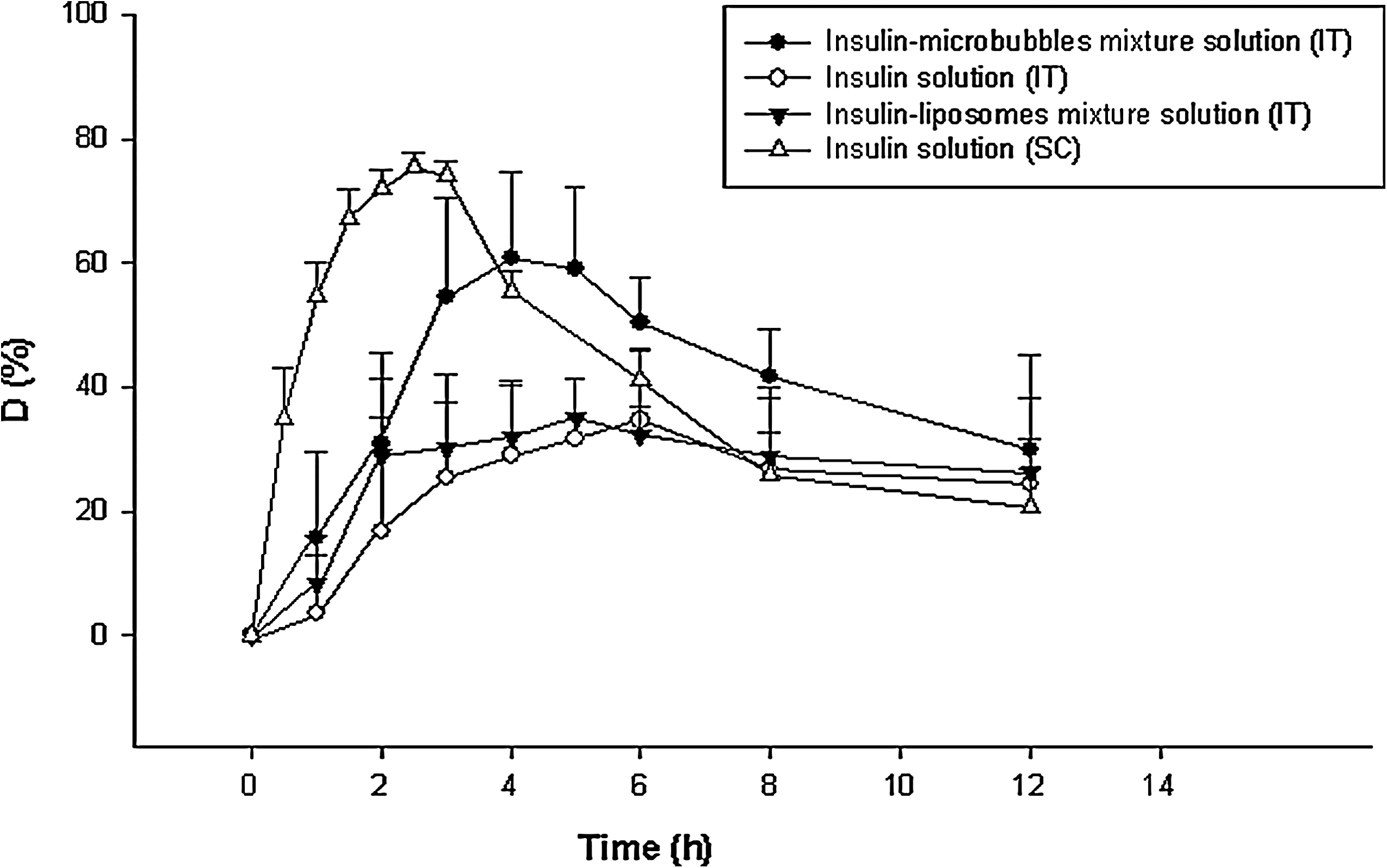
Decrease of the blood glucose concentration (D%) after intratracheal delivery (IT) of liposome-/microbubble-associated insulin solution and subcutaneous injection (SC) of insulin solution: insulin–microbubble mixture solution by IT (2 IU/kg) (•), insulin–liposome mixture solution by IT (2 IU/kg) (▼), insulin solution by IT (2 IU/kg) (○), and insulin solution by SC (1 IU/kg) (△) (n = 7). Data points (mean ± SD) represent relative values of the initial glucose concentration.
Data are mean ± SD values (n = 7).
Statistical significance: ** P < 0.01.
F, bioavailability relative to subcutaneous injection; IT, intratracheal instillation delivery; MBGC, minimum blood glucose concentration; MRGB, minimum reduction of blood glucose concentration; SC, subcutaneous injection.
Therefore, insulin pulmonary absorption enhanced by microbubbles was better than that by liposomes. The profile of blood glucose level of liposomes was similar to that of the insulin solution with pulmonary administration (P < 0.05). The F value (representing bioavailability relative to subcutaneous injection) of microbubble-associated administration (48.6%) was much higher than that of liposome-associated (30.8%) administration and subcutaneous insulin solution-only administration (29.1%). Pulmonary drug administration of most peptide/protein drugs is characterized by the low bioavailability due to the barriers of low permeability, mucociliary clearance, lung macrophages, and enzymatic degradation. 34 Therefore, it is necessary to enhance pulmonary absorption for optimal pharmacological response. Microbubbles could dramatically improve the bioavailability of insulin pulmonary delivery, which might become a novel technique for insulin pulmonary absorption.
Conclusions
In this article, an experiment was designed to compare the enhancement efficiency between liposomes and microbubbles for insulin pulmonary absorption. Both blank liposomes and microbubbles had a homogeneous spherical shape, with a narrow, monodispersed size distribution. Little changes of morphologic characteristics were observed between blank phospholipid-based vesicles and insulin–vesicle mixture solution. From the MTT assay, a vesicle concentration of <25% (vol/vol) in the final volume is a safe dosage range that can avoid severe cytotoxic effects. From the animal study, microbubble-associated insulin can significantly reduce the blood glucose concentration of normal Sprague–Dawley rats by intratracheal instillation compared with liposome-associated insulin. The bioavailability of intrapulmonary administration of the insulin–microbubble mixture (48.6%) relative to subcutaneous injection is much higher than that of the insulin–liposome mixture (30.8%). From these results, microbubbles have much better efficiency than liposomes in the rate and extent of insulin pulmonary absorption. Microbubbles might be recommended as a potential agent for enhancing protein intrapulmonary absorption.
Footnotes
Acknowledgments
This research was supported by the National Natural Science Funds (grants 30870755, 81071277, and 81071164), the Natural Science Foundation of Zhejiang Province (grants Y2110587 and Y2080915), Medicine and Health Grants from the Wenzhou Bureau of Science and Technology (H20100017 and Y20100029), Zhejiang Province funds for Talented Youth in Medical Technology (grant 2010ZQ007), and the Zhejiang Science and Technology Innovation program for students (M.Z., L. Zheng, and J. Huang [only M.Z. is a co-author]).
Author Disclosure Statement
No competing financial interests exist.