
Abstract
Background:
To evaluate whether structured self-monitoring of blood glucose (SMBG) is associated with changes in diabetes-specific quality of life (DSQoL) and locus of control (LOC) in patients with noninsulin-treated type 2 diabetes (T2DM).
Study Design and Methods:
In this analysis of the PRISMA (Prospective Randomized Trial on Intensive SMBG Management Added Value in Noninsulin-Treated T2DM Patients) Study psychosocial data, we evaluated the impact of 12 months of structured SMBG on the individual domains of DSQoL and LOC questionnaires, including the role of selected confounders.
Results:
The score for Satisfaction, Impact, and Worry domains (DSQoL) improved when compared with baseline, without significant differences between structured SMBG regimen (intervention group, n = 501) and active control group (n = 523). Scores for Internal, Chance, and Powerful Others domains (LOC) improved compared with baseline, with a significant between-group change in Chance (P = 0.0309). For DSQoL domain score, improvements were associated with higher number of SMBG measurements (P = 0.007), older age (P = 0.013), and male sex (P = 0.0133) for Satisfaction and with male sex (P < 0.0001) for Worry. Concerning LOC domain score, improvements were associated with longer diabetes duration (P = 0.0084) and younger age (P < 0.0001) for Chance and total number of SMBG measurements (P = 0.0036) for Internal, with the intervention group close to being significant (P = 0.06).
Conclusions:
Our analysis demonstrates that in patients with noninsulin-treated T2DM, structured SMBG is not associated with a deterioration of quality of life and LOC, which is strongly predicted by demographics and diabetes-related variables. These findings should be considered when tailoring educational support to SMBG for these patients.
Introduction
S
SMBG has been associated with a poorer quality of life (QoL), suggesting that the positive effects on metabolic control could be counterbalanced by psychological distress, thus casting doubts on using SMBG in patients who do not require capillary glucose results to adjust the insulin dose at meal time. However, some authors have suggested that the negative impact of SMBG on QoL is limited to noninsulin-treated patients, being possibly a consequence of the frustration deriving from target glycemic values that cannot be autonomously modified. 3,4
In line with this hypothesis, a deterioration of QoL with SMBG has not been described in insulin-treated patients, 4 and a recent report suggests that in adults with type 1 diabetes, continuous glucose monitoring with a subcutaneous sensor is, on the contrary, associated with an improvement of the satisfaction related to therapy. 5
Based on these evidences, whether SMBG has a negative impact on QoL in noninsulin-treated diabetic subjects is still a matter of debate. A previous analysis of the PRISMA Study indicated that in addition to the positive effect on HbA1c, structured SMBG had no negative impact on diabetes-specific quality of life (DSQoL). 1 Furthermore, the same analysis revealed better scores in the locus of control (LOC), suggesting that patients in the more intensive SMBG group were less likely to attribute their diabetes control to chance or fortune than those on active usual control. 1
To better clarify this issue, we used the PRISMA Study psychosocial data to evaluate the impact of 12 months of structured SMBG on the individual domains of DSQoL and LOC, including the role of selected confounders.
Study Design and Methods
The PRISMA Study protocol has been presented in detail elsewhere. 6 Briefly, the PRISMA Study was a 12-month, prospective, multicenter, open, parallel group, randomized, and controlled trial with the aim of evaluating the added value of an intensive, structured SMBG regimen (intensive structured monitoring [ISM] group, n = 501) compared with active control (AC group, n = 523) in type 2 diabetes patients treated with oral agents and/or diet enrolled in 39 diabetes clinics in Italy.
Eligibility criteria were type 2 diabetes not treated with insulin for 1–10 years, age 35–75 years, and HbA1c 7.0%–9.0% (53–75 mmol/mol). Exclusion criteria were insulin treatment for >7 days, previous use of structured SMBG, impending complications of diabetes, limited life expectancy, pregnancy, breastfeeding, or intent to become pregnant.
All eligible patents were randomized 1:1 to either the ISM group or AC group. Patients in the ISM group were required to perform four-point capillary glucose measures 7,8 3 days/week, every week, for 12 months. Furthermore, they were trained to interpret SMBG data and were given a diary listing glycemic targets and suggestions for reaching treatment goals. To obtain data for comparison with the ISM group, patients in the AC group were required to complete a 3-day four-point profile before study visits at months 6 and 12.
These data were not available to clinicians for the adjustment of diabetes medications, which was based solely on HbA1c. A commercially available educational program (Accu-Chek EduCare; Roche Diagnostics, Monza, Italy) was used to provide standardized diabetes information on nutrition, physical activity, SMBG, and diabetes medications in both groups. For adjusting diabetes medications, investigators had the option to use a treatment algorithm 6 based on guidelines from international and national scientific societies. 9
Two validated questionnaires were administered at baseline and after 12 months of intervention to assess the psychosocial aspects of structured SMBG among PRISMA Study participants. The DSQoL questionnaire is a DSQoL questionnaire, a modified version of the diabetes quality of life questionnaire used in the DCCT, 10 which was translated in Italian and validated. 11 This questionnaire includes three domains: Satisfaction (satisfaction with the management of the disease, 14 questions, domain score from 14 to 70); Impact (impact of diabetes on life, 28 questions, domain score from 28 to 92); and Worry (worry about diabetes, 5 questions, domain score 5 to 25). Lowering the scores of any of the DSQoL domains indicates a shift toward a better quality of life.
The diabetes-specific LOC questionnaire, 12 translated into Italian, 13 includes three domains: Internal (the LOC lies within the patient); Powerful Others (i.e., either health professionals or nonmedical powerful individuals control patient's diabetes); and Chance (patient's diabetes is controlled by chance or fortune), each with a score 6 to 36: the domain with the highest score indicates the LOC of diabetes-related events, as perceived by the patient. Lowering the scores of the Powerful Others and Chance domains and increasing the scores of the Internal domain indicate a shift toward an internal LOC of diabetes.
Statistical analyses
Changes from baseline of the DSQoL and LOC scores after 12 months of intervention were analyzed on an intent-to-treat (ITT) basis, including all randomized patients. They were also analyzed in the per protocol (PP) population, consisting of all randomized patients who completed the study without major protocol violations and were compliant with the SMBG regimen (i.e., >80% of the required SMBG measurements in the ISM group and ∼200 unstructured discretionary SMBG measurements in the AC group, the maximum measurements recommended for these patients by the Italian Standards of diabetes care). 14
Statistical analyses were performed using change in DSQoL (Satisfaction, Impact, Worry) and LOC questionnaire (Internal, Powerful Others, Chance) domain scores from baseline as dependent variables. Initially, ANCOVA models with baseline scores as covariate and treatment group (ISM or AC) as dummy fixed effect were used to analyze data and to obtain univariate findings. Results are reported as least-square means with two-tailed 95% confidence intervals (CIs).
As an additional step, multiple linear regression models were performed using the basal score as covariate and treatment group (ISM or AC), gender, treatment at baseline (diet or diet+oral hypoglycemic agents), age, diabetes duration, and total number of glycemic measurements as independent predictors. Regression coefficients are reported in graphs as standardized estimates with two-tailed 95% CIs. Missing data have been imputed using maximum likelihood estimates (obtained through Expected Maximization algorithm or Multiple Imputation). SAS version 9.02, TS level 02M0, was used for all statistical computations. A two-sided test with a P-value ≤0.05 was considered statistically significant.
Results
Participants' flow and baseline characteristics have been reported elsewhere. 1 Of the 1024 eligible patients, 501 were randomized to the ISM group (49%) and 523 to the AC (51%) group. Overall, study participants were predominantly male (60%), obese (BMI ≥30), with a median age of ∼60 years, and with HbA1c median levels of 7.4% (57 mmol/mol) in the ISM group and 7.3% (56 mmol/mol) in the AC group.
Patients on diet only were 4.8% in the ISM group and 7.6% in the AC group. During the study, participants in the ISM group performed a median of 512 SMBG measurements, whereas patients in the AC group performed a median of 108 SMBG measurements. Two hundred participants in the ISM group (39.9%) and 98 in the AC group (18.7%) were not compliant with the SMBG regimen, that is, they did perform <80% of the capillary glucose measurements required by the study protocol for the ISM group or >20% for the AC group.
Changes from baseline in DSQoL and LOC domain scores
The DSQoL and LOC scores at baseline and after 12 months of intervention are shown in Table 1 for participants in the ISM and AC groups. The scores for all three domains of the DSQoL questionnaire were lower at the end of the study compared with baseline, indicating an improvement in quality of life, although with no significant between-group differences.
Basal values are reported as mean ± standard deviation, while changes from basal and differences are reported as least-square mean ± standard error.
AC, active control; DSQoL, diabetes-specific quality of life; ISM, intensive structured monitoring; LOC, locus of control.
The scores for the Chance and Powerful Others domains of the LOC questionnaire were lower at the end of the study compared with baseline, indicating that patients perceived that chance and other individuals were less important in the control of their diabetes. The between-group changes were significant for the Chance domain (P = 0.0309), indicating that patients in the ISM group were less likely to attribute the control of their diabetes to chance or fortune than those in the AC group.
Similar results were reported in the Practical ITT (data not shown) and in the PP analysis (Supplementary Table S1; Supplementary Data are available online at
The same trends were also observed when the analysis of the LOC domain scores was repeated in the other two datasets (Practical ITT, PP). Notably, in the PP dataset, the decrement from baseline values in the Chance domain was even larger in the ISM group (−1.28 at 12 months vs. baseline) and between-group difference was still significant (P = 0.05) (Supplementary Table S1).
Predictors of changes from baseline in the score of each DSQoL and LOC domain
Predictors of changes from baseline in the scores of each DSQoL (Fig. 1) and LOC (Fig. 2) domain are shown. An improvement in the Satisfaction domain score, that is, lower scores at the end of the study, was associated with higher number of SMBG measurements performed during the study (P = 0.007), older age (P = 0.013), and male sex (P = 0.0133). An improvement in the Worry domain score was associated with male sex (P < 0.0001), whereas no independent predictors of changes from baseline were observed for the Impact domain.
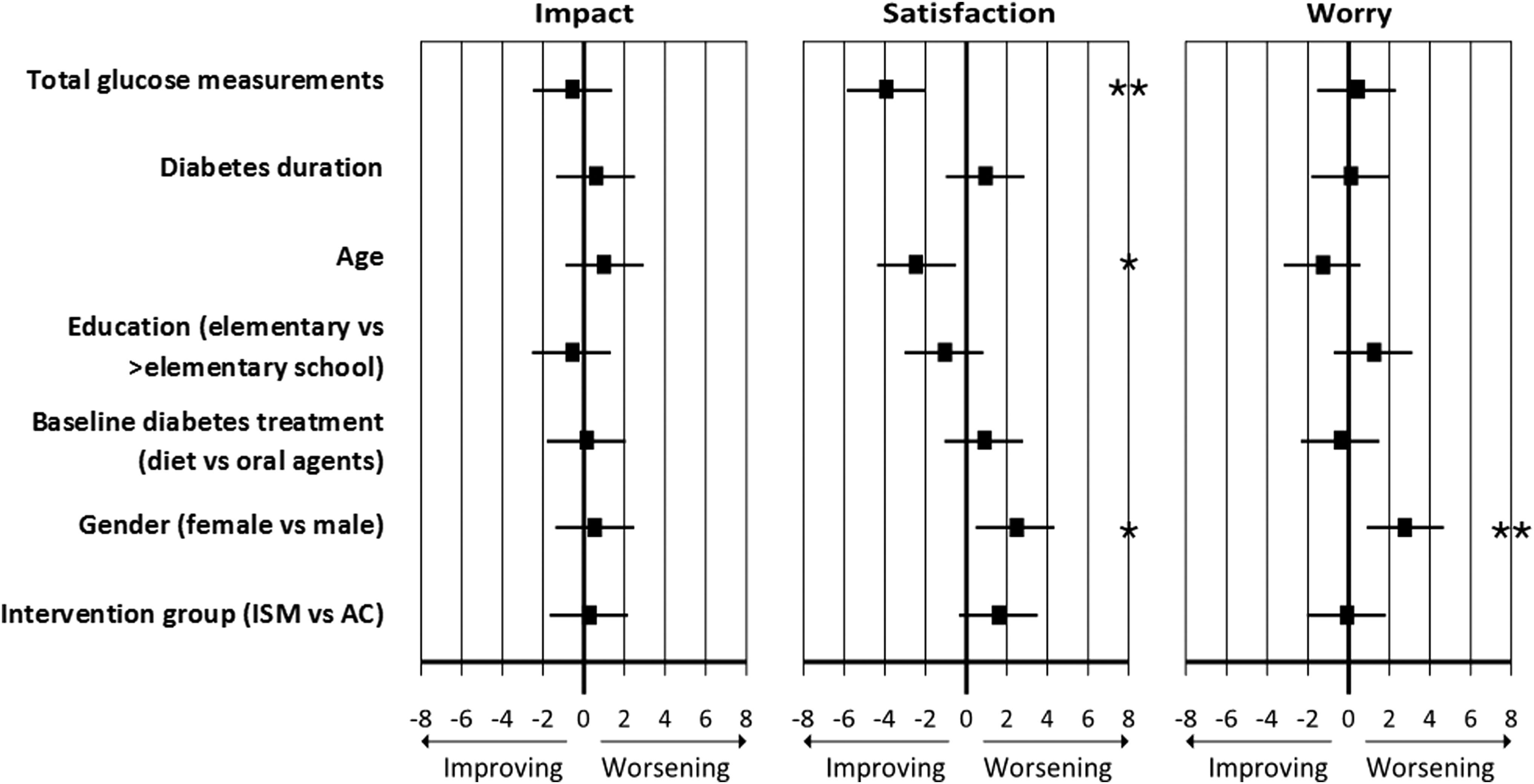
Standardized estimates (black squares) and 95% CI (horizontal lines) for the predictors of each diabetes-specific quality of life domain score among PRISMA Study participants. *P < 0.02; **P < 0.005. CI, confidence interval.
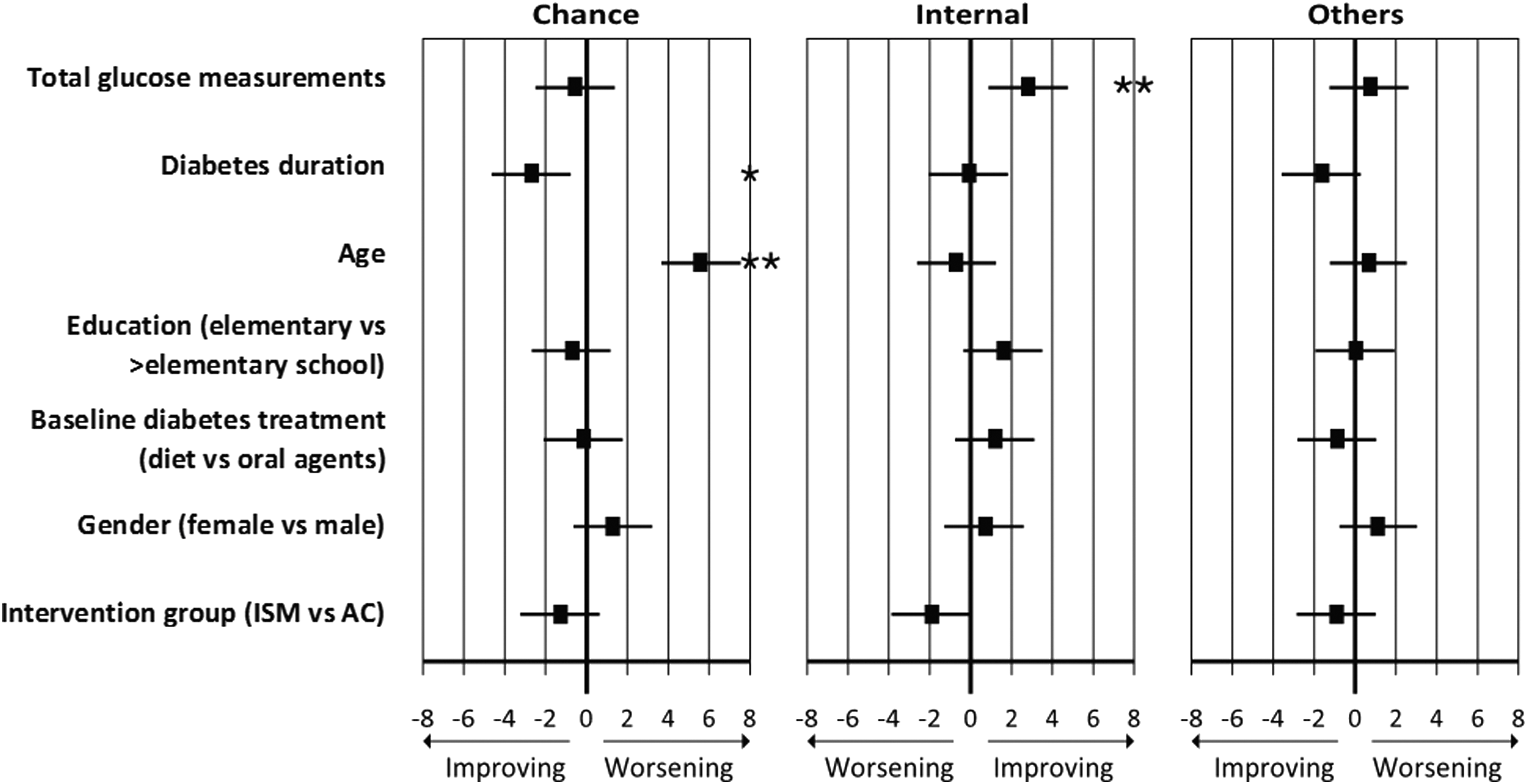
Standardized estimates (black squares) and 95% CI (horizontal lines) for the predictors of each locus of control domain score among PRISMA Study participants. *P < 0.01; **P < 0.004.
Lower scores for the Chance domain after 12 months of intervention, indicating a lesser role attributed to chance or fortune in the control of diabetes, were associated with longer diabetes duration (P = 0.0084) and younger age (P < 0.0001). An increase in the Internal domain scores, indicating an improved perception of personal control over the disease, was associated with the total number of SMBG measurements performed during the study (P = 0.0036), with the intervention group close to being significant (P = 0.06). As for the Powerful Others domain, indicating the attributed importance of other people (health professionals or nonmedical persons) in diabetes control, no independent predictors of change were identified, with diabetes duration close to being significant (P = 0.09).
Discussion
Our analysis showed that demographics and selected diabetes-related variables are significant predictors of the changes in DSQoL and LOC domain scores during the PRISMA Study. In the PRISMA Study main report, we documented that the efficacy of a structured SMBG on HbA1c in patients with noninsulin-treated type 2 diabetes 1 was not accompanied by deterioration in DSQoL or perceived control over the disease. This more detailed analysis of the PRISMA Study psychosocial data expands our previous observations: satisfaction about the management of the disease, impact on patients' life, and worry about diabetes showed significantly lower scores after 12 months of intervention, indicating an overall improvement of DSQoL overtime, although with no significant differences between intervention groups.
The impact of SMBG on DSQoL is still a disputed issue, especially in patients with noninsulin-treated type 2 diabetes. In a large cross-sectional Italian survey in patients with noninsulin-treated type 2 diabetes, 4 a more frequent SMBG was associated with higher levels of distress, worries, and depressive symptoms. However, this study only questioned participants about the frequency of SMBG and involved also patients under general practitioners' care, probably not adequately educated on interpreting the results of structured SMBG.
To date, only few prospective studies have addressed the impact of SMBG on QoL in noninsulin-treated patients. Findings from these studies have been inconsistent because of different study designs, including SMBG modalities, study population, and setting (general practitioners or diabetes specialists, nurses, etc.). 15
Among these studies, the ROSSO-in-praxi trial 16 demonstrated that addition of SMBG to a 12-week lifestyle intervention was associated with significant improvements in QoL in insulin-naive patients with type 2 diabetes mellitus, and the 2-year follow-up of a subset of participants showed the persistence of this improvement over time. 17 The STeP trial, a 12-month, two-arm, cluster randomized trial, tested a combination of structured SMBG data and data management software in 483 insulin-naive patients with type 2 diabetes and found that structured SMBG was associated with improved self-confidence and autonomous motivation in diabetes management. 18
Conversely, the DIGEM 19 and ESMON 20 trials failed to find any benefit of SMBG on QoL in patients with noninsulin-treated type 2 diabetes, whereas other two SMBG intervention studies, the St. Carlos trial 21 and the ROSES, 22 did not include QoL among their outcomes.
In a systematic review and meta-analysis of the relevant trials, although not including the most recent studies, the presence of worst outcomes in terms of QoL in patients regularly performing SMBG was interpreted in the context of a lack of diabetes education, which may have negative psychological effects. 23
On the contrary, intervention studies where structured SMBG was combined with education led to different results. Thus, prospective trials, such as the STeP 18 and the DESMON trials, 24 and recent reports by Muchmore et al. 25 and Schwedes et al. 26 showed that structured SMBG was associated with better or similar QoL measures than those observed in the control group, even when comparing SMBG vs. urine self-monitoring or usual care. 27
Our data are well in line with these reports, expanding the beneficial effects of SMBG and demonstrating that they are not limited to HbA1c, but could well be extended to DSQoL. At the end of the study, Satisfaction and Worry domain scores improved both in the ISM and AC groups, but these improvements were more evident in the ISM group. These results confirm that despite the high demand on patients of a more intense SMBG regimen, when capillary glucose measurement is integrated in an appropriate education program, the overall effect on DSQoL is at least neutral if not advantageous.
The improvement in DSQoL scores with SMBG is concomitant with similar changes in the LOC questionnaires scores. The highest domain scores indicate who/what the patient perceives as being in control of his/her diabetes. In our analysis, both the control attributed to chance and to others (people) decreased after 12 months of intervention, indicating patients perceived to be less dependent on surrounding factors for the control of their diabetes. Furthermore, the improvements in the Chance domain were more evident in the ISM group, indicating that structured SMBG may indeed increase the awareness of patients of their own role in managing diabetes.
These latter results are important when considering that one of the major goals of diabetes education is to empower patients to actively manage their disease, that is, to shift patients' belief that their diabetes is under the control of chance or other people to the feeling that they have a major role in the treatment process.
To date, only a handful of studies have examined the role of SMBG on LOC questionnaire results, and high Chance domain scores have been associated with diabetes-related negative outcomes, 28 including poor glucose control 29 and both physical and mental QoL. 30 However, other authors have shown no relationship between LOC or QoL and HbA1c levels. 31,32
Of course, SMBG may not be the only factor influencing QoL in patients with diabetes. Our results showed that both demographic and diabetes-related factors, such as age, sex, and diabetes duration, may play a relevant role. A recent Italian study on a large cohort of patients with type 1 diabetes 33 showed that worst DSQoL scores were independently associated with female sex, older age at onset, and lower schooling, in addition to higher fasting plasma glucose, severe hypoglycemia over the last year, and lower number of outpatient visits, concluding that the impact of type 1 diabetes on DSQoL may also depend on demographic and diabetes-related variables.
Our data suggest that these same factors may strongly influence changes in QoL overtime also in patients with noninsulin-treated type 2 diabetes. In our study, female patients showed worst DSQoL scores in the Satisfaction and Worry domains. Several hypotheses may explain the relative vulnerability of the female gender, including the documented lack of time for self-care in women with diabetes, which is thought to contribute to their worst outcomes. 34
Notably, although elderly are more exposed to comorbidities, polypharmacy, depression, and frailty, 35,36 in our analysis, Satisfaction and Worry DSQoL scores improved with aging, indicating that older subjects may cope better with the burden of diabetes. Although prior studies on this topic have yielded conflicting results, 37 –39 a recent retrospective analysis of a large pharmacy claims database found that greater adherence to antidiabetic medications was also associated with older age and male sex. 40
A possible explanation for these results may be that (unlike what is observed in women) older patients have more time to care for their diabetes. Furthermore, the less stringent glucose targets usually defined in older subjects according to standard guidelines may provide more freedom in the management of the disease, lightening its burden.
For patients with diabetes, integrating diet, exercise, medications, and glucose monitoring in everyday life is a true and often unappreciated challenge. Since a good QoL is the ultimate goal when treating chronic diseases such as diabetes, every single element of care, which may have an impact on QoL, should be carefully weighed in terms of its risks/benefits ratio, including SMBG. 41,42
In conclusion, our analysis of the PRISMA Study psychosocial data shows that in noninsulin-treated patients with type 2 diabetes, structured SMBG is not associated with a deterioration of quality of life and that demographic and selected diabetes-related variables are significant predictors of the changes in DSQoL and LOC domain scores associated with SMBG: these findings should be taken into consideration when tailoring educational support to structured SMBG for these patients.
Footnotes
Acknowledgments
This study was supported by Roche Diagnostics Diabetes Care. The sponsor contributed to the design of the study and provided funding for the conduct of the study, collection, management, and analysis of the data. The authors thank the investigators, trial staff, and participants (see ![]() ). Clinical trial reg. no. NCT00643474,
). Clinical trial reg. no. NCT00643474,
Authors' Contributions
G.T.R. researched data and prepared the first draft of the manuscript. M.S. conducted an independent statistical analysis of the data and prepared the first draft of the manuscript. E.B. conducted an independent statistical analysis of the data. E.B., F.G, E.A., and A.T. contributed to study design and critically reviewed the manuscript. D.C. contributed to study design, researched data, and prepared the final draft of the manuscript. All authors participated in reviewing and interpreting the data, in planning post hoc analyses, and in revising the manuscript. D.C. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Author Disclosure Statement
E.B. served on the PRISMA Study Advisory Board and serves on the Advisory Board for Roche and Abbott. M.S., A.C., D.C., A.T., and F.G. served on the PRISMA Study Advisory Board. E.B. served as statistical consultant for Roche Diagnostics Diabetes Care. E.A. is an employee of Roche Diagnostics Diabetes Care.
Appendix: PRISMA Study Participating Centers (Site,Principal Investigator,and Collaborators)
Unit of Diabetology, Ospedali Riuniti di Bergamo, Bergamo, Italy: Roberto Trevisan, MD, Alessandro Roberto Dodesini, MD, Anna Corsi, MD; Department of Endocrinolgy and Diabetes, “Felice Villa” Hospital, Mariano Comense, Italy: Luigi Sciangula, MD, Alessandra Ciucci, MD, Emanuela Simona Olivo, MA; Endocrinology and Metabolism Unit, University Hospital of Udine, Udine, Italy: Laura Tonutti, MD, Clara Boscariol, MA, Marina Armellini, Dietitian PhD; University Campus Bio‐Medico, Roma, Italy: Paolo Pozzilli, MD, Anna Rita Maurizi, MD, Silvia Manfrini, MD, Nicola Napoli, MD, Dario Tuccinardi, MD; Diabetology, UCSC Policlinicico A. Gemelli, Roma, Italy: Giovanni Ghirlanda, MD, Lucilla Gagliardi, MD, Loredana Ranalli, MA; University of Messina, Messina, Italy: Domenico Cucinotta, MD, Simona Zaccuri, MD, Letterio Giorgianni, Dietitian PhD; University of Padua, Department of Medicine, Division of Metabolic Diseases, Italy: Antonio Tiengo, MD, Gabriella Guarnieri, MD; Diabetes Clinic, Department of Digestive and Metabolic Diseases, Ravenna Local Health Unit, Ravenna, Italy: Paolo Di Bartolo, MD, Francesca Pellicano, MD, Patrizia Scolozzi, MA; Sandro Pertini Hospital, Unit of Dietology, Diabetology and Metabolic Diseases, Roma, Italy: Sergio Leotta, MD, Lucia Fontana, MD; San Giovanni di Dio Hospital, Diabetology Unit, Olbia, Italy: Giancarlo Tonolo, MD, Sara Cherchi, Nutritionist PhD, Lucia Canu, MA; Fermo Hospital, Diabetology Unit, Italy: Paolo Foglini, MD, Rossana Maricotti, MA, Elena Tortato, MD; San Raffaele Hospital, Diabetes Research Institute, Milan, Italy: Emanuele Bosi, MD, Cecilia Pianti, MD, Sara Madaschi, MD; Diabetes Center, Monfalcone, Italy: Carla Tortul, MD, Roberto Da Ros, MD, Raimonda Muraro, Dietitian PhD; Hospital of Alessandria, Division of Endocrinology and Metabolism, Alessandria, Italy: Egle Ansaldi, MD, Serena Cacciola, Dietitian PhD; University Hospital of Foggia, Division of Endocrinology and Metabolism, Foggia, Italy: Mauro Cignarelli, MD, Olga Lamacchia, MD; Morgagni Hospital, Endocrinology and Metabolism Unit, Forlì, Italy: Maurizio Nizzoli, MD, Lisa Buci, MD; ASL Salerno, Italy: Pasqualino Calatola, MD, Gennaro Clemente, MD, Alessandra Caputo, MA; S.M. Maddalena Hospital, Department of Internal Medicine, Diabetes and Metabolic Disease Unit, Rovigo, Italy: Francesco Mollo, MD, Gemma Friogato, MD; Fatebenefratelli Hospital, Diabetes Centre, Milan, Italy: Pietro Amatore Rampini, MD, Paola Morpurgo, MD, Giacomo Bonino, MA; Aldo Moro University, Department of Emergency and Organ Transplantation, Section of Internal Medicine, Endocrinology and Metabolic Diseases, Bari, Italy: Francesco Giorgino, MD, Maria Grazia Vita, MD, Luigi Laviola, MD; Magna Gaecia University, Department of Clinical and Experimental Medicine, Catanzaro, Italy: Agostino Gnasso, MD, Claudio Carallo, MD, Marilena Calabria, MD; San Bassano Hospital, Bassano del Grappa, Vicenza, Italy: Giampietro Beltramello, MD, Alberto Marangoni, MD; ASL3, Villa Scassi, Genova, Italy: Anna Cattaneo, MD, Roberta Guido, MD; U.O. Diabetes, Lanusei, Italy: Albino Massidda, MD, Gisella Meloni, MD; Niguarda Ca’ Granda Hospital, Milano, Italy: Matteo Andrea Bonomo, MD, Gianluigi Pizzi, MD, Mariangela Camerini, MA; Division of Diabetology, Partinico, Italy: Vincenzo Provenzano, MD, Lidia Ferrara, MD, Francesca Provenzano, MD; Health Care Management of the Local Health Authority, ULSS 9, Treviso, Italy: AgostinoPaccagnella, MD, Maria Sambataro, MD, Barbara Almoto, MD; University of Cagliari, Department of Medical Science, Endocrinology and Diabetes Unit, Cagliari, Italy: Marco Giorgio Baroni, MD, Efisio Cossu, MD, Anita Zedde, MD; University G. D'Annunzio, Chieti, Italy: Agostino Consoli, MD, Patrizia Di Fulvio, MD; University of Siena, Diabetes Unit, Siena, Italy: Francesco Dotta, MD, Elisa Guarino, MD; Federico II University, Department of Clinical and Experimental Medicine, Napoli, Italy: Giovanni Annuzzi, MD, Lutgarda Bozzetto, MD PhD; Diabetes Unit, Terni, Italy: Giovanni Cicioni MD; Misericordia and Dolce Hospital, department of Diabetes and metabolism, Prato, Italy: Maria Calabrese, MD, Sandra Guizzotti, RN; ASL of Cagliari, Diabetology Unit, Quartu Sant'Elena, Italy: Francesco Cabasino, MD, Fernando Farci, MD, Mariangela Ghiani, MD; San Camillo Forlanini Hospital, Diabetes Unit, Roma, Italy: Caludio Tubili, MD, Maria Rosaria Nardone, MD; ASS1 Triestina, Diabetes Center, Trieste, Italy: Riccardo Candido, MD, Elisabetta Tommasi, MA, Giuseppe Jagodnik, MA; San Bartolo Hospital, Metabolic and Endocrinology Unit, Vicenza, Italy: MarcoStrazzabosco, MD, Chiara Alberta Mesturino, MD; University of Perugia, Department of Internal Medicine, Perugia, Italy: Fausto Santeusanio, MD, Elisabetta Torlone, MD, Silvia Annone, MD.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.