
Abstract
Background:
Single- and dual-hormone closed-loop systems can improve glycemic control and have the potential to reduce carbohydrate-counting burden for patients with type 1 diabetes; however, simplification of meal insulin calculation should not compromise glycemic control.
Methods:
We compared in a randomized outpatient pilot trial: (1) a single-hormone closed-loop system accompanied with carbohydrate-content matched boluses versus accompanied with a simplified meal bolus strategy, and (2) a dual-hormone closed-loop system accompanied with carbohydrate-content matched boluses versus accompanied with a simplified meal bolus strategy. Carbohydrate-matched boluses were based on the participant's carbohydrate meal content estimation whereas the simplified strategy involved the selection, by participants, of a semi-quantitative meal carbohydrate-content size: snack, regular, large, or very large meal. Each participant also underwent sensor-augmented pump therapy. Basal insulin delivery was more aggressive with the simplified bolus. The primary outcome was mean sensor glucose level over a 15-h daytime period.
Results:
Twelve participants were recruited (48.2 ± 16.0 years old; HbA1c 7.4% ± 0.9%) to compare the two bolus strategies during single- and dual-hormone closed-loop delivery. A similar mean sensor glucose level (15 h) was achieved with the carbohydrate-matched boluses and simplified strategy using single-hormone (median [interquartile]: 7.6 [7.2–8.1] vs. 8.0 [7.0–8.6] mmol/L; P = 0.90) and dual-hormone closed-loop systems (7.6 [6.7–9.1] vs. 7.0 [6.4–8.2] mmol/L; P = 0.08). Exploratory analyses showed that, as compared with sensor-augmented pump therapy, there was an increased time spent in hypoglycemia with the simplified strategy but not with the carbohydrate-matched boluses.
Conclusions:
Though the algorithm employed in this pilot study may lead to an increased risk for hypoglycemia, this strategy has the potential to reduce the carbohydrate-counting burden in patients with type 1 diabetes while generally maintaining adequate glucose control. Longer outpatient studies with an improved algorithm are needed.
Introduction
T
Carbohydrate counting is an important aspect of type 1 diabetes treatment, and its accuracy is associated with better glycemic control. 4,6,7 However, accurate carbohydrate counting remains a challenging task for many patients with type 1 diabetes. A study showed that the average error remains ∼15 g per meal, representing 21% of the meal's content. 8 These errors were associated with increased glucose fluctuations. 8 Another study also showed that overemphasis on carbohydrate counting in patients' teaching could negatively influence their dietary choices, leading them to limit their consumption of carbohydrate-rich foods such as fruits and starches to avoid difficulties encountered with carbohydrate counting. 9 These studies suggest that patients could benefit from a system or strategy whereby the emphasis on precision of carbohydrate counting would be reduced. In addition, recent studies have suggested that carbohydrate type (glycemic index concept), protein, and lipid content of meals also impact the postprandial glucose control, adding to the complexity of meal insulin calculation for patients with diabetes. 10,11
The closed-loop strategy is a promising technology in which the subcutaneous infusion rate is modulated based on recommendations generated by an algorithm and relying on continuous glucose sensor readings. 12 Single-hormone (insulin only 13 ) and dual-hormone (insulin and glucagon 14 ) closed-loop systems have been proposed. Both versions improved glucose control when compared with conventional insulin therapy 12 –17 ; addition of glucagon infusion to insulin could further reduce the risk of hypoglycemia. 18,19
Although the simplification of meal boluses in the context of closed-loop strategy can reduce the carbohydrate-counting burden, this benefit should not be detrimental to glucose control. Several strategies have been proposed to simplify meal control during the closed-loop strategy such as the complete omission of prandial boluses or using partial prandial boluses based on body weight, total daily insulin, or insulin-to-carbohydrate ratio. Complete omission of prandial boluses resulted in prolonged hyperglycemia, 20,21 and the partial prandial bolus showed better glucose control. 20,22 –25 Limited data exist on comparing simplified meal boluses with the full carbohydrate-matched boluses. 24,25 We recently examined the efficacy of a simplified meal bolus strategy based on a semi-quantitative assessment of the meal carbohydrate content compared with carbohydrate-matched boluses in regulating glucose levels after three meals in adults with type 1 diabetes. 24 The simplified boluses yielded similar mean glucose and time spent in target compared with the carbohydrate-matched boluses. However, greater postprandial glycemic excursion was observed with the simplified strategy after a large carbohydrate content meal. 24
No attempt has yet been made to simplify meal boluses using the single-hormone closed-loop system. Moreover, no study has examined in outpatient conditions whether a partial prandial bolus could achieve acceptable glucose control when compared with carbohydrate-matched boluses using either single- or dual-hormone closed-loop strategies. Examination of the partial bolus in outpatient settings allows testing the strategy in a more complex context where carbohydrate-counting errors are likely to be more frequent. 8 During in-patient studies, carbohydrate counting was avoided by providing participants with the exact carbohydrate content of their meal. 24,25
The objective of the present study is to test in outpatient unrestricted settings whether, in the context of the closed-loop strategy, carbohydrate counting could be reduced by a simplified semi-quantitative meal carbohydrate-content size assessment without a significant degradation in overall glycemic control in adult patients with type 1 diabetes. We first compared the single-hormone closed-loop system accompanied with carbohydrate-content matched boluses versus accompanied with a simplified meal bolus strategy. We then compared the dual-hormone closed-loop system accompanied with carbohydrate-content matched boluses versus accompanied with a simplified meal bolus strategy. Participants also completed an intervention with sensor-augmented pump therapy accompanied with carbohydrate-content matched boluses for exploratory analyses.
Subjects and Methods
Study design
This pilot crossover study is an open-label, randomized, five-way study comparing the efficacy of single- and dual-hormone closed-loop systems combined with either conventional carbohydrate counting (carbohydrate-content matched boluses) or a simplified meal bolus strategy (semi-quantitative meal carbohydrate-content size assessment: snack, regular, large, or very large carbohydrate-content meal), and sensor-augmented pump therapy in regulating glucose levels in adults with type 1 diabetes. This pilot trial is registered as NCT02490098.
Study population
Participants were recruited and tested from May to October 2015 at the Institut de Recherches Cliniques de Montréal (IRCM), Montréal, Canada. Inclusion criteria were as follows: adults (≥18 years of age) with type 1 diabetes for >1 year, using insulin pump therapy for at least 3 months, and using carbohydrate counting for meal boluses. Participants with poor glucose control (glycated hemoglobin >10%), with clinically significant micro- (e.g., gastroparesis) or macrovascular complications or using medication likely to affect the results interpretation (e.g., agents affecting gastric emptying), were excluded. Other exclusion criteria were applied as detailed in the clinical trial registry. The IRCM ethics committee approved the study, and all participants provided informed written consent.
Study procedures
Before testing, all study participants completed a screening visit, including a medical exam, glycated hemoglobin testing, anthropometric measurements, and insulin therapy records examination. Usual average carbohydrate intakes were reviewed, and the simplified meal carbohydrate content estimation strategy was explained to the participants by a registered nutritionist. Participants were also taught how to install and use the continuous glucose monitoring systems (Dexcom G4 Platinum; Dexcom). Participants were asked to document their hypoglycemia and hyperglycemia thresholds to be used for all study interventions, and they were instructed to calibrate sensors at least twice daily using capillary blood glucose values.
Interventions were undertaken 1–5 days after sensor insertion. Interventions were conducted in outpatient settings and lasted 15 h. To ensure flexibility in matching their usual schedule, participants were allowed to begin the interventions between 6:00 and 8:00 and the interventions ended between 21:00 and 23:00. A research team member accompanied participants during closed-loop interventions to implement hormonal infusions. Subjects were allowed to eat whatever they wanted and were allowed to drink alcohol. They were, however, asked to consume a minimum of three meals during the day and they were asked not to eat before the beginning of interventions. Subjects were also allowed to exercise, but they were asked to perform a similar amount and as close to the same intensity of exercise on all intervention days. Interventions were separated by 0–30 days. In all interventions, the participant's usual fast-acting insulin analog was used.
In control testing, subjects used sensor-augmented pump therapy and freely implemented their usual basal rate and carbohydrate-matching full prandial bolus, including temporary basal and correction boluses, to regulate glucose levels as per their standard practice. Subjects had access to their finger-stick glucose measurements as well as to sensor values, and they were advised to measure their glucose level as per their standard practice.
In closed-loop interventions, variable subcutaneous insulin (single-hormone and dual-hormone closed-loop systems; Lispro, Aspart or Guilisine) and glucagon (dual-hormone closed-loop system only; Eli Lilly) infusion rates were used to regulate postprandial glucose levels by using one (single-hormone) or two (dual-hormone) infusion pumps (Accu-Check Combo; Roche). The glucose levels as measured by the real-time sensor were entered manually into a computer tablet every 10 min. The pumps' infusion rates were then changed manually, using a remote control device, based on the computer-generated recommendation infusion rates. The computer-generated recommendations were based on a predictive algorithm. The algorithm was a variant of the algorithm used in our previous studies 14,26 in which we increased the aggressiveness of meal boluses in all arms and the aggressiveness of basal delivery in the simplified bolus arm. The algorithm was initialized using body weight, daily insulin requirements, and insulin-to-carbohydrate ratios.
In the interventions where the closed-loop system was accompanied with a carbohydrate-matched bolus, prandial boluses were calculated using individualized insulin-to-carbohydrate ratios multiplied by the meal's carbohydrate content as evaluated by participants. Prandial boluses were also accompanied by correction boluses when glucose levels at the time of the meal were higher than 7.0 mmol/L. These prandial boluses were provided to the algorithm for calculation of postprandial basal insulin and glucagon boluses. In the interventions where the closed-loop system was accompanied with a simplified meal bolus strategy, prandial boluses were calculated based on semi-quantitative meal carbohydrate-content size assessment. Meal categories included snack (<30 g of carbohydrate), regular meal (30–60 g), large meal (60–90 g), and very large meal (>90 g). Prandial boluses were calculated as individualized insulin-to-carbohydrate ratios multiplied by a fixed factor for each category (snack = 15, regular meal = 35, large meal = 65, and very large meal = 95). For example, a participant with an insulin-to-carbohydrate ratio of 1 U for 10 g of carbohydrates who would consume 80 g of carbohydrates (large meal) would receive 6.5 U as a prandial bolus (bolus for a fixed factor of 65). Meal size assessments were provided to the algorithm for calculations of postprandial basal insulin and glucagon boluses. Participants selected a meal category during the interventions rather than counting the carbohydrate content of their meal. To avoid interference with the simplified strategy application, we decided not to ask participants to report the exact carbohydrate content of their meals with this strategy. In all cases, patients were instructed to give their insulin prandial boluses within 10 min before the beginning of the meal.
Outcomes
The endpoint for the primary comparisons was the mean glucose level over the study period (15 h) as measured by the glucose sensor. The following comparisons were done: (1) Single-hormone closed-loop system with a simplified meal bolus strategy versus single-hormone with carbohydrate-content matched boluses; (2) dual-hormone closed-loop system with a simplified meal bolus strategy versus dual-hormone with carbohydrate-content matched boluses. Secondary outcomes included mean glucose levels for all closed-loop strategies compared with sensor-augmented pump therapy, the percentage of time for which plasma glucose was (1) in the target range (4.00–10.00 mmol/L), (2) below the target range, or (3) above the target range, as well as the total amount of insulin and glucagon delivered. All comparisons between the closed-loop interventions and sensor-augmented pump therapy were secondary and for exploratory purposes, and, therefore, they do not require multiplicity adjustment. A block randomization, created by a third party unrelated to the project, was used to determine the order of the interventions.
Statistical analyses
Pairwise comparisons between the single-hormone and dual-hormone closed-loop systems with simplified boluses and with full boluses for our primary endpoint (mean glucose) were estimated from a linear mixed-effect model with treatment and starting glucose levels as fixed effects, and individuals as random effects. All pairwise comparisons for the secondary continuous outcomes were similarly estimated. Endpoints that did not respect normality assumptions were rank transformed. Data are presented as median [interquartile range] or mean ± standard deviation.
This is a pilot study, which recruited 13 participants to examine the feasibility and potential effectiveness of the simplified strategy in outpatient settings. This pilot study is not sufficiently powered for the primary outcome.
Results
Among the 13 participants recruited, one participant dropped out before the first intervention and thus only 12 participants completed the study and were included in the analysis (Fig. 1). Of the 12 participants, 10 completed all five interventions whereas two participants completed three interventions (noncompliance to protocol during the two remaining interventions for one participant, and no availability to complete the two remaining interventions for the other participant). Participants (50% men and 50% women) were 48.2 ± 16.0 years old with glycated hemoglobin of 7.4% ± 0.9% and duration of diabetes of 29.8 ± 16.6 years (Table 1).
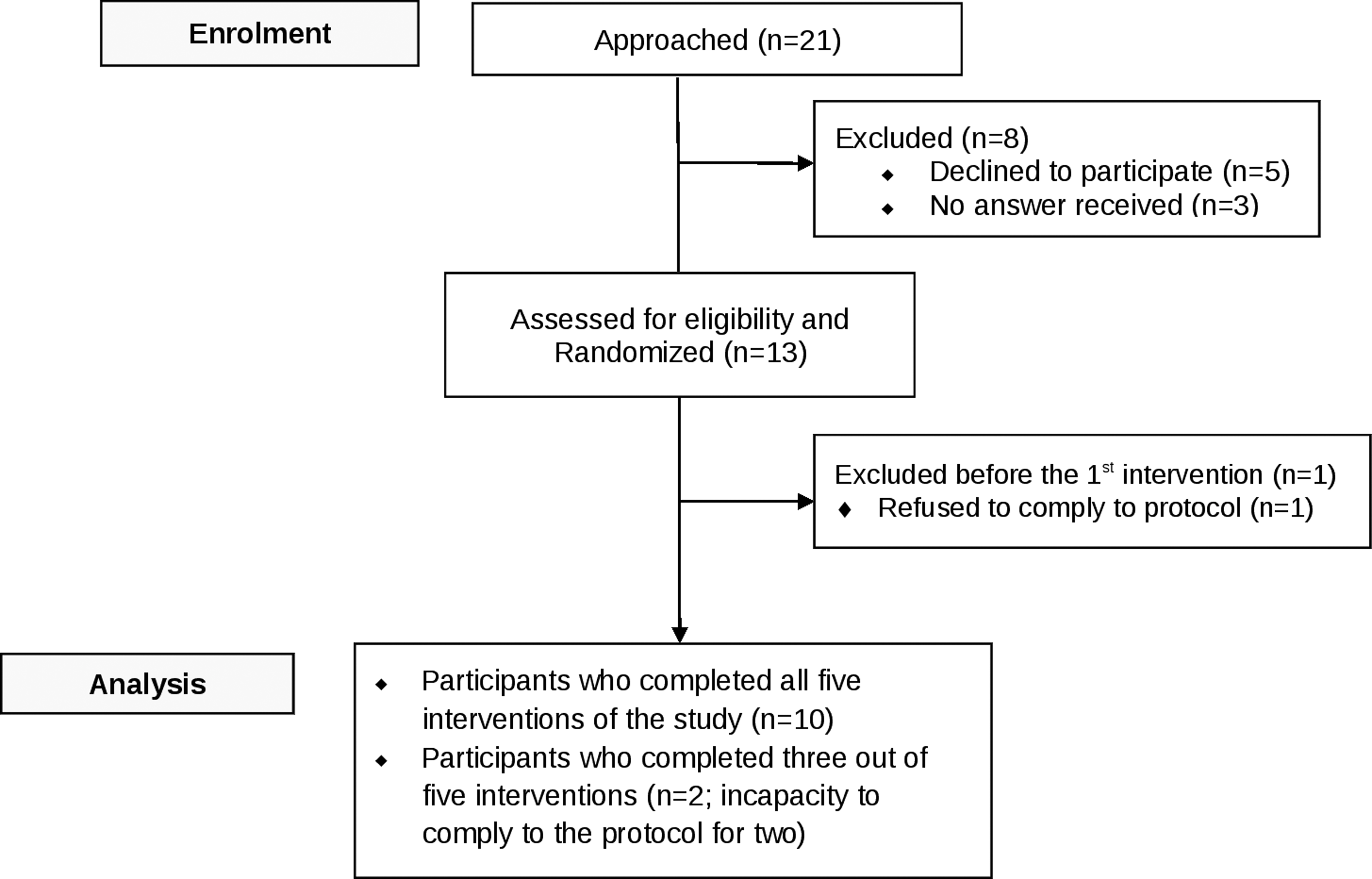
Flow of participants through the crossover study.
SD, standard deviation.
The primary comparisons examined the simplified meal bolus strategy and the carbohydrate-matched boluses in the context of single- and dual-hormone closed-loop systems. As shown in Table 2, no significant difference was observed between the two bolus strategies for mean sensor glucose level throughout the day (15-h period) for either the single- or the dual-hormone closed-loop systems (P = 0.90 and 0.08, respectively). As for the percentage of time spent in target range (4.0–10.0 mmol/L), no significant difference was observed between all closed-loop interventions (P > 0.05). The percentage of time spent above 10 mmol/L was also similar (P > 0.05) between the closed-loop interventions. Finally, the percentage of time in hypoglycemia (below 3.3 or below 4.0 mmol/L) did not differ between closed-loop interventions (P > 0.05).
Linear mixed-model analyses adjusted for starting plasma glucose.
Comparison between the two meal bolus strategies in single- and dual-hormone closed-loop systems for this outcome is the primary endpoint.
Significantly different (P ≤ 0.05) compared with sensor-augmented pump therapy (E).
In exploratory analyses, we compared the closed-loop strategies with sensor-augmented pump therapy (Table 2). First, when compared with this sensor-augmented pump therapy, the dual-hormone closed-loop system with the simplified bolus achieved lower mean glucose (7.0 mmol/L vs. 8.7 mmol/L; P = 0.007). A lower percentage of time spent >10 mmol/L was observed with the simplified bolus in both the single-hormone (20.7%) and the dual-hormone closed-loop systems (14.9%) when compared with sensor-augmented pump therapy (30.7%) (P = 0.05 and P = 0.01, respectively). Hyperglycemia occurred with sensor-augmented pump therapy in the late postprandial period throughout the whole day, whereas it mainly occurred in the morning postprandial period with the closed-loop strategies (Fig. 2). Single-hormone and dual-hormone closed-loop strategies with the simplified boluses also resulted in a higher percentage of time spent <4.0 mmol/L compared with sensor-augmented therapy (P = 0.05). No specific trend was observed for the timing for hypoglycemia, with the exception of the single-hormone closed-loop strategy with the simplified bolus for which hypoglycemia mainly occurred in the late-morning period (Fig. 2).
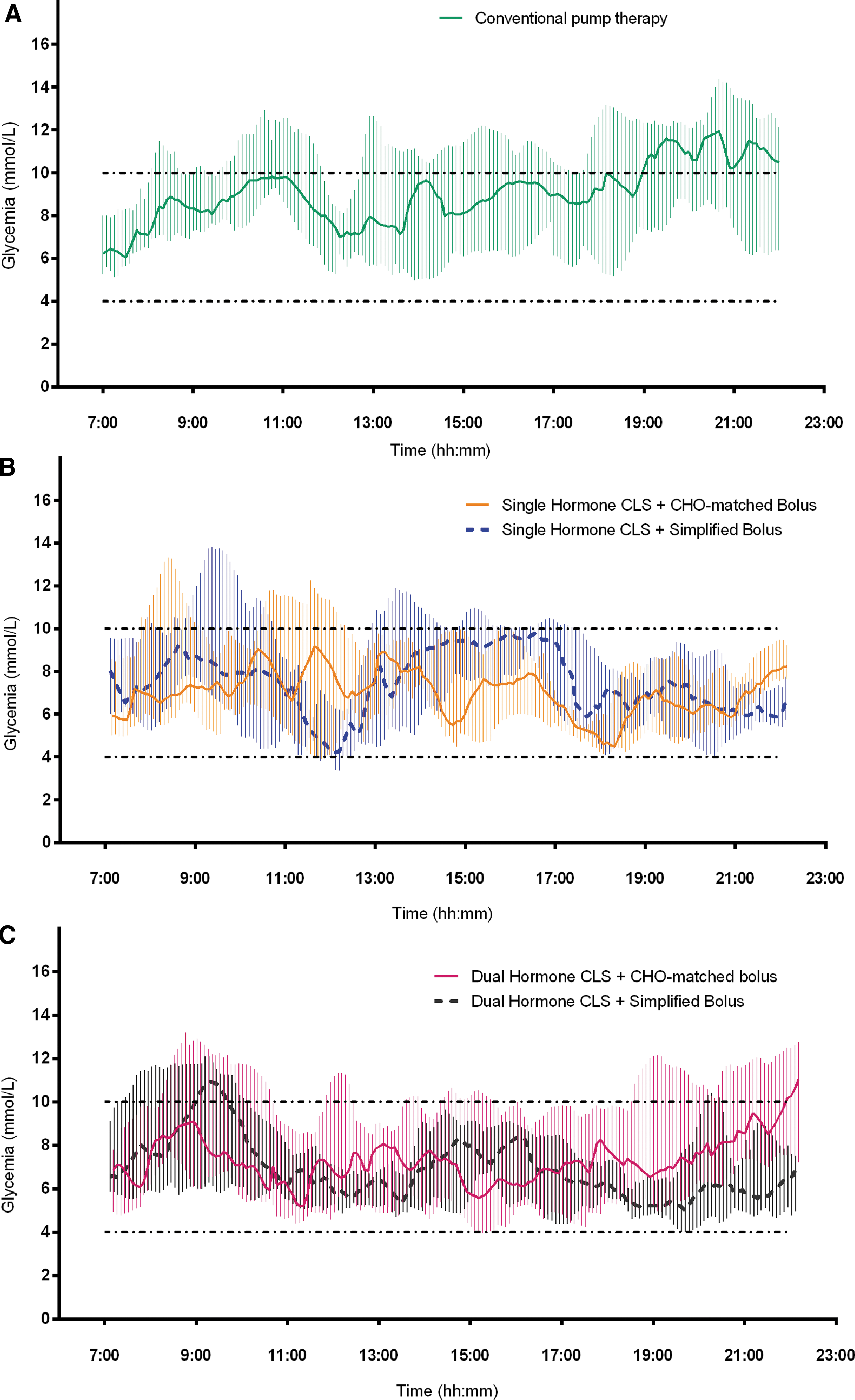
Profile (medians and interquartile ranges) of plasma glucose during sensor-augmented pump therapy
The amount of insulin delivery was similar through all interventions, including sensor-augmented pump therapy (P > 0.05; Table 2). In sensor-augmented pump therapy, three participants used additional correction boluses during the day whereas correction boluses were given by only one participant during each of the closed-loop interventions. The amount of glucagon delivery (Table 2) was also similar during both dual-hormone closed-loop interventions with carbohydrate-matched bolus (0.21 mg [0.16–0.30 mg]) and with the simplified bolus (0.25 mg [0.18–0.41 mg]; P = 0.28), with most of the glucagon delivered in the late postprandial period for both interventions. No adverse events related to glucagon boluses were reported by any patient throughout the study.
Discussion
In this pilot study, we examined whether similar glucose control could be achieved using the single- and dual-hormone closed-loop systems with a simplified meal insulin bolus based on the patient's insulin-to-carbohydrate ratio and a semi-quantitative meal carbohydrate-content size assessment compared with the standard carbohydrate-matched boluses used by participants. Similar glucose control was achieved with both the carbohydrate-matched and the simplified boluses using both closed-loop strategies as assessed by mean glucose and time spent in target range (4.0–10.0 mmol/L). Secondary exploratory analyses showed that the simplified strategy tended toward lower time spent in hyperglycemia due to aggressive insulin dosing, but at the same time also tended to increase time spent in hypoglycemia as compared with sensor-augmented pump therapy.
Several studies have investigated partial prandial bolus strategies in combination with the closed-loop strategy where body weight was generally used for prandial boluses calculations. 20,22,25 With a dual-hormone approach, the adaptive weight-based meal-priming bolus strategy tested by El-Khatib et al. 22 showed improvements in mean plasma glucose as compared with the absence of meal bolus. However, also with a dual-hormone approach, Haidar et al. 25 showed greater postbreakfast glucose excursions and time spent in hyperglycemia with a weight-dependent bolus compared with a carbohydrate-matched bolus. Exploratory analyses from this previous study 25 allowed us to determine that the participant's insulin-to-carbohydrate ratios were a strong determinant in the performance of the simplified boluses.
Using insulin-to-carbohydrate ratios rather than body weight preserves the ability of adapting insulin boluses for each individual's insulin sensitivity rather than assuming it is similar for subjects with the same body weight. Important variations in insulin sensitivity for a similar body weight are well described. 27 Such an approach also takes into account the variability of postprandial insulin requirements throughout the day. 28 We tested in a previous study the dual-hormone closed-loop system combined with a simplified meal bolus using two meal bolus categories, and we showed amelioration in glycemic control, with, however, greater postmeal excursions after large carbohydrate-content meals. 24 We, thus, adapted the strategy for the present study, adding a third meal carbohydrate-content size category for very large carbohydrate content meals and adding the snack category for small carbohydrate intakes. The strategy appeared to be effective for overall glucose control as well as for reduction of time spent in hyperglycemia.
As compared with other studies, 19,29,30 we observed a larger proportion of time spent in hypoglycemia with the closed-loop interventions, even with the use of glucagon. This is related to our attempt to use a more aggressive algorithm for both basal insulin delivery and prandial insulin boluses. Modifications in the insulin and/or glucagon aggressiveness of the algorithm are, thus, needed to minimize such hypoglycemic risk before proceeding to longer outpatient studies.
In addition to providing data on the performance of the simplified meal bolus strategy, the present study also provided information on the use of this system by participants in outpatient settings. None of the participants reported any difficulty in understanding the simplified meal bolus categorization during the closed-loop interventions. A registered nutritionist explained the strategy to participants during a brief (10–15 min) interview, suggesting an easy teaching process for patients already familiar with carbohydrate counting. Participants were also taught about how the closed-loop system works and during the interventions, they freely decided which meal category corresponded to their planned intake. Most participants gave boluses for each carbohydrate intake, although some participants decided not to bolus their snacks before exercise or not to give boluses for snacks in the context of normal-range blood glucose. These choices may have led to hyperglycemia on some occasions, due to the combination of food intake without bolus after prolonged insulin suspension and a glucagon bolus. Other participants administered insulin correction boluses for hyperglycemia: three participants for a total of three events in sensor-augmented pump therapy interventions versus five participants for a total of seven events in closed-loop interventions combined. The use of correction boluses with the closed-loop system would also have to be reviewed with participants to prevent hypoglycemic episodes due to insulin stacking. 31 Also, there was no instance of sensor failure requiring the return to usual conventional therapy during the interventions. Only minor sensor interruptions were observed (5–35 min), with one participant accidentally removing the sensor 85 min before the end of testing.
This study has some limitations. First, this is a pilot outpatient study with a small sample size. The objective was to compare the closed-loop strategies with carbohydrate-matched boluses and with simplified boluses in outpatient settings and to assess how participants would use the system. Although this study provided valuable insight on the performance of the simplified bolus, the statistical analyses need to be cautiously interpreted due to this small sample size. The algorithm design, which led to a higher percentage of time spent in hypoglycemia with the closed-loop strategies, is also a limitation, one that can be attenuated by either reverting to the aggressiveness of postmeal insulin delivery that we used in our previous studies 14,18,25,26,32 or increasing glucagon delivery. Also, manual control was used rather than automated control. 33,34 The presence of a team member with participants throughout the interventions might have affected their natural behavior. However, the clinical conclusions from this study are unlikely to be affected considering the conditions were the same for all the interventions for the primary comparisons. Manual control allowed avoiding technical difficulties in data transmission, and remote control allowed testing the algorithm with the simplified strategy in outpatient conditions that are close to free-living. We are also unable to evaluate whether our conclusions can be generalized to other artificial pancreas systems. Considering the specificity of each algorithm, the proposed strategy may not be suitable for all systems. Finally, considering the complexity of postprandial glucose excursions, other ways to simplify meal insulin doses should be investigated, including meal size estimation or the combination with anti-diabetic agents (alpha-glycosidase inhibitors, SGT2-Inhibitors, pramlintide, or glucagon-like peptide-1).
This is the first study that compared in an outpatient unrestricted setting both single- and dual-hormone closed-loop strategies with a carbohydrate-matched bolus and with an alternate simplified strategy aiming at reducing the carbohydrate-counting burden. The simplified strategy tested in this pilot study aimed at partially alleviating carbohydrate counting. With the aggressive algorithm employed in this study, the carbohydrate-counting burden was reduced without affecting mean glucose level or time spent in target range, but at the expense of increased risk of hypoglycemia. Longer outpatient studies with an improved algorithm are needed.
Footnotes
Acknowledgments
The authors are first grateful to all the participants of this study. They also thank Maryse Dallaire, Joanie Lupien, Mélanie Collin, Marie Devaux, Malalatiana Randriamanantena, and Jennifer Levasseur who provided nursing support. This work is supported by the J.A. DeSève Foundation to R.R.L. V.G. and R.R.L. are research scholars of FRQS (Fonds de Recherche du Québec en Santé). A.H. is a research scholar from the Canadian Institutes of Health Research (Banting Postdoctoral Fellowship).
Author Contributions
A.H., R.R.L., and L.L. co-designed the study. V.G. conducted the study. A.H. designed the dosing algorithm. V.G. carried out the data analysis and drafted the article. M.L. conducted the statistical analyses. V.M., A.H., and R.R.L. coordinated and supervised the study. All authors contributed to the interpretation of the results and the writing and critical review of the article. All authors approved the final version of the article.
Author Disclosure Statement
R.R.L. has received consultant/speaker honorariums and/or grants from Astra-Zeneca, Becton Dickinson, Bohringer, Eli Lilly, Janssen, Insulet, Lifescan, Medtronic, Merck, Novartis, Neomed, Novo-Nordisk, Roche, Sanofi-Aventis, Takeda, and Valeant. A.H., L.L., V.M., and R.R.L. own IPs in the area of artificial pancreas. No other competing financial interests were reported.