
Abstract
Background:
Little research exists regarding how real-time continuous glucose monitoring (RT-CGM) data sharing plays a role in the relationship between patients and their care partners.
Objective:
To (1) identify the benefits and challenges related to RT-CGM data sharing from the patient and care partner perspective and (2) to explore the number and type of individuals who share and follow RT-CGM data.
Methods:
This qualitative content analysis was conducted by examining publicly available blogs focused on RT-CGM and data sharing. A thematic analysis of blogs and associated comments was conducted.
Results:
A systematic appraisal of personal blogs examined 39 blogs with 206 corresponding comments. The results of the study provided insight about the benefits and challenges related to individuals with diabetes sharing their RT-CGM data with a care partner(s). The analysis resulted in three themes: (1) RT-CGM data sharing enhances feelings of safety, (2) the need to communicate boundaries to avoid judgment, and (3) choice about sharing and following RT-CGM data. RT-CGM data sharing occurred within dyads (n = 46), triads (n = 15), and tetrads (n = 2).
Conclusions:
Adults and children with type 1 diabetes and their care partners are empowered by the ability to share and follow RT-CGM data. Our findings suggest that RT-CGM data sharing between an individual with diabetes and their care partner can complicate relationships. Healthcare providers need to engage patients and care partners in discussions about best practices related to RT-CGM sharing and following to avoid frustrations within the relationship.
Introduction
M
New technologies, such as real-time continuous glucose monitors (RT-CGM), now have the capacity to involve close relationships in a more data-specific manner. RT-CGM first came to market in a way such that only the individual with diabetes could view their blood sugars using a receiver they carried with them; care partners could not visualize the data unless they viewed the individual's RT-CGM receiver. Advances in RT-CGM technology has resulted in a data sharing function to allow others within one's network (i.e., parents, romantic partners, friends, healthcare workers) to access the RT-CGM data. Through this advancement, care partners can receive RT-CGM data on mobile phones. The first platform to share RT-CGM data with care partners was the non-FDA-approved Nightscout in 2014. 6 FDA-approved Dexcom® (G4 PLATINUM System with Share and G5 Mobile CGM system) and MiniMed® (Connect App) platforms followed in 2014 and 2015.
Little is known about whom individuals with T1D share RT-CGM data or how sharing affects relationships between individuals with T1D and their care partner(s). Based on the social relationships literature, it is likely that children would choose to share data with their parents, whereas adults are inclined to share data with their romantic partner. 7 There is evidence indicating that RT-CGM without data sharing positively affects glycemic control and enhances physical and psychological wellbeing. 8 Patients and care partners alike mention that RT-CGM provides a sense of security, especially when engaging in high-risk activities, such as driving as well as when experiencing hypoglycemic episodes during sleep 8 and can support collaborative diabetes management and increase spousal engagement in diabetes care. 9 However, it can also lead to conflict, especially when coupled with a caregiver's lack of understanding regarding what actions to take when alarms occur. Currently, there are no clinical guidelines in how to involve care partners in RT-CGM data sharing.
In the digital age, individuals with diabetes and their care partners have opportunities to share their thoughts and feelings related to health within the diabetes online community. 10 Examination of online platforms, such as personal blogs, is one way to explore how patients and care partners view RT-CGM data sharing. Thus, we decided to explore the uniquely patient-centric personal blogs within the diabetes online community. The purpose of this research was to (1) identify the benefits and challenges related to RT-CGM data sharing from the patient and care partner perspective and (2) to explore the number and type of individuals who share and follow RT-CGM data.
Methods
Sampling
The study was acknowledged by the University of Utah Institutional Review Board as being exempt. To analyze relationship interactions, benefits, and challenges related to RT-CGM data sharing, a systematic appraisal of publicly available personal blogs was completed. This systematic appraisal included assessment of trustworthiness (Did each blog site have at least 10 other blog posts that were specific to diabetes?), value (Is the patient and/or care partner's perspective clearly described?), and relevance (Was the blog clearly focused on the research objective?).
Personal blogs were identified by searching Google and consulting with experts in the diabetes online community. The first 10 pages of each database search in Google were reviewed for the presence of blogs. Several search terms were used, including: continuous glucose monitoring OR CGM OR sensor AND share AND blog; Dexcom share OR Dexcom g4 with share OR Dexcom g5 OR CGM in the cloud OR Medtronic AND blog. Furthermore, experts in the diabetes online community located blogs based on their knowledge of the community and shared them with our research team for review. Blogs were chosen for inclusion if they met the following inclusion criteria: (1) written by a patient or care partner (i.e., parent, spouse), (2) focused on the personal experience of RT-CGM use and data sharing, (3) written in English, and (4) published between 2014 and 2017. We used the cutoff of 2014 because RT-CGM data sharing did not exist before that year. Blogs focused on RT-CGM were omitted if they did not mention both data sharing and a personal experience using this technology. Forums were omitted because they do not always provide the rich information that personal blogs can provide.
Our search strategy yielded 833 website records requiring screening. Eligibility assessment and systematic appraisal was performed independently by two reviewers. Disagreements between reviewers were resolved by consensus, and are noted in Figure 1. We developed a data extraction sheet, pilot tested it with 12 blogs, and refined it as needed. Initially, website records were reviewed to remove websites that were not blogs. Blog duplicates were then removed. Blogs were then further screened to remove types of blogs that were not personal blogs (i.e., health news blogs, organization blogs, etc.). A final screen and systematic apparaisal was conducted to include only personal blogs from the view of the patient or care partner that indicated a personal experience with RT-CGM and data sharing. There were 39 blogs with 206 corresponding comments in the final analysis. The search was conducted between February 2017 and April 2017.
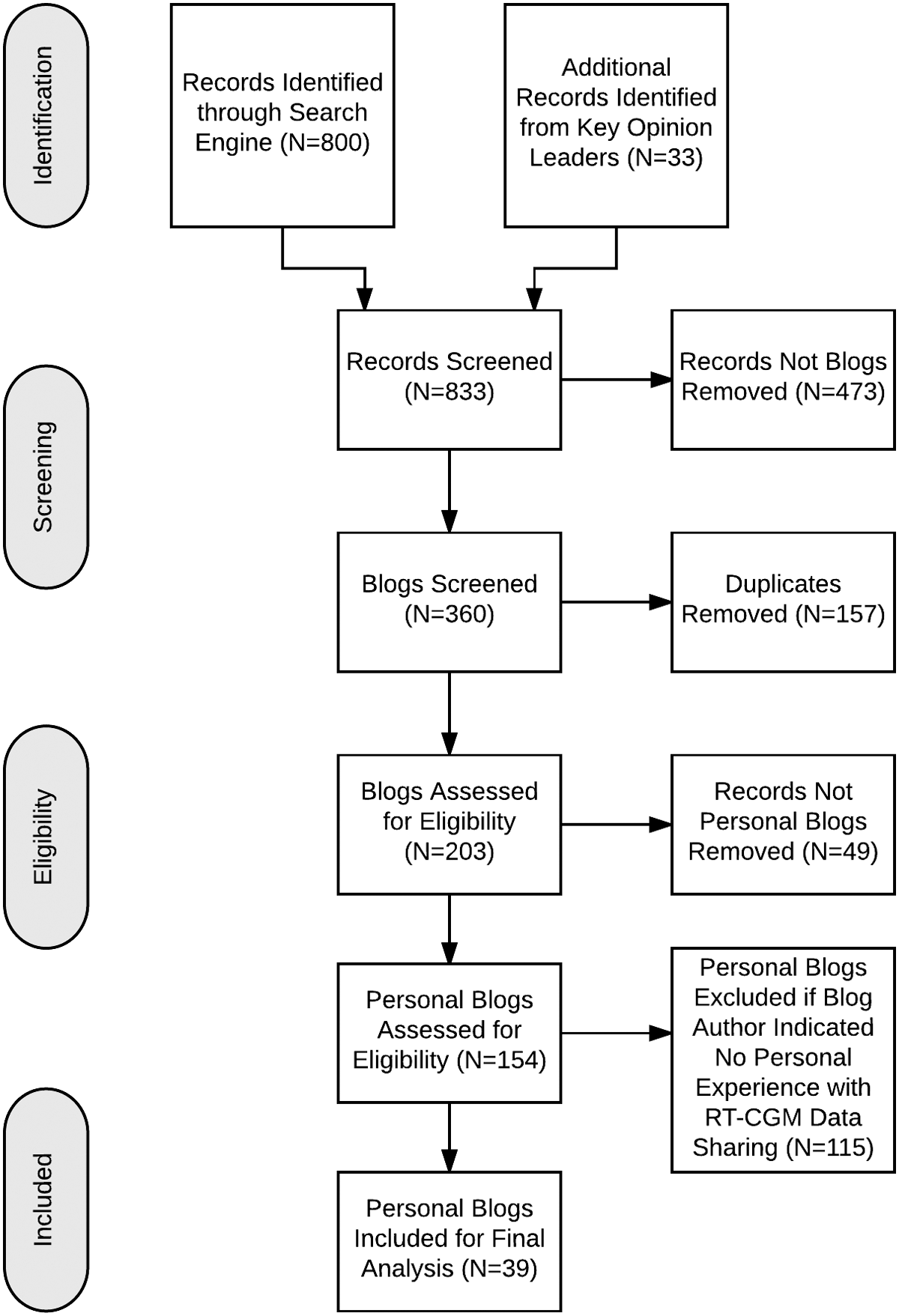
Process for inclusion and exclusion of blogs.
Data analysis
A qualitative content analysis of blogs and associated comments was conducted. Using this approach, we used a consistent set of codes to organize similar data. 11 Blogs were initially read by two independent investigators. The coding template was created after reading the first five blogs to generate an initially coding template by one of the investigators (M.L.L.). A second investigator (N.A.A.) reviewed the codes and coded data to establish credibility. There was 100% agreement on codes and categories, but disagreement on thematic emphasis. Through discussion, we reached consensus.
The codes were systematically applied to the remaining blogs by using an open code approach, which allowed for capture of any additional codes that may have been previously missed. 11,12 A coding process was performed with an audit trail. 13 Coded data was then used to develop corresponding themes. 14 RT-CGM sharing between patient and care partner(s) were categorized by type, resulting in two groups. The first group included adults with diabetes who shared their RT-CGM data with a care partner. The second group were parents who were following their child/children's RT-CGM data. Repetitive data emerged, and no new codes emerged by the 13th blog, indicating data saturation. However, data from all 39 blogs were included in this study.
Results
In this study, the person/individuals selected to receive RT-CGM data will be referred to as care partners. This study examined 39 blogs with 206 corresponding comments. Blog length, without comments, averaged 1184 words (range 205–5699). Twenty-two of the 39 blogs were authored by individuals living with diabetes, 16 were authored by parents, and one was authored by a spouse. RT-CGM data sharing occurred within six different types of dyads (n = 46) (Table 1). There were six different types of triads (n = 15) in which two categories existed, (1) “share”—a patient sharing with two different care partners, and (2) “follow”—a care partner following two people in the family with T1D (Table 2). There were also two different types of tetrads (n = 2) (Table 3), and an outlier category which included one physician who was following multiple patients who were using RT-CGM.
T1D = type 1 diabetes.
“Share”—a patient sharing with two different care partners. “Follow”—a care partner following two people in the family with T1D.
The results of the study provided insight about the benefits and challenges related to individuals with diabetes sharing their RT-CGM data with a care partner(s). Data were broken into two groups for analysis: first, adults with diabetes and their care partners; and second, children with diabetes and their parent care partners. The analysis resulted in three themes: (1) RT-CGM data sharing enhances feelings of safety, (2) the need to communicate boundaries to avoid judgment, and (3) choice about sharing and following RT-CGM data (Table 4).
RT-CGM = real-time continuous glucose monitoring.
RT-CGM data sharing enhances feelings of safety
Adults with diabetes and care partners
Individuals with T1D felt a peace of mind knowing that their care partners could view their RT-CGM data anytime during the day, providing a safety net, even when there was distance between them (i.e., traveling for business). Most individuals with T1D expressed interest in RT-CGM data sharing for hypoglycemia alerts, especially during the night. One representative quote includes: “I share my numbers with my husband who works varying shifts, including many overnights. With two younger kids at home, I feel exponentially safer knowing he can see where I'm at in case of emergency. He called me one evening after 3 unanswered texts, it may have saved my life.” Care partners felt that RT-CGM enhanced their ability to protect their loved one with T1D. One person with T1D noted the following after a discussion with her husband:
He had tears in his eyes telling me what it means to him that he can now keep me safer. I didn't set the share alarm to alert him if my blood sugar dropped too low, not wanting to unnecessarily burden him. He set it for himself. He said, ‘I can better protect you now.’ And I realize I do feel safer.
In many instances, care partners only had alerts set for persistent hypoglycemia and were not alerted during hyperglycemia episodes. One person noted, “For me, I see [RT-CGM data sharing] as an additional insurance policy if I was to go unusually low. [My husband and daughter's] alerts are only for persistent lows.”
Feelings of safety related to RT-CGM data sharing allowed those with T1D to sleep better, knowing that someone else was watching over them. One person noted, “I slept better with my [RT-CGM] rigged up. [My husband] could see my data while I was sleeping, and his system would alert him to any overnight hypos, should they occur. That's some good peace of mind for me when I'm a plane ride away from my support system.”
Children with diabetes and parent care partners
Parents felt that RT-CGM data sharing allowed them to disrupt their child less, while still having the ability to intervene if necessary. One parent noted, “this system gives us more freedom to let her be a kid,” whereas another parent noted, “I like that I can see a number and avoid the text or call to have them check blood sugars, I interrupt their lives less.” Overall, parent care partners noted that RT-CGM allowed them to step back and foster independence in their child.
Children and parent care partners in this study stated that with RT-CGM they felt safer allowing their child to engage in independent activities without interference, which in turn also enhanced the feelings of normalcy. These feelings of safety allowed children to feel more confident in engaging in their own independent activities. One parent stated, “We used to discuss a plan of ‘what ifs’ each time he went somewhere, now we are no longer thinking about it.” Another mother stated that her child, “no longer felt alone when getting dropped off for various activities.”
Several parents mentioned the ability to check in on their child at school or during the night also provided an enhanced feeling of safety and confidence in caring for their children. RT-CGM allowed for less burden on parents as well as more confidence and independence in their children with T1D. One parent noted, “This technology can help kids manage themselves with the safety net of someone else watching over them.”
Need to communicate boundaries
Adults with diabetes and care partners
Both individuals with T1D agreed that lack of communication could cause tension in the relationship. One care partner noted, “[RT-CGM Data Sharing] could be a recipe for hurt relationships and awkward interactions, with two individuals unsure about what they are supposed to do and when.” Another care partner described the importance of communication:
We don't want diabetes to dominate all our conversations. So, it's a balancing act. This is something all couples and probably families need to deal with when navigating this new world of streaming diabetes data. Technology only goes so far, but in the end, it's really about communicating with those important people in your life. We're partners in this game, so working together and sharing our feelings about all of this is so very important.
Those who had set boundaries before initiating RT-CGM data sharing spoke to their care partner about how and when they wanted to be contacted about a concerning low blood sugar. One person with T1D noted, “usually I advise them only to bug me for lows and for the most part tell them to ignore everything else.”
Individuals acknowledged that the act of sharing RT-CGM was an “intimate” experience. Both individuals with T1D and care partners described the importance of setting boundaries before establishing RT-CGM data sharing to avoid negative effects on the relationship. Individuals who had not developed boundaries with their care partner a priori felt like the loved one was “policing” their behavior and sometimes interacting in a way that was viewed as intrusive, resulting in frustration. There was a fine line between care partners being overbearing or critical and being supportive. One individual reported,
It's comforting to know someone else is “watching,” but at the same time I almost feel like [my wife] and I need to have a more in-depth talk about diabetes. When I go too low/high she will usually ask me why. At that point to me, it doesn't matter why I'm there, I just need to get out of it and I don't like feeling like I have to explain myself. I know it comes from a good place and she's only asking because she's worried about me.
Communication between the individual with T1D and their care partner(s) was also important throughout the RT-CGM data sharing process. When the person with T1D goes “offline” related to not wearing their sensor or they stop sharing their data, and do not communicate this to the care partner, this can increase care partner frustration and worry.
Children with diabetes and parent care partners
The parent care partner and child relationship was somewhat different than the adult and care partner relationship given the power imbalance. Some parent caregivers noted that their children with T1D felt that RT-CGM data sharing was too intrusive. One parent noted, “When my child started [RT-CGM data sharing] we did set up rules. I wouldn't text or call him unless it alerted a low of 70 or less or a high over 300 for more than 1 hour. Seems like pretty relaxed rules, right? Not really. Since I wouldn't have the data normally when he is away [without RT-CGM data sharing], in his mind, it is already more intrusive than he has ever had to deal with.”
To avoid appearing intrusive, some parent care partners strategically contacted their loved ones to see how they were generally doing, instead of focusing on glucose levels. One parent noted, “I do not contact [my daughter] unless I get a repeated low alarm, which will prompt me to text her with a question such as: Having a good day? or something generic like that. I do not check her number unless I get an alert. I think that would be too intrusive.”
Several parent care partners discussed the importance of talking with their kids about monitoring, especially with older children and teenagers. Specifically, some parents spoke about the undesired effects of constant streaming of data. One parent stated, “its important to establish how you're going to use [RT-CGM data sharing] together and come up with a plan. If both parents are constantly texting a kid that they are low or high, they are going to ‘burn out.’”
Choice about sharing and following RT-CGM data
Adults with diabetes and care partners
Individuals with T1D expressed the need to have power over whether or not they shared their RT-CGM data. The choice to share RT-CGM data related to several factors. Feelings of judgment, shame, or guilt motivated individuals to either share or not share CGM data. Some with T1D found themselves not wanting to feel that they had to explain every glucose number to their care partner, especially hyperglycemia. One individual with T1D noted, “I appreciate the option to share the data for my safety, but not for [care partner] scrutiny.” While another said, “The level of sharing that works for me on days when my blood sugar is 93 mg/dL and holding steady is very different than when I'm riding out a 288 mg/dL for four hours.”
Some individuals with T1D would only share if they felt they needed an additional “safety net” because they were experiencing activities outside of their norm, such as travel or illness. Once their situation normalized, they would turn the RT-CGM data sharing feature off. One individual with T1D said, “I live alone. If I'm not feeling well, or have had wild swings, I can ask my mom to watch via share. It puts both of our minds at ease. Most of the time I don't use it, but it's nice to have every once and a while!”
In some instances, patients would stop RT-CGM data sharing or threaten to, because of a strain in the relationship caused by RT-CGM data sharing. One caregiver noted, “[My husband] thought I was being annoying, but I was just concerned.” After we exchanged a few messages, the arrow and low reading still weren't changing and I asked if the CGM sensor was working correctly. He sent me a text, “That's it, I'm turning off Nightscout.”
Care partners who do not understand how to be helpful or are overwhelmed by the responsibility of having access to RT-CGM data may be more hesitant. One person with T1D commented, “My boyfriend did not want to see the CGM data, [rationalizing] ‘This is a lot of responsibility.’ It's not that he doesn't love me. He is just overwhelmed by the responsibility.”
Children with diabetes and parent care partners
Many parents expressed that the use of RT-CGM gave them a sense of freedom encouraged independence for themselves and their children. For example, one parent shared, “I can watch from the wings. This is pure joy for both of us.” Another shared, “there are times when I see something that he hasn't noticed yet and I will prompt him. I don't feel like I have taken back control though. I feel like I'm helping him at a level that is appropriate for someone his age. He's continued to move forward in his level of self-care.”
As children grow and develop independence, parent monitoring may cause conflict or resentment in the care partnership. One parent shared that she has heard kids tell their parents “you're stalking me.” Many parents shared that they compromise with their older children such that the parents will adjust settings to view only agreed-upon high and low alerts. Alternatively, some teens will choose to share with friends they trust. One parent noted, “my daughter shares her RT-CGM numbers with a new friend. This friend would occasionally see low blood sugar alerts and text my daughter to make sure she was doing something about it.”
Discussion
This is the first publication to our knowledge focused on how RT-CGM data are shared within close relationships. We were able to analyze information from two different perspectives, the adult with diabetes sharing with care partners and children with diabetes sharing with parent care partners. Our findings indicate that RT-CGM data sharing enhances feelings of safety among those with T1D and their care partners. In addition, individuals with T1D and care partners need to communicate boundaries in order for the individual with T1D to avoid feelings of judgment. Finally, these findings emphasize the importance of patient choice about when and when not to share RT-CGM data with their care partner.
Individuals with T1D are sharing their RT-CGM data to feel more safe from hypoglycemia events. Individuals with T1D may feel more vulnerable to hypoglycemia events when engaging in certain activities, such as travel, being alone at night, or caring for small children. Recommendations for insulin adjustments based on RT-CGM data have been established 15 and care partners may be able to assist with insulin or rapid-carbohdyrate decisions in times of need, especially parents. In this study, we identified various dyads, triads, and tetrads that were made up of several different types of care partners. RT-CGM data sharing did not exceed three care partners, despite the technology being able to support more. While sharing CGM data may decrease hypoglycemia risk, it cannot guarantee avoidance of serious hypoglycemia or emergency treatment.
Patients are empowered with RT-CGM data, however, data sharing can complicate relationships. Patients using RT-CGM can experience sensor inaccuracy and alarm fatigue 8 which may transfer to care partners when data sharing. RT-CGM without share may positively impact marital quality, however, sharing with appropriate collaborative diabetes management may also be beneficial. 9 Furthermore, if parents interact with their child's RT-CGM data in a controlling manner, it may disrupt feelings of self-efficacy, especially if the child is generally efficacious. 3 Similarly, when adult care partners exert control related to diabetes management it can create tension in the relationship. 16 Patient choice matters. Just because RT-CGM data sharing is available, it should not impose on the patient's choice on whether or not they want to include a care partner in their diabetes management.
Healthcare providers should engage patients and care partners in discussions about proper management strategies related to RT-CGM data sharing before care partners have access to the shared data to avoid frustrations and relationship tension. While there are no current professional recommendations on this topic, an example discussion guide, including eight talking points, related to RT-CGM data sharing with care partners exists within the blogosphere. 17 Based on the findings from this study, discussions about RT-CGM data sharing should include how care partners can (1) support safety by setting alarms and communicating with the person with T1D, (2) communicate effectively to avoid dialogs that could be perceived as judgmental or critical, and (3) open discussion about when RT-CGM data sharing should and should not occur based on dyad, triad, and tetrad agreement.
Patients and care partners typically need time to adjust to RT-CGM data, 18 and therefore may need ongoing support from healthcare providers to aid in proper management strategies. Interventions in family management strategies with respect to type 2 diabetes suggest that patients can be guided toward a more effective use of their family network for support for diabetes activities. 19
A systematic appraisal of blogs carries some limitations. It is difficult to determine age, type of CGM device and or platform (i.e., Nightscout) used, and other demographic data through an analysis of blogs. Open Artificial Pancreas System (OpenAPS) or CGM in the Cloud users may be more vocal due to a social learning process; however, we were unable to capture specific information about how many of our participants might identify with one of those groups. There were no postings that overtly indicated a patient with T1D as being an older adult. It is important to note that despite lack of access, there are older adults with T1D who are using RT-CGM, 20,21 although it is unknown how many older adults share their RT-CGM data with others. Importantly, older adults who are experiencing cognitive issues may especially benefit from RT-CGM and data sharing because they are at significantly increased risk for hospitalization and hypoglycemia. 22,23 Data extracted from blogs does not succumb to research bias, but may succumb to bias of the intended reader. Health blogs are typically viewed as anecdotal information, however, aggregated data collected from multiple health blogs can support empirical investigations. 24 –26
This study examined individuals who share their CGM data. Importantly, it must be noted that there is a subset of patients who have access to CGM sharing abilities, but do not for a number of reasons: (1) the patient or care partner may not have the technology supported on their mobile device, (2) there may be challenges with setting up the sharing features, (3) patients may not want to share their data due to privacy concerns, not wanting to include others in their care, or not seeing a clinically useful benefit, or (4) patients may identify with diabetes as being their own condition opposed to a shared condition. 27
In conclusion, this is the first study to examine the social context of sharing RT-CGM data. Patients with T1D and caregivers report that RT-CGM data sharing is beneficial in enhancing perceptions of safety, however, challenges do exist, such as tension in relationships, when communication about family engagement activities related to RT-CGM data sharing does not occur. We hypothesize that improved healthcare provider knowledge of this relationship tension and proactive discussions with patients and caregivers before starting RT-CGM share will improve the collaborative diabetes management experience, ultimately improving patient outcomes among those sharing RT-CGM data.
Footnotes
Author Disclosure Statement
No competing financial interests exist.