
Abstract
This study investigates the performance of an iteration of the Medtronic hybrid closed-loop (HCL) algorithm, which utilizes sensor glucose values non-adjunctively for bolus advice, recognizes sustained hyperglycemia, suggests insulin bolus correction, and includes more accommodative SmartGuard™ automode parameters that aim to improve function and usability. Adolescents aged 13–17 years with type 1 diabetes >1 year, glycated hemoglobin (HbA1c) 7.0%–10%, currently using Continuous Subcutaneous Insulin Infusion were randomized to the control Medtronic standard HCL algorithm or to the intervention Medtronic HCL with enhancements. Participants attended a 7-day and 7-night nonstructured camp setting. Twelve participants (mean age 15 years, seven males, five females, mean HbA1c 8.55%) completed the study. For the control group, time in target glucose sensor range (3.9–10 mmol/L) was 63.68% ± 10.74% at baseline and changed to 75.85% ± 8.49% during the study (relative Δ19%). Time spent in <2.8 mmol/L was 0.61% ± 0.79% at baseline for the control group and changed to 0.32% ± 0.31% during the study for the control group (relative Δ48%). In the intervention group, time in target glucose sensor range (3.9–10 mmol/L) was 52.15% ± 9.55% at baseline and changed to 74.32% ± 8.41% during the study (relative Δ42%). Time spent in <2.8 mmol/L was 1.07% ± 1.77% at baseline for the intervention group and changed to 0.24% ± 0.14% during the study for the intervention group (relative Δ78%). Mean sensor glucose was 8.05 ± 0.73 mmol/L and 8.22 ± 0.56 mmol/L for the control and intervention participants. SmartGuard automode exit frequency was 0.54 exits per person per day for control and 0.12 exits per person per day for the intervention. Participants were in active SmartGuard automode 97.1% and 98.8% of the time for the control and intervention, respectively. Alarm frequency was 2.1 alarms per person per day for the control arm, and 0.26 alarms per person per day in the intervention arm. Feasibility of the enhanced HCL algorithm was demonstrated with a high proportion of time spent in SmartGuard automode and target glucose range. The iterative changes resulted in less SmartGuard automode exits without compromising glycemic control.
Introduction
H
Full automation of all insulin delivery is constrained by present technology limits, particularly sensor glucose lag and insulin action time. Until these limits are overcome, emphasis on improving user experience is needed to facilitate translation of promising research findings into routine clinical practice. This user experience is dependent on both the education offered on how to maximize benefit (glycemic and quality of life) and also on the interaction between the technology and the user.
We aimed to explore the performance of an iteration of the Medtronic HCL algorithm in a camp setting with adolescents with type 1 diabetes. The research emphasis was on function and usability of the system and gathering data to help future study design.
Methods
Study design
An open-label, parallel-arm, randomized controlled trial for 7 days in a camp setting.
Subjects
Adolescents aged 13–17 years with type 1 diabetes >1-year duration, glycated hemoglobin (HbA1c) 7.0%–10%, and currently using insulin pump therapy >6 months were eligible. Participants were recruited as a convenience sample from the Princess Margaret Hospital (Western Australia) diabetes service. Exclusion criteria included pregnancy and an inability to adhere to study protocol requirements.
HCL systems
Participants were fitted with one of two Medtronic HCL systems. Both consisted of a Medtronic insulin pump and Guardian Sensor 3 and a Medtronic feedback control algorithm. The algorithm received continuous glucose monitoring (CGM) data every 5 min, which then automated “basal” insulin delivery. Meals were announced by the user, and an insulin bolus was delivered according to the individualized patient carbohydrate ratio and insulin sensitivity factor (should a correction bolus be required in addition to the insulin for carbohydrate).
The “intervention” HCL system included the following iterations: (1) a more aggressive correction bolus for hyperglycemia, (2) more accommodative parameters to remain in SmartGuard™ automode, (3) all meal bolused insulin from sensor glucose value (nonadjunctive), and (4) the “intervention” system suggested an insulin correction bolus in the setting sustained hyperglycemia and maximal insulin delivery calculated by the algorithm.
Study protocol
Seven days before the camp all participants were randomized to either control or intervention, fitted with the relevant HCL system including CGM, and trained how to use the pump in manual mode. Experienced CGM users were permitted to use CGM-based alarms if they were currently using this. Participants were instructed to use the pump at home in manual mode, and no effort was made by the investigators to optimize settings or improve glycemia. Participants then attended a camp for 7 days and nights. At the camp, each participant was housed in an independent unit, with a fully equipped kitchen. Food for breakfasts, lunches, and snacks was chosen by the participants and stored in their own rooms, allowing participants to eat what and when they liked. The evening meal was eaten communally. Daily activity was unstructured, and the participants had access to a swimming pool, bicycles, pedal carts, and the beach. The protocol included three planned challenges: a high-fat evening meal on day 5, 60 min of exercise on the morning of day 6, and an unannounced 70 g carbohydrate lunch on day 6.
The staff
Participant ratio was 1:3, with participants being physically sighted hourly during the day, and three hourly overnight. All meals were associated with a capillary blood glucose test (BGL) (before bolusing for the control arm and after bolusing for the intervention). Additional BGLs were taken before bed and once overnight at 3 am. Unscheduled BGL testing occurred when the HCL requested a capillary BGL value, or if the participant experienced hypoglycemia (by sensor <3.9 mmol/L or if symptomatic). Participants were requested to be in their own unit by 10:30 pm and lights out at 11 pm.
Outcomes
The study was an exploratory pilot study investigating the performance of the two iterative HCL algorithms. Usability outcomes were % time in SmartGuard automode, frequency of automode exits, frequency of device alarms, user satisfaction (internal user satisfaction survey provided by Medtronic), and sensor performance (median absolute relative difference, all paired samples during run-in and camp phase). Glycemic outcomes reported are based from a consensus statement on artificial pancreas study report, 2 and included sensor glucose values during camp, time in target range 4–10 mmmol/L (day and night), time hypoglycemic <2.8 mmol/L, <3.3 mmol/L, <3.9 mmol/L, and time spent hyperglycemic >10 mmol/L, >13.9 mmol/L, >16.7 mmol/L, average sensor glucose value, and sensor glucose variability. Glycemic data during the run-in period are provided.
Statistical methods
The study was exploratory, with the purpose of generating means and standard deviations (SDs) for future studies; therefore, no comparative analyses were planned. A study population n = 12 (n = 6 in each arm) was based on evidence that this is the optimal sample size for defining a confidence interval around the mean. 3 All raw data are presented with means, medians, and SDs as appropriate.
Results
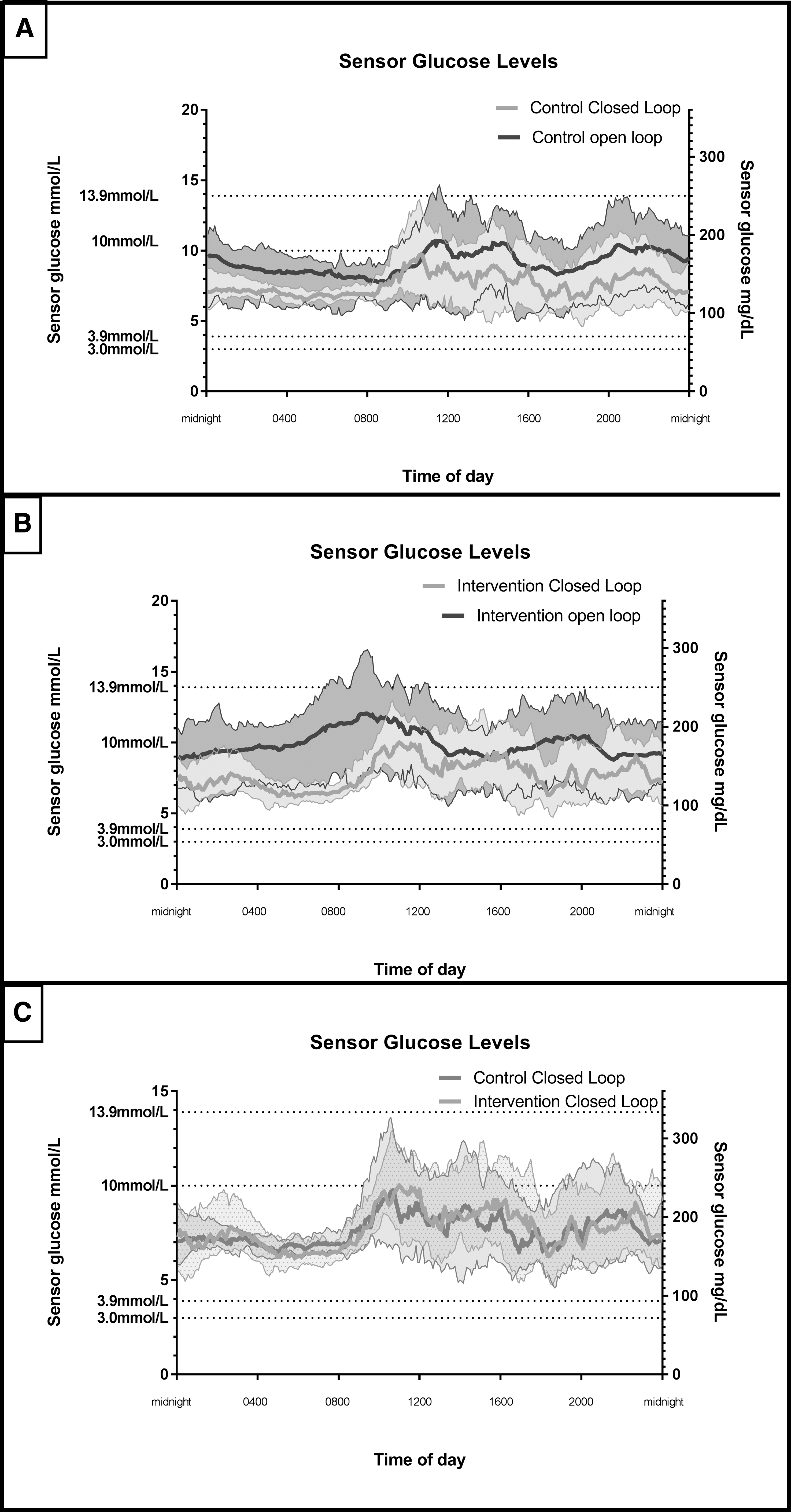
Twelve participants (mean age 15 years [range 13–17], seven males, five females, mean HbA1c of 8.55% [range 7.4%–9.6%]) were recruited and completed the study. All glycemic data and performance parameters are listed in Table 1 and illustrated in Figure 1. For the control arm, time in target glucose sensor range (3.9–10 mmol/L) was 63.68% ± 10.74% at baseline and changed to 75.85% ± 8.49% during the study (relative Δ19%). Time spent in <2.8 mmol/L was 0.61% ± 0.79% at baseline for the control arm and changed to 0.32% ± 0.31% during the study for the control arm (relative Δ48%). In the intervention arm, time in target glucose sensor range (3.9–10 mmol/L) was 52.15% ± 9.55% at baseline and changed to 74.32% ± 8.41% during the study (relative Δ42%). Time spent in <2.8 mmol/L was 1.07% ± 1.77% at baseline for the intervention arm and changed to 0.24% ± 0.14% during the study for the intervention arm (relative Δ78%). Overall, mean sensor glucose was 8.05 ± 0.73 mmol/L and 8.22 ± 0.56 mmol/L for the control and intervention participants during the camp phase. Overnight (0000–0600 h) the mean sensor glucose levels were 7.34 ± 0.34 mmol/L and 7.47 mmol/L for the control and intervention participants during the camp phase. Mean sensor glucose during the open-loop run-in was 9.11 ± 1.00 mmol/L and 9.83 ± 0.95 mmol/L for the participants randomized to control and intervention, respectively.
Median absolute relative difference was calculated by analyzing all observations in all participants and is expressed as median (interquartile range).
N/A; SD, standard deviation.
Measures of the HCL system usability are also described in Table 1. During the camp phase, the control system exited SmartGuard automode 23 times (0.54 exits per person per day), compared with five exits in the intervention arm (0.12 exits per person per day). Total alarms were 88 (2.1 alarms per person per day) for the control arm compared with 11 (0.26 alarms per person per day) in the intervention arm. Participants were in active SmartGuard automode 97.1% and 98.8% of the time for the control and intervention, respectively, reflecting quick intervention to return to SmartGuard automode in the control patients (usually by providing a capillary blood glucose value). The various reasons for alarms are described in Table 1. Sensor median absolute relative difference was 10.8%. Overall satisfaction was 83% for the control and 100% for the intervention.
Discussion
In this pilot study, we have shown that iterative improvements in the function of an established HCL system have the potential to enhance usability and efficacy. The intervention arm started with poorer glucose metrics in terms of time spent in target range during the run-in phase and demonstrated a greater improvement. In particular, the reduction in alarms is relevant to the patient experience, as alarm fatigue has been shown to be an important negative factor that decreases adherence to closed-loop systems. 4 Glycemic improvements due to technical advances are directly proportional to the time they are used, 5 and therefore, iterations that improve usability and adherence are likely to translate to improved glycemic measures with long-term use.
Glycemic data relating to time in range and hypoglycemia are comparable with various camp and outpatient studies previously published. 1 Our results are also consistent with the literature demonstrating that time in range is best overnight while using an automated insulin delivery system. 1
We acknowledge the limitations of this study: a small sample size only in adolescents, closely supervised setting, and short duration of follow-up, which is why statistical comparisons have not been made, and the results are not generalizable. Raw data during the open-loop phase and the camp study are provided to guide power calculations in future planned work and not intended to be used as a measure of effectiveness. Nevertheless, by conducting this study in a non-structured camp setting, a middle ground between long-term outpatient studies and tightly controlled in-clinic or in-silico studies is met. While long-term closed-loop studies currently underway are comprehensively assessing the efficacy and safety of today's technology, these data provide insight on the performance of iterations of HCL technical enhancements that can be incorporated into the HCL technologies of tomorrow.
We conclude that with even relatively minor adjustments to present closed-loop technology, the experimental arm had a greater magnitude of improvement both in clinical outcomes and patient experiences. We encourage that in the design of long-term studies investigating diabetes technologies, allowance is made to include iterative improvements in the technology and therefore contemporize the conclusions made as opposed to drawing conclusions based on technologies that have been made obsolete. 6
Footnotes
Acknowledgment
This is an investigator-led study. Hardware was provided by Medtronic through an unrestricted support agreement.
Author Disclosure Statement
No competing financial interest exists for M.D.B., J.D., M.H., G.S., E.D., and T.J.