
Abstract
Background:
The use of insulin pumps in pediatric patients with type 1 diabetes (T1D) has expanded; however, data comparing devices remain scarce. We compared glycemic control, technical difficulties, and quality of life (QOL) between pump devices of three companies.
Methods:
This prospective observational trial is based on clinical data retrieved during 12 months of follow-up of pediatric patients who started pump therapy as part of their clinical care in four medical centers. The devices fully reimbursed by the national health insurance are as follows: MiniMed™ 640G, MiniMed® Veo™, Animas® Vibe®, and Abbott OmniPod®. Parameters investigated included discontinuation rate, glycated hemoglobin (HbA1c), mean self-monitoring of blood glucose (SMBG), total daily dose of insulin (TDD), pump setting parameters, body mass index (BMI), frequency of technical difficulties, significant skin reactions, and QOL.
Results:
Of 113 children (mean age 9.1 ± 4.1 years, 46% females), 68 (60%) used Medtronic devices, 33 (29%) OmniPod, and 12 (11%) Animas devices. Twelve percent of the cohort stopped using the pump during the study period, with no difference according to device. There were no differences between groups regarding mean SMBG values (P = 0.86), insulin TDD (P = 0.24), BMI (P = 0.87), level of insertion site pain or local reaction (P = 0.51), technical problems (P = 0.66), and QOL (P = 0.38). Changes in HbA1c from study initiation to end were also not statistically significant for any of the devices: from 7.99% ± 1.14% to 7.93% ± 0.99% for Medtronic, from 7.71% ± 1.29% to 7.92% ± 1.38% for OmniPod, and from 8.75% ± 1.3% to 7.70% ± 1.33% for Animas (P = 0.63).
Conclusions:
Pump devices were comparable regarding glycemic control, weight gain, and satisfaction among pediatric patients with T1D.
Introduction
Since the introduction of continuous subcutaneous insulin infusion pump therapy in 1979, 1 this technology has been widely translated into pediatric practice, especially in the last decade. The goals of such implementation are improvement in glucose control and quality of life (QOL). 2 –6 In 2007, a joint consensus statement recommended that pump therapy be considered in children and adolescents with suboptimal diabetes control and wide fluctuations in blood glucose levels, and when the insulin regimen compromises lifestyle. 7
Pumps have since become widely used among type 1 diabetes (T1D) pediatric patients, with a reported percentage use of roughly 40%–60%. 2 –6 Due to the availability of several pump devices on the market, parents and children ponder as to the device that is optimal for them. Issues to consider are the efficiency, safety, and convenience of the devices.
Continuous insulin delivery is the hallmark of the pump; however, the specific insulin bolus and basal insulin delivery technologies differ; one is a patch device and the others use tubing for insulin delivery. They differ in size and weight, appearance, interface language, and water stability, as well as in their connections to continuous glucose monitoring (CGM) technology. The multiple features of each pump may influence device selection and satisfaction from the technology.
Interestingly, despite several years of experience, knowledge is lacking regarding pump selection, real-life practice of the various devices, and possible differences in glycemic control and patient experience. To date, studies comparing the various devices are sparse, 8 –11 and mainly focused on technical evaluation, including dose accuracy of basal intervals, 10 blood glucose and plasma insulin profiles after bolus insulin infusion, 11 short-term treatment satisfaction, and glycated hemoglobin (HbA1c) level. 9 Furthermore, a survey of 985 pump users from the United States and Germany demonstrated that only 47% were very satisfied with their current pump. 12
The Israeli basic health insurance covers full pump use for all T1D pediatric patients, with no preference between pumps of three companies (Insulet OmniPod®, Animas Vibe®, Medtronic Paradigm Veo and G640®), as well as CGM for all pediatric patients who experience severe hypoglycemic episodes. Thus, the objective of the current study was to compare glycemic control, compliance parameters, technical problems, and QOL between the pump devices of three companies, during the first year of pump use, among all new pediatric pump users at four medical centers.
Methods
Study design
This is a prospective observational real-life multicenter trial, based on clinical data retrieved as part of clinical care at each clinic visit during 12 months of follow-up, and conducted according to the principles of the Declaration of Helsinki on biomedical research involving human patients and the respective local national regulations (
Initiation of pump therapy and selection of the specific pump type were decided before and independent of study enrollment, and were based on the family's choice after presentation and explanation of all options by the diabetes teams (not by sales representatives). Those who chose Medtronic pumps, received G640 or VEO pumps according to availability in the country. During study period, the company stopped providing VEO. Patients who were enrolled in the study at the visit switched from multiple daily injections to the pump, after receiving all the pump equipment and instructions from the diabetes team regarding principles of care.
Pump settings were determined by the health care professionals according to patients' individual needs and were adjusted as required during clinic visits. Patients were invited for routine clinical visits every 3 months and received intensive diabetes management with the aim of achieving target glycemic control according to ISPAD guidelines. 13 Patients were followed prospectively for 1 year from pump initiation. They filled QOL assessment questionnaires and reported by questionnaire the frequency of technical difficulties, adverse events during use, number of sets used or disposed without appropriate use, and pain at insertion at the end of follow-up.
Study population
The study population comprised all individuals with T1D ages 0–20 years who switched management modality from multiple daily injections to the pump as part of their clinical care (pump naive), and who were managed by the pediatric diabetes teams from the AWeSoMe Study Group (four pediatric diabetes multidisciplinary clinics in Israel: Assaf Harofeh Medical Center, E. Wolfson Medical Center, Edmond and Lily Safra Children's Hospital, and Maccabi National Juvenile Diabetes Center). Patient eligibility criteria included the following: a diagnosis of T1D recorded by a pediatric endocrinologist, periodic attendance at clinic visits, and initiation of pump therapy between May 2015 and March 2017. There were no restrictions on HbA1c values at study recruitment or on the use of CGM. CGM fully reimbursed and used in Israel during study period included Dexcom G4 Platinum (Dexcom) and Medtronic MiniMed 640G (Medtronic Enlite).
Data collection
Variables recorded at the baseline visit were as follows: gender, age, diabetes duration, other medical problems, and educational and marital status of the parents. Variables recorded at each visit, including the baseline visit were HbA1c levels, as obtained with a DCA point of care device, episodes of diabetic ketoacidosis (DKA) (defined as blood pH <7.3 and the requirement of insulin infusion), and severe hypoglycemia (defined as glucose level <50 mg/dL and the inability to self-treat, requiring treatment by another person), height, weight, body mass index (BMI), (BMI-standard deviation score (SDS) and height SDS were calculated based on CDC 2000 growth charts), 14 and Tanner pubertal stage. 15
Glycemic control parameters, based on data from the 14 days before the clinic visit, included the mean number of self-monitoring of blood glucose (SMBG), mean ± standard deviation (SD) of glucose values by SMBG or by CGM, the mean total daily dose of insulin (TDD), and basal and bolus ratios that were downloaded at each visit using computerized programs (CareLink Therapy Management System for Diabetes-Clinical, Medtronic, Tolochenaz, Switzerland, CoPilot System, Abbott Diabetes Care, Inc., and Diasend® product, via
Questionnaires
QOL was assessed utilizing the Diabetes Treatment Satisfaction Questionnaires (DTSQ) for teens and for parents. 16 The teens' version of the DTSQ contained 12 items scored on a six-point scale, of which 9 were summed. The parents' version of the DTSQ contained 14 items, of which 9 were summed. The maximal score on both versions was 42.
All patients were asked five questions regarding monthly frequency of local reaction including local redness, itching, and swelling, technical problems including pump failure, tubing occlusions, and the need to use additional insertion sets due to “dumped” sets (sets that were disposed without full 3 days of use), and the level of pain at catheter insertion graded subjectively from 1 to 10.
Outcome measures
Primary outcome measures were differences in QOL, technical problems encountered while using the pump, skin reactions, and the discontinuation rate between users of the various pump devices during 12 months of follow-up. Secondary outcome measures were differences in glycemic control parameters and metabolic parameters after 3, 6, and 12 months of follow-up, between users of the various devices.
Statistical analysis
Categorical variables were described as frequencies and percentages. Continuous variables were assessed for normal distribution using histograms and Q-Q plots. Normally distributed continuous variables were described as mean and SD, and non-normally distributed parameters were described as medians and interquartile ranges (IQRs). The chi-square test and Fisher's exact test were used to evaluate differences in categorical variables between the three pump device groups. The Kruskal–Wallis test and Mann–Whitney test were used to assess differences in continuous variables between device groups. Linear regression was used to evaluate differences between pump device groups at baseline, after controlling for diabetes duration and CGM use.
The Generalized Estimating Equations (GEE) model was used to evaluate changes in each outcome during the follow-up period. An interaction between time and pump device was applied to evaluate differences between the pump types in changes occurring during the follow-up. Two-tailed P < 0.05 was considered a statically significant result. Data were analyzed with IBM SPSS Statistics for Windows, Version 23.0 (released in 2015).
Results
The study population comprised 113 children with T1D, mean age 9.1 ± 4.1 years, 46% females. Sixty-eight children (60.2%) used the MiniMed 640G insulin pump with SmartGuard (64 children) or the MiniMed Veo insulin pump (4 children) (Medtronic group), 33 children (29.2%) used the Abbott Diabetes Care OmniPod (OmniPod group) and 12 children (10.6%) used the Animas Vibe insulin pump (Animas group).
Comparison between those who continued and discontinued pump
In total, 14 children (12.4%) stopped using the insulin pump during the study period, with no statistically significant difference according to pump device: 9 children from the Medtronic group (13%), 2 children from the OmniPod group (6%), and 3 from the Animas group (25%), P = 0.21. Their characteristics are presented in Table 1. The children who stopped using the pump were older than those who continued (12.7 ± 3.5 years vs. 9.9 ± 4.3 years, P = 0.02), had longer duration of diabetes before pump initiation (2.0 ± 2.4 years vs. 1.1 ± 1.7 years, P = 0.04), and checked their glucose level less frequently (5.1 ± 2.5 vs. 6.5 ± 2.3 SMBG per day, P = 0.05). No differences were observed between the groups in gender, age at diagnosis, HbA1c level, insulin TDD, or in characteristics related to housing conditions. Interestingly, all those who discontinued pump use had diabetes for longer than 3 months, and none was using a CGM system before pump initiation. The children who stopped using the pump were excluded from further statistical analysis.
Baseline Characteristics of Constant Insulin Pump Users and Pump Discontinuers
Values are mean ± SD for parameters with normal distribution and median with IQR in cases of nonlinear distribution.
Other diseases, including celiac and hypothyroidism.
Newly diagnosed—diagnosed within 3 months before pump initiation.
SMBG—retrieved from 3- to 6-month visits before initiation.
BMI, body mass index; CGM, continuous glucose monitoring; HbA1c, glycated hemoglobin; IQR, interquartile range; SD, standard deviation; SDS, standard deviation score; SMBG, self-monitoring of blood glucose; TDD, total daily dose of insulin.
Consistent pump users' analysis
The median follow-up for the 99 study participants who continued pump use during the 1-year study period was 1.02 (0.81, 1.11) years. Use of a CGM device was the only characteristic examined that differed between the pump device groups (Table 2). A higher proportion, 9/31, of those who chose the OmniPod were already using a CGM device; this compares with 4/59 of Medtronic pump users (P = 0.009) and none of the Animas pump users (P = 0.01). In total, 16 patients were with newly diagnosed diabetes (<3 months duration): 4/31 of the OmniPod group, 9/59 of the Medtronic group, and 3/9 of the Animas group (P = 0.26).
Baseline Characteristics of Constant Pump Users According to Device Type
Values are mean ± SD for parameters with normal distribution and median with IQR in cases of nonlinear distribution.
Other diseases, including celiac, hypothyroidism, psoriasis, and asthma.
Newly diagnosed—diagnosed within 3 months before pump initiation.
SMBG—retrieved from 3- to 6-month visits before initiation.
After 12 months of follow-up, a total of 48 participants (48.5%) used CGM: 23/59 of Medtronic users used Medtronic Enlite, 17/31 of OmniPod pump users, and 8/9 of Animas pump users used Dexcom. The proportion of CGM among Animas users was significantly higher than that of Medtronic users, and similar to that of OmniPod users (P = 0.009, P = 0.23 at 6 months and P = 0.01, P = 0.22 at 12 months, respectively). The proportion of CGM among OmniPod users was also significantly higher than that of Medtronic users at 6 months but not at 12 months (P = 0.04 at 6 months and P = 0.07 at 12 months).
Complications and technical problems
No significant differences were demonstrated between the three pump devices regarding frequency of short-term disease complications (severe hypoglycemia, DKA, hospitalization, significant local reactions at insertion site), the number of disposable equipment used during a month, and the number of “dumped” sets, which were unused for 3 days due to defects or use failure (Table 3). Patients using an Animas device graded pain at insertion as significantly lower than did those using Medtronic devices (P = 0.005). However, this difference became nonsignificant when a regression analysis was performed using diabetes duration as a possible modifier. No significant difference was found between the pain reported by OmniPod and Medtronic device users (P = 0.08) and between OmniPod and Animas device users (P = 0.31).
Short-Term Complications and Technical Problems According to Pump Devicea
Data regarding hypoglycemia, hospitalization, or DKA were collected from medical charts. Data regarding skin reactions, local pain, and sets used and “dumped” (sets that were disposed without full 3 days of use) were collected from questionnaires.
The patients graded the pain during the insertion (score 1–10). Animas users graded pain at insertion as significantly lower than did Medtronic users (P = 0.005), with no significant difference between OmniPod and Medtronic (0.08) and between OmniPod and Animas users (0.31). The difference became nonsignificant when a regression analysis was performed, using diabetes duration as a possible modifier.
During the full follow-up period.
DKA, diabetic ketoacidosis.
Quality of life
Eighty participating families (80.8% of consistent users) filled the DTSQ at the end of the follow-up period, including 67% of the OmniPod users, 88% of Medtronic users, and 78% of Animas users. No difference was detected in satisfaction level among parents according to pump device: median (range) scores of 38.0 (33.0, 39.5), 37.5 (34.5, 41.0), and 40 (36.0, 42.0), P = 0.38, respectively; nor among children: 36.0 (31.2, 40.3), 38 (34.0, 41.0), and 41 (36, 42), respectively, P = 0.17.
Glycemic control
The GEE model was applied to assess differences between pumps over time, regarding definitions of bolus calculations, insulin TDD, HbA1c, mean glucose and SD of glucose, number of SMBG per day, and BMI-SDS. Analysis was controlled for the duration of time from T1D diagnosis to pump initiation. No statistically significant differences were found in any of the parameters examined over time (Fig. 1). HbA1c at initiation and end was 7.99% ± 1.14% and 7.93% ± 0.99% for Medtronic, 7.71% ± 1.29% and 7.92% ± 1.38% for OmniPod, 8.75% ± 1.31% and 7.70% ± 1.33% for Animas (P = 0.63 for the difference between the groups), mean glucose values at initiation and end were 185.3 ± 4.4 and 194.9 ± 37.8 for Medtronic, 171.6 ± 41.7 and 183.5 ± 39.5 for OmniPod, 171.9 ± 46.5 and 206 ± 49.7 for Animas (P = 0.78 for the difference between the groups), mean SMBG at initiation and end was 8.8 ± 3.7 and 8.3 ± 4.2 for Medtronic, 6.2 ± 2.5 and 5.9 ± 3.4 for OmniPod, 8.3 ± 3.2 and 6.8 ± 2.3 for Animas (P = 0.87), and BMI-SDS at initiation and end was 0.2 ± 1 and 0.4 ± 1 for Medtronic, 0.3 ± 0.9 and 0.4 ± 0.9 for OmniPod, 0 ± 1.1 and 0.2 ± 0.5 for Animas (P = 0.12).
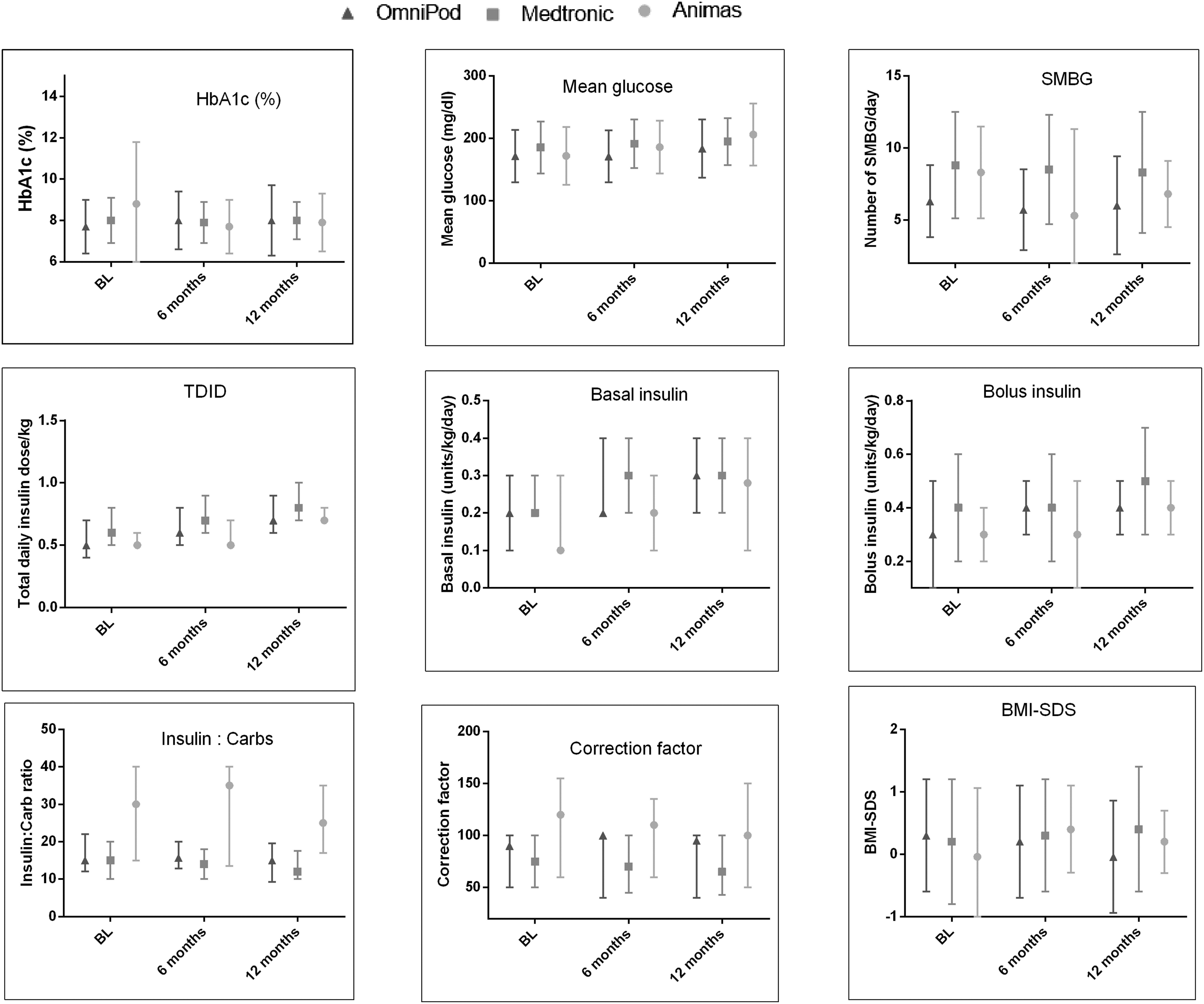
Comparison of glycemic control, BMI-SDS, and pump setting parameters between devices. The GEE model was applied to assess differences between pumps over time, from BL until 12 months after start of pump therapy. Data points represent mean (standard error). No statistically significant differences were found in any of the parameters examined over time between the groups: for HbA1c P = 0.63, for mean glucose P = 0.78, for mean number of SMBG per day P = 0.87, for median and IQR of TDID P = 0.36, for basal daily insulin dose P = 64, for daily bolus dose P = 0.13, for insulin to carbs. BL, baseline; BMI, body mass index; GEE, generalized estimating equations; HbA1c, glycated hemoglobin; IQR, interquartile range; SDS, standard deviation score; SMBG, self-monitoring of blood glucose; TDID, total daily insulin dose.
No differences were found in median and IQR of insulin TDD at initiation and end: 0.6 (0.5, 0.8) and 0.8 (0.7–1) for Medtronic, 0.5 (0.4, 0.7) and 0.7 (0.5, 0.9) for OmniPod, 0.5 (0.5, 0.9) and 0.7 (0.7, 0.8) for Animas (P = 0.36), with similar basal-bolus ratios and carbohydrate to insulin and correction ratios.
Discussion
This study demonstrates the noninferiority of commonly used insulin pump devices of three manufacturers, in various aspects of diabetes management among pediatric patients with T1D, including glycemic control, short-term diabetes-related complications, technical difficulties of daily use, and QOL. In the decision-making process of selecting an insulin pump device, patients and their families are faced with several sources of information: social media, agents of manufacturers, and health care providers. While the first two sources are based on personal experience and self-interests, the recommendations provided by the diabetes team should rely on objective evidence-based information. To the best of our knowledge, this is the first study to compare various aspects of a number of insulin pump devices used by children with T1D in a real-world setting. According to our findings, patients should choose their insulin pump device according to convenience and lifestyle preferences, as no evidence-based superiority was found of one pump device over another.
The rate of pump discontinuation was 12.3%, similar between pump devices, and similar to previous reports. 17 The statistically significant indicators for pump discontinuation in our study were their older age, longer duration of diabetes before pump initiation, more frequent SMBG, and no previous use of technological devices such as CGM. Our findings add to previous reports indicating discontinuation predictors in a relatively large population, which may add to the considerations taken before pump initiation in clinical practice.
Among >28,000 adolescents with T1D enrolled in the Exchange Clinic Registry, and National Paediatric Diabetes Audit, during 2011–2012, >40% were using insulin pumps. 3 Since patients generally choose a new pump every few years, according to insurance policies, this is an important decision. Therefore, health care providers of patients with T1D should endeavor to provide their patients with objective recommendations.
Concurring with our findings, a crossover pattern randomized study that comprised 29 pediatric patients 9 reported no significant difference in QOL between users of wireless pumps and of pumps with tubing. However, in their study, the mean HbA1c levels significantly decreased during the first 12 weeks, with the use of both OmniPod and conventional pumps. The decrease in HbA1c was more marked in the OmniPod group. No additional improvement was observed in mean HbA1c value in either group during the following 12 weeks, which marked the end of the study. The current study did not demonstrate statistically significant changes in HbA1c during follow-up for any of the devices investigated. This can probably be attributed to the real-life observational design of this study, compared with interventional study protocols. Enrolling patients in a research study could in itself improve diabetes control in the short term.
We report similar satisfaction with diabetes treatment between patients, and between parents of patients, using different pump devices. Walsh et al. 12 evaluated general pump satisfaction, frequency of technical problems, daily usage parameters, and glycemic control, by means of a questionnaire-based survey in a large mostly adult population. They reported that only 47% of pump users were very satisfied with their pump, but 95% would recommend pump therapy to their friends. Although their report included multiple pump devices, it did not compare between the devices. The current study provides an important overview of the pump device setting and its impact. The finding that nearly 50% of pump users were also using a CGMS at the end of the follow-up period is not surprising, although this proportion is higher than previously reported by our group. 18 Yet, most sensor users were with the OmniPod and Animas, and not with Medtronic, despite the fact that the main feature of the latter is the “crosstalk” of CGMS and the pump (the sensor-augmented pump). This finding surprised us, since we expected that CGM users would prefer the sensor-augmented pump. We can only speculate with caution that it was related to the timing of study: during the year of the study, DEXCOM G4 was available in the market in Israel and the diabetes-related social networks had multiple advertisements regarding its accuracy and convenience.
The aim of the current study was also to provide an additional overview of possible differences in the pump device settings of basal and bolus ratios. Interestingly, despite the implemented differences in the specific device algorithms of length and timing of insulin delivery each hour, the carbohydrate ratios, correction factors, and basal to bolus ratios did not differ significantly.
Parental education is an acceptable parameter of socioeconomic state, and was used as an indicator for pump simplicity. The Medtronic and Animas devices are translated to Hebrew, while OmniPod is only in English. It was interesting to see that there was no difference in parental education while choosing the pump device, even though the language was different. Furthermore, it adds information that education level was not a parameter for pump initiation or discontinuation, nor pump satisfaction and CGM use.
The strength of the study is its methodology of nonfunded, real-life, multicenter data collection for comparison between devices, not reported in the literature so far, the relatively long follow-up duration, and the referral to glycemic parameters, as well as short-term complications and technical difficulties of use, including usage of disposable equipment and QOL. Despite several years of pump experience, knowledge is lacking regarding pump selection, real-life practice of the various devices, and possible differences in glycemic control and patient experience. The findings show the similarity between the devices, regarding all parameters, which may reassure both patients and their caregivers in the decision-making process between pump devices.
This study has several limitations. For one, the size of the groups was not equal, with a considerably higher proportion using the Medtronic pump. A possible explanation is that the cohort included Arab-speaking patients who prefer a pump with an Arabic language interface, a unique feature of the Medtronic pump. In contrast, the language interfaces of the OmniPod and Animas pumps are English and Hebrew, respectively. Second, it did not include a DTSQ at study initiation for all participants for comparison of QOL prior and after a year of use. However, the fact that QOL assessment at end of study was similar between pump devices answers the initial objective of the study of difference in satisfaction and QOL between devices after a year of constant use in a real-life setting. In conclusion, this prospective multicenter study offers an important overview of pump device performance in real life in a pediatric population. The findings show that all pump devices are well received in the pediatric population with T1D, and that there are no differences between the devices, regarding glycemic control parameters, short-term complications, usage of disposable equipment, and QOL after 1 year of use.
Footnotes
Acknowledgments
We thank Dr. Tomer Ziv for statistical analysis and Cindy Cohen for the scientific editing.
Author Disclosure Statement
All authors state that no competing financial interests exist in connection with the submitted article.