
Abstract
Objective:
To determine whether the glucose management indicator (GMI), an estimate of hemoglobin A1c (HbA1c) derived from continuous glucose monitoring (CGM) mean glycemia, differs by CGM system and patient race.
Methods:
One hundred three patients with prediabetes or stable diabetes and a minimum of 10 days of CGM data collected with the FreeStyle Libre CGM system immediately before measurement of HbA1c were included in this clinic-based observational study that used data from electronic health records in an academic endocrinology clinic. HbA1c and Libre CGM-measured mean glucose were plotted to derive a race-agnostic and race-specific regression equations to calculate a Libre-specific GMI (GMILi). The mean GMI derived from the published formula (GMIP) was compared with GMILi.
Results:
Mean ± SD (standard deviation) age of patients was 61.9 ± 13.3 years; 50% were of nonwhite race and 77% had type 2 diabetes; mean HbA1c was 62 mmol/mol (7.8%). The mean (range) number of days with available CGM data was 26 (10–90). The mean ± SD GMILi was higher than the GMIP in the entire cohort (7.9% ± 1.0% vs. 7.5% ± 1.0%, respectively; P = 0.01) and among Asian patients (7.9% ± 0.9% vs. 7.2% ± 1.0%, respectively; P = 0.03).
Conclusions:
In a cohort with prediabetes or stable diabetes, the regression equation to calculate GMI varied by CGM system and patient race. The development of device- and race-specific regression equations for GMI may be warranted.
Introduction
Hemoglobin A1c (HbA1c) is a well-established clinical measure of average glycemia over the prior 2–3 months and it is valuable for assessing patients’ overall glycemic trends over time, and as a surrogate marker for the development of long-term diabetes-specific complications. 1,2 However, HbA1c has limited utility in the patient's day-to-day diabetes management because it does not provide information on glycemic variability—including hypoglycemia—or daily patterns of glycemia. 3 Furthermore, HbA1c is not a reliable measure in patients with altered red blood cell life (e.g., anemia, hemoglobinopathies), and there are also racial differences in the correlation between HbA1c and mean glycemia. 4 –6 Due to the shortcomings of the HbA1c metric, real-time self-monitoring of blood glucose is used by patients to manage their day-to-day glycemia. However, self-monitoring of blood glucose has its own limitations with the major one being the need by the patient to perform a fingerstick to obtain a blood sample, which almost always results in an inadequate number of measurements that cannot fully capture daily glycemia.
Continuous glucose monitoring (CGM) is emerging as a new standard of care in patients with diabetes because it provides not only the patient's current glucose level but also real-time glycemic trends, including direction and rate of change, which can inform therapeutic decisions. Furthermore, analysis and synthesis of CGM data offer the patient and clinician valuable information on glycemic variability throughout the day, including degrees and patterns of hypoglycemia and hyperglycemia, which may lead to better long-term therapeutic and lifestyle modifications. 7,8 Since mean glucose levels correlate with HbA1c, a regression equation has been published to convert CGM-measured mean glycemia into an estimate of laboratory-measured HbA1c, which has been termed glucose management indicator (GMI). 9 The GMI indicates the HbA1c value that would be expected based on mean glucose concentrations measured in a large number of persons with diabetes. The GMI has been endorsed as a clinically useful metric that provides important clues and insights in the management of diabetes. 9 –11
The published regression equation for GMI has been derived using CGM data collected with a specific type of sensor (Dexcom G4 and G5), and it is not known whether this equation is applicable to other CGM sensors. In addition, the published regression equation is based primarily on data from non-Hispanic whites and it is not known whether the equation differs by race, especially in blacks and Asians. We conducted an observational study to test the hypothesis that the regression equation to calculate a GMI value varies by type of CGM system and patient race.
Methods
Study design
We conducted a retrospective clinic-based study using data available in the electronic health records from patients receiving care in a single-site academic endocrinology practice (Tufts Medical Center, Boston, MA) from January 1, 2018 to May 15, 2019. The study was approved by the Tufts Institutional Review Board.
Study population
We included data from patients with (a) any type of established diabetes based on ICD codes (managed with lifestyle only or being on a stable pharmacologic treatment regimen in the prior 3 months) or prediabetes based on ICD codes or medical history and (b) a minimum of 10 days of CGM data obtained with the professional or personal version of the FreeStyle Libre Flash CGM system (Abbott Diabetes Care, Inc., Alameda, CA) immediately prior to measurement of HbA1c. We excluded patients who at the time of the HbA1c measurement had (a) known anemia (hematocrit <32% for women, <36% for men), (b) received a red blood transfusion within the past 3 months, (c) any condition potentially interfering with measurement of HbA1c or rendering HbA1c results unreliable as an indicator of chronic glycemia (i.e., hemolysis, hemoglobinopathy, iron deficiency, estimated glomerular filtration rate below 15 mL/min/1.73 m2, or use of erythropoietin), and (d) a recent (within the last 3 months) large change in glycemic control (e.g., development of diabetes ketoacidosis) or change in antidiabetic medication (start/stop medication, change in dosage).
Data collection
As part of routine clinical care in our practice, the provider offers to patients who are not using a personal CGM the opportunity to have a Libre CGM professional sensor placed 2 weeks before their scheduled visit if the provider thinks that having detailed blinded CGM-measured glucose data would help guide treatment decisions. The device's factory-calibrated sensor measures glucose in the interstitial fluid every 15 min. Data collected with the Libre CGM professional system are “blinded,” that is, the patient has no interaction with the sensor and no access to real-time glucose data. At the visit (end of the wear period), the sensor was scanned and CGM data were uploaded to the FreeStyle LibreView software to generate a standard Ambulatory Glucose Profile report, which includes CGM-measured mean glucose concentration during the period of the CGM wear. At the same time of the CGM data download, HbA1c was measured at point-of-care using the DCA Vantage (CV 3.57%; Siemens Healthcare Diagnostics, Inc., Tarrytown, NY). An identical approach was followed for patients who wore the personal Libre CGM personal system. The personal system provides real-time glucose data when the patient uses a reader (or smart phone) to scan the sensor. All patients received individualized pharmacotherapy and lifestyle recommendations at the discretion of their treating clinicians, including how to incorporate real-time CGM data in day-to-day diabetes management. We collected the following variables from the electronic health record: age, sex, race/ethnicity, body mass index, diabetes type, diabetes years of diagnosis, and HbA1c.
Statistical analysis
We computed a regression equation for the association between HbA1c and Libre CGM-measured mean glucose concentration for the entire cohort regardless of race. Each patient contributed a single datapoint in the regression equation. If a patient had more than one CGM wear period/HbA1c combination during the period of the study, the combination that reflected the most stable period (as evaluated by the treating clinician) was included in the analysis. We used this regression equation to calculate a race-agnostic, Libre-specific GMI (GMILi) for each patient. We used the published regression equation to calculate a race-agnostic, CGM-agnostic GMI [GMIP (%) = 3.31 + 0.02392 × mean glucose (mg/dL)] for each patient. 9 For the entire study population, we compared the mean GMILi to the mean GMIP using a t-test (two samples-unequal variances).
We also computed race-specific regression equations for the association between HbA1c and Libre CGM-measured mean glucose concentration for non-Hispanic white, black, and Asian (Chinese or Vietnamese) patients. There were too few Hispanic patients to derive a Hispanic-specific regression equation. We used these equations to calculate a race-specific, Libre-specific GMI for each patient according to his/her race (GMILi-WHITE, GMILi-BLACK, and GMILi-ASIAN). For the three subpopulations defined by race (i.e., non-Hispanic white, black and Asian), we compared the mean race-specific and Libre-specific GMI to the mean GMIP using a t-test (two samples-unequal variances).
To explore the possibility that glycemic gaps from personal CGM due to patient infrequent scanning did not influence results, we run sensitivity analyses after excluding patients with an average number of daily scans less than 3.
The sample size was estimated to be at least 95 patients to have a 90% power to detect a minimum of a 0.4% difference between the race-agnostic GMILi and GMIP in the entire study population. Our final dataset was larger which allowed us to also test differences by race.
Results
Study participants and CGM data
The analysis cohort consisted of 103 adults with mean ± SD (standard deviation) age of 61.9 ± 13.3 years (Table 1). Approximately half (49.5%) were of nonwhite race and 77% had type 2 diabetes. The mean HbA1c level was 62 mmol/mol (7.8%); 25% of patients had a HbA1c value less than 53 mmol/mol (7%), 34% had a value between 53 and 64 mmol/mol (7%–8%), and 41% had values of 64 mmol/mol (8%) or greater. Fifty-nine percent of patients contributed CGM data via the professional version and 41% via the personal version of the Libre CGM system. The mean (range) number of days with available CGM data was 26 (10–90). The Libre CGM-measured mean ± SD glucose concentration for the entire cohort was 174 ± 52 mg/dL.
Patient Characteristics
Unless otherwise specified, values are shown as means ± SD. Percentages may not add up to 100 because of rounding.
Race/Ethnicity was self-reported. The cohort also included Hispanic (n = 7) and Other/Unknown race (n = 2). Asian race includes Chinese (n = 20) and Vietnamese (n = 2).
To convert glucose from mg/dL to mmol/L, multiply by 0.055.
HbA1c, hemoglobin A1c; SD, standard deviation.
Regression equations for GMI
The linear regression between Libre CGM-measured mean glycemia and HbA1c measured at the end of the CGM wear period for the entire study population is shown in Figure 1a. This plot was used to derive a race-agnostic regression equation for a GMI specific to the Libre CGM system, as follows:
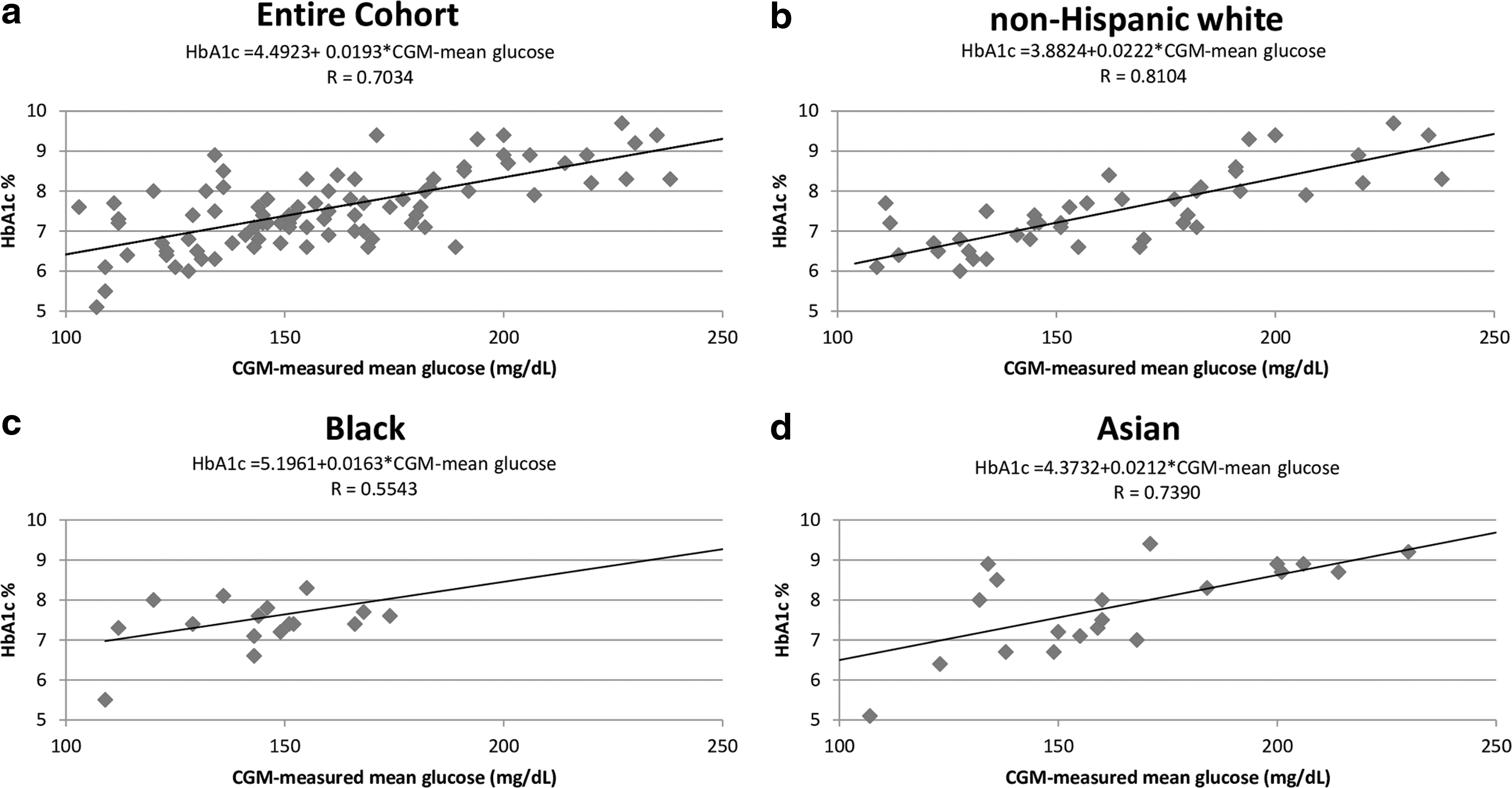
HbA1c versus FreeStyle Libre CGM-measured mean glucose concentration in the
GMILi (%) = 4.4923 + 0.0193 × Libre CGM-measured mean glucose (mg/dL)
The linear regression between Libre CGM-measured mean glycemia and HbA1c by race is shown in Figure 1b–d. These plots were used to derive race-specific regression equations for a GMI specific to the Libre CGM sensor system and also specific to our white, black and Asian population.
GMILi-WHITE (%) = 3.8824 + 0.0222 × Libre CGM-measured mean glucose (mg/dL) in whites
GMILi-BLACK (%) = 5.1961 + 0.0163 × Libre CGM-measured mean glucose (mg/dL) in blacks
GMILi-ASIAN (%) = 4.3732 + 0.0212 × Libre CGM-measured mean glucose (mg/dL) in Asians
Comparison of GMILi and GMIP
For the entire study population, the mean GMILi was higher than the mean GMIP (7.9% vs. 7.5%, respectively; P = 0.01) (Table 2). Among Asian patients, the mean GMILi-ASIAN was higher than the mean GMIP (7.9% vs. 7.2%, respectively; P = 0.03) (Table 2). The same pattern was observed among white (GMILi-WHITE 7.9% vs. GMIP 7.6%; P = 0.27) and black (GMILi-BLACK 8.0% vs. GMIP 7.4%; P = 0.14) patients, but the differences were not statistically significant. In sensitivity analyses, after excluding 14 patients who used the personal CGM system and had a mean number of daily scans less than 3, results did not change appreciably.
Mean Population Glucose Management Indicator Calculated Based on Libre-Specific Regression Equations Versus the Published Regression Equation
Values are means ± SD.
GMILi is a glucose management indicator specific to Libre CGM system based on the following regression equations (see also Results section): race-agnostic GMILi (%) = 4.4923 + 0.0193 × Libre CGM-measured mean glucose (mg/dL) or race-specific GMILi-WHITE (%) = 3.8824 + 0.0222 × Libre CGM-measured mean glucose (mg/dL), GMILi-BLACK (%) = 5.1961 + 0.0163 × Libre CGM-measured mean glucose (mg/dL), GMILi-ASIAN (%) = 4.3732 + 0.0212 × Libre CGM-measured mean glucose (mg/dL).
GMIp is a race-agnostic glucose management indicator based on a published regression equation as follows: GMIP (%) = 3.31 + 0.02392 × CGM-measured mean glucose (mg/dL). 9
CGM, continuous glucose monitoring.
Table 3 shows examples of GMI values calculated for various CGM-measured mean glucose concentrations when using the race-agnostic Libre-specific regression equation (GMILi) or the published regression equation (GMIP). At low mean glucose concentrations, there are large differences between the two GMI results. For example, a patient who has a CGM-measured mean glucose concentration of 125 mg/dL would have a GMI of 6.9% when using the Libre-specific regression equation and a GMI of 6.3% when using the published regression equation. At high mean glucose concentrations, these differences between the two GMI results were less pronounced.
Glucose Management Indicator Calculated for Various Continuous Glucose Monitoring-Measured Mean Glucose Concentrations, by Continuous Glucose Monitoring Device
GMILi is a race-agnostic glucose management indicator specific to Libre CGM system based on the following regression equations (see also Results section): GMILi (%) = 4.4923 + 0.0193 × Libre CGM-measured mean glucose (mg/dL).
GMIp is a race-agnostic glucose management indicator based on a published regression equation as follows: GMIP (%) = 3.31 + 0.02392 × CGM-measured mean glucose (mg/dL). 9
To convert glucose from mg/dL to mmol/L, multiply by 0.055.
Discussion
Our results showed that in a cohort with prediabetes or stable diabetes, the GMI value calculated from a Libre CGM-specific regression equation is higher than the GMI calculated from a published regression equation that was derived based on a different CGM system (Dexcom G4/G5). The GMI value may also be influenced by race.
Because of the wide range of mean glucose concentration associated with a given HbA1c level, utilizing HbA1c alone to manage diabetes is problematic, and self-monitoring of real-time glucose levels is needed for appropriate diabetes management. 3 The increased availability of CGM systems has led to the derivation of a formula to calculate an estimated HbA1c (eA1C) from CGM-measured mean glucose levels. 3 Comparing the eA1C with the observed (measured) HbA1c may provide additional important clues and clinical insights in the management of diabetes, especially when the eA1c differs from the HbA1c. 3,9 However, as the eA1C became more widely available and started appearing in standard ambulatory glucose profiles generated from CGM systems, the FDA began to receive reports of confusion from patients and health care professionals about the meaning of the eA1C metric. 12 To reduce the confusion in the interpretation of the eA1c, the GMI term was developed. 9 However, despite the name change, the GMI concept has limitations at least, in part, due to differences in CGM systems and the known racial differences in the correlation between HbA1c and mean glycemia, which our study examined. 4 –6
There are many potential reasons that can explain why GMILI differed from GMIP in our study. The published regression equation for GMIP was based on pooled data from three clinical trials using the Dexcom G4 Platinum CGM system with software 505 (315 adults with type 1 diabetes and 72 adults with type 2 diabetes) and one trial using the Dexcom G5 Mobile CGM system (141 adults with type 1 diabetes). 9,13 –16 In contrast, our regression equation for GMILI was derived using data collected with the Libre CGM system (professional or personal version). Although all CGM systems measure glucose in the interstitial fluid, there are several differences among them, including: overall accuracy (defined as the mean absolute relative difference between sensor readings and reference values), sensor wear time (6–14 days), requirement for calibration with self-obtained blood glucose (which improves accuracy), frequency of glucose readings (every 15 min for the Libre CGM vs. 5 min for all the other CGM devices), 17 and ability to automatically generate glucose data without the need for scanning by the patient. 18 Such device-specific differences are the most likely explanations for why the regression equations between GMILI and GMIP differ. Another difference to consider is that the pooled dataset used to derive the published regression equation for GMIP was primarily from adults with type 1 diabetes (86% of the cohort), while the cohort we used to derive the regression equation for GMILI was composed mainly of adults with type 2 diabetes (77%). However, there is scant evidence that type of diabetes may influence the association between HbA1c and mean glucose levels. 19
It is well recognized that black individuals have higher HbA1c levels than non-Hispanic white individuals for the same degree of mean glycemia and this observation was recently confirmed in a study that used CGM-measured glucose data collected with the Libre CGM professional system. 4 –6 Therefore, racial differences in the correlation between HbA1c and mean glycemia may have implications when deriving regression equations for the GMI. To the best of our knowledge, no study has previously evaluated a race-linked effect in how the GMI metric is derived. In our study, when we applied the race-agnostic equation for GMIP and compared to the race-agnostic Libre CGM system equation (GMILi) in our Asian study population, the difference between the two mean GMI values was 0.4%; when we applied the Asian-specific equation for the Libre CGM system (GMILi-ASIAN), the difference in GMI widened to 0.7% (Table 2). More studies are needed in larger and diverse populations to better understand how race might influence the derivation and application of the GMI.
Our findings are consistent with other studies reporting clinically meaningful differences (>0.5%) between laboratory-measured HbA1c and GMIP based on data from other glucose sensors (Dexcom, Guardian 3, and Navigator 2). 11 We found a higher discordance between the GMIP and measured HbA1c with the Libre system compared with other systems (Table 4), which may be explained by our multiracial cohort. Such discrepancies suggest that the detailed information on glycemic patterns provided by the CGM should be the primary tool for providers and patients in making informed lifestyle modifications and therapeutic decisions with the laboratory-measured HbA1c serving as surrogate marker for the development of long-term diabetes-specific complications. Providers willing to incorporate the GMI in diabetes management need to carefully explain to their patients the difference between this index and the laboratory-measured HbA1c 9 and to understand that each sensor has its unique relationship of mean glucose to GMI.
Difference Between Glucose Management Indicator Calculated from Continuous Glucose Monitoring-Derived Mean Glucose Using a Published Formula and Laboratory-Measured Hemoglobin A1c
Formula available from Bergenstal et al. 9
Data for Guardian 3, Navigator 2 and Dexcom sensors are from Leelarathna et al. 11 in a predominantly Caucasian population with type 1 diabetes.
Data for FreeStyle Libre sensors are from the present article (n = 103 patients), which includes a multiracial population of predominantly patients with type 2 diabetes.
Our study has several strengths. We included real-world data from typical patients with at least 10 days of CGM data (consistent with current guidelines) immediately prior to HbA1c measurement by the same point-of-care device thereby limiting interlaboratory variability in HbA1c assay methodology. Our patient population is heterogeneous in terms of age (range 21–90 years), race (50% white; 20% black; 21% Asians), and glycemic control (HbA1c range 29–126 mmol/mol [4.8%–13.7%]), which improves external validity.
Our study has limitations. First, the sample size is relatively small, which limited our ability to examine the impact of races other than Asian. Second, the published regression equation for GMIP incorporated data from a mean 48 (range 13–89) days with available CGM glucose values compared to our regression equation for GMILI which integrated data from a mean 26 (range 10–90) days with available CGM glucose values. 9 However, 10–14 days of CGM data correlate well with 3 months of CGM data, and sampling of additional days beyond the last 14 days of CGM wear before HbA1c measurement does not substantially improve the correlation between CGM-measured mean glucose levels and HbA1c. 20 Therefore, the shorter mean observational period in our study should not have significantly impacted our regression equation for GMILI, especially since the agreement between CGM-measured mean glucose and HbA1c seems to plateau by about 7–10 days of data over a period of stable diabetes management. 21 Third, the published GMI formula was based on measurement of HbA1c at a research laboratory, whereas HbA1c was measured with a point-of-care device in the current study. Finally, our analysis is limited to glucose data collected with one specific CGM system and our comparison of calculated mean GMI values is not based on concurrently generated data using different CGM systems in the same population.
Conclusions
In this retrospective observational study in a typical clinic patient population, the GMI calculated from a Libre CGM-specific regression equation differed from the GMI derived from a published formula based on data collected with a different CGM system in a cohort with prediabetes or stable diabetes. GMI may also vary by race. If our findings are replicated in other larger studies (especially trials), and GMI is accepted as a core CGM metric, development of a CGM system- and race-specific regression equations may need to be developed.
Footnotes
Acknowledgments
All authors contributed to the concept and design of the study and writing and critical revision of the article. E.A. is the guarantor of this work and, as such, takes responsibility for the integrity and accuracy of the study design.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported, in part, by generous donations to the Tupper Research Fund at Tufts Medical Center. This work was presented as an abstract at the 79th ADA Scientific Sessions (June 7–11, 2019) in San Francisco.