
Abstract
Background:
The Medtronic MiniMed™ 670G system adjusts basal insulin delivery in response to continuous glucose monitoring levels and is already in use in clinical practice. We tested the home-based feasibility of the new MiniMed advanced hybrid closed-loop (AHCL) system, which includes several algorithm enhancements and an optional autocorrection bolus mode.
Methods:
Twelve adolescents and young adults (eight females) with type 1 diabetes [median (interquartile range)] aged 16.6 (15.9, 18.2) years and diabetes duration of 7.1 (4.7, 8.8) years] participated in this single-arm study. The first stage was a 6-day open-loop run-in period, with the predictive low-glucose suspend feature on. This was followed by 6 days/5 nights in a supervised hotel setting, using the AHCL system, including closed-loop challenges (missed meal bolus, late meal bolus, and physical activity); and finally, 3 weeks with unrestricted home use. Glycemic parameters were compared between the open-loop and closed-loop periods.
Results:
Participants spent 93.3% (4.7) of the time in SmartGuard™ Auto Mode. Hemoglobin A1C levels decreased from median (interquartile range) 7.1% (6.7, 7.9) at baseline to 6.8% (6.6, 7.4) at study end, after 4 weeks (P = 0.0027). Time in range (TIR) (70–180 mg/dL) was 68.4% (10.6) and time below 70 mg/dL was 4% (3.5) during open-loop; and 74% (6.1) and 2.6% (1.9), respectively, during the closed-loop at home phase (P = 0.06, P = 0.27). TIR increased during the nighttime, from 64.6% (17.4) to 80.7% (7.8), P = 0.007, without change in time below 70 mg/dL (P = 0.15). No serious adverse events occurred.
Conclusions:
The new AHCL system demonstrated safety and effectiveness in controlling day and night glucose levels.
Introduction
Closed-loop systems are becoming an integral part of diabetes management. These systems have uniformly been shown to improve glycemic control and to reduce hyperglycemia and hypoglycemia, while modestly reducing hemoglobin A1C (HbA1c) levels and improving quality of life. 1 While overnight closed-loop control is satisfactory using current means, postprandial hyperglycemia during daytime remains a challenge. 2
The MiniMed™ 670G system was the first closed-loop system to be approved by the U.S Food and Drug Administration (FDA) for people with type 1 diabetes (T1D) and until recently, the only system with regulatory approval used in clinical practice. 3 A large retrospective analysis of real-world glucose data of the first 3141 people with T1D to use the system showed the advantage of an increased sensor time in range (TIR), by about 7%, together with reduced time in hypoglycemia. However, time spent in hyperglycemia remained between 21% and 33% across all age groups. 4 In another retrospective study of 127 adults aged 21–68 years who switched from sensor augmented pump therapy to the MiniMed 670G system, TIR increased by a mean of 12.4% and hypoglycemia below 70 mg/dL decreased by 1%, after 6 months of use. The time in hyperglycemia above 180 mg/dL was 26%. 5
The MiniMed 670G system uses a modified adaptive proportional-integral-derivate with insulin feedback (PID-IFB) algorithm to automatically modulate insulin basal rate delivery according to sensor-measured glucose levels, with personalized dynamic constraints on insulin delivery. 6,7 In this hybrid system, the users still need to manually deliver insulin boluses to cover carbohydrate consumption and to correct high blood glucose levels. While changing the basal rate yields gradual improvement in glucose levels, a bolus correction can achieve similar results more quickly, due to the pharmacodynamics and pharmacokinetics of the currently available insulins. Therefore, a closed-loop system capable of delivering automated insulin boluses can further improve glycemic control. The MD-Logic was the first system to incorporate automated correction boluses during closed-loop operation. In addition, its meal-detection algorithm enables the MD-Logic a different method for calculating meal boluses than for calculating correction boluses during the fasting state. 8 –10 Data from the first studies on automated insulin boluses incorporated in closed-loop operation were demonstrated to be safe during night and day. 10,11
As closed-loop systems have demonstrated safety, the next steps in development are to further reduce hyperglycemia by the use of automated boluses, lowering of the glucose target, and reducing alarms and the workload needed for system operation. The MiniMed Advanced Hybrid Closed-Loop (AHCL) has several enhancements over the MiniMed 670G system, aiming to provide solutions for these exact goals: an improved autobasal control, which significantly tightens glycemic control and reduces the number of system alarms, an addition of autobolus module (developed in collaboration with DreaMed Diabetes Ltd.) that delivers correction boluses automatically, a meal detection module (developed by DreaMed Diabetes Ltd.), which if triggered can potentially let the system deliver more aggressive autocorrection boluses, and finally, three available options for autobasal glucose targets (100, 120, or 150 mg/dL). The controller was tuned to a lower setpoint of 100 mg/dL, aiming to achieve tighter control without compromising safety.
We conducted a small feasibility study to evaluate the performance of the AHCL system by adolescents and young adults living with T1D, who are treated at the Schneider Children's Medical Center (Petah Tikva, Israel).
Research Design and Methods
Study design
This single-center, single-arm feasibility study evaluated the performance of an AHCL system at Schneider Children's Medical Center of Israel. Twelve participants with T1D underwent an at-home run-in phase with the system in an open-loop for 6 days, followed by a 6 days/5 nights hotel phase in AHCL Auto Mode, and finally a 3-week unsupervised at-home phase in AHCL Auto Mode.
The study was approved by the Rabin Medical Center Institutional Review Board (IRB) and was conducted in compliance with the protocol, the Declaration of Helsinki, and applicable regulatory and Good Clinical Practice requirements. All the participants and their parents provided a written informed consent before study initiation. The study is registered in
Participants and eligibility criteria
Eligible individuals were recruited from the Schneider Children's Medical Center of Israel. The main inclusion criteria for participation were age 14 to 40 years; T1D for at least 1 year; the use of an insulin pump for at least 6 months; previous experience with continuous glucose monitoring (CGM); HbA1c below 10% [86 mmol/mol]; willingness to perform ≥3 finger stick blood glucose measurements daily and required sensor calibrations; and living with at least one adult educated in the management of diabetes. The main exclusion criteria were concomitant disease, or other conditions and medications that could influence metabolic control, compromise safety, or prevent participants from completing the study; participation in another study; pregnancy; an episode of diabetes ketoacidosis or hypoglycemia resulting in seizure or loss of consciousness within 6 months before enrolment; an intention to travel abroad during the study duration; sensor tape adhesive allergy; and any disease or condition that may influence glycated hemoglobin testing.
Study investigational closed-loop device
The MiniMed AHCL system (Medtronic, Northridge, CA) consists of the MiniMed 670G insulin pump with the SmartGuard™ AHCL algorithm; a Medtronic Guardian™ 3 Sensor; a Guardian™ Link 3 glucose sensor transmitter; and a CONTOUR®NEXT LINK 2.4 blood glucose meter (Ascensia Diabetes Care, Parsippany, NJ).
The MiniMed AHCL system has several distinguishing features over the commercial MiniMed 670G system during Auto Mode: (1) The controller glucose setpoint (i.e., basal target) was redesigned and returned to enable a new optional lower glucose setpoint of 100 mg/dL, in addition to the existing option of 120 mg/dL and the temporary setpoint of 150 mg/dL up to 24 h. (2) Improved safety features enable increased time spent in Auto Mode. This improves user experience and reduces exits from Auto Mode, thus enabling operation of the system without interruption. 12 For example, a change in closed-loop safeguards increases the minimum insulin delivery timeout exit from 2.5 to 3–6 h (depends on insulin on board), and the maximal timeout exit from 4 to 7 h. These enable increased safe basal time to 4 h. The modifications in the insulin timeout have been previously described and tested. 12 In addition, alerts were modified; for example, a high glucose alert notifies but does not cause the user to exit the Auto Mode when glucose levels exceed 250 mg/dL for more than 3 h. The function that alerted and forced out from Auto Mode when glucose sensor levels exceeded 300 mg/dL for more than an hour was removed. (3) Automated correction boluses are based on sensor glucose levels 13 and delivered up to every 5 min to achieve a target of 120 mg/dL. Thus, correction boluses can be delivered when sensor glucose level is above 120 mg/dL before high-glucose levels occur. A temporary glucose target of 150 mg/dL can be manually set, during which no autocorrection boluses are given. This temporary glucose target can be used for physical activity. The active insulin time (AIT) during the study was fixed and set at 4 h for all the participants. The glucose setpoint was uniformly set to 100 mg/dL during the hotel and home phase closed-loop use.
The system enables the use of sensor glucose values for bolus calculations, whenever glucose values from a blood glucose meter are not available. The system also has a “safe meal bolus” feature that can reduce the insulin bolus per meal to mitigate the risk of hypoglycemia.
Interventions
All the participants completed a 6-day run-in period, during which they used the MiniMed AHCL pump with the closed-loop SmartGuard™ Auto Mode feature off and the predictive low-glucose suspend feature on. This was followed by a 6 days/5 nights supervised hotel phase, during which the system with the closed-loop feature was on, and finally a 3-week unsupervised at-home phase with the closed-loop feature on.
Insulin pump optimization and a dietitian's evaluation of the required carbohydrate ratio were performed at the screening visit and before the hotel phase of the study. Participants continued to use their own insulin: eight participants used Novorapid (insulin aspart) and four Humalog (insulin lispro).
The participants received training regarding data download at home and the use of the insulin pump and sensor. They were asked to download devices data every other day during the run-in period.
Hotel study phase period
After the 6-day at-home run-in period, all the participants attended a 6 days/five nights' stay in a supervised hotel setting. On the first day, the data from the run-in period were downloaded from the various devices. The data were reviewed by the study physicians, and carbohydrate ratios were modified as needed. Then, the participants underwent a 1-h training session on closed-loop use and the system was activated. During the hotel stay, participants were not limited in their activities or in their meal or snack preferences or content (except for the meal challenges). Participants were instructed to use the bolus calculator for every meal and deliver premeal boluses.
The hotel phase of the study also included three closed-loop challenges (a missed meal bolus, a late meal bolus, and physical activity), starting from day 3 of the hotel stay. On day 3, a missed dinner bolus challenge was conducted. The participants were instructed to consume 40 g of carbohydrates (approved by a dietitian) without giving a premeal bolus and were not allowed to eat for 5 h thereafter unless hypoglycemia ensued. On day 4, a late meal bolus challenge was conducted. The participants were instructed to consume 40 g of carbohydrates, and deliver a meal bolus, calculated by the bolus wizard using current sensor glucose data, only 20 min after the meal had commenced. Participants were not allowed to eat for 5 h thereafter unless hypoglycemia ensued. Notably, other than the carbohydrate amount, the content of the two meal challenges was similar, but not identical and was determined for each participant individually.
On day 5, a mild to moderate physical activity challenge of an hour's duration of jogging in the park (with breaks as needed) was conducted. The glucose target was set to 150 mg/dL 2 h before the physical activity and turned off at the end of the activity. Dinner was served 3 h after completion of the afternoon activity.
Home study phase period
At the end of the hotel stay, participants returned to their homes to use the closed-loop system for an additional 3 weeks' period with no restrictions. They were asked to give premeal boluses as per usual care, ∼15 min before each carbohydrate containing meal, and to upload data every evening. The data were reviewed by the study team and only the insulin-to-carbohydrate ratio was modified as necessary.
Statistical analyses
As this was a feasibility study focused mainly on safety outcomes, the sample size was not calculated. Similar to other feasibility studies, we recruited 12 participants. 12,14
Glycemic control, as measured by various CGM metrics, was averaged per participant and compared between the open-loop run-in period, the hotel closed-loop period, and the home closed-loop period. The primary efficacy endpoint was TIR (70 to 180 mg/dL), as measured by the CGM. Exploratory outcomes included the percentage of time spent in hypoglycemia (below 70 and below 54 mg/dL), the percentage of time spent in hyperglycemia (above 180 and 250 mg/dL), mean glucose and standard deviation (SD), total daily dose of insulin, percentage of basal insulin of the total daily dose, and the percentage of time using the sensor and closed-loop. Subanalyses were performed separately for daytime (6 AM–midnight) and nighttime (midnight–6 AM) outcomes. The nighttime analysis also included the percentage of time spent in a stricter target range of 70 to 140 mg/dL.
Glucose levels from CGM during the 5 h following the two meal challenges (missed and late bolus) were analyzed. Outcome measures for the meal challenges included the following: peak postprandial glucose level, 2 h postprandial glucose levels, mean glucose area under the curve (AUC) >180 mg/dL, mean and SD glucose levels, time in different ranges (70–180 mg/dL, >180 mg/dL and <54 mg/dL), and insulin delivery for the 5 h postprandial period. CGM metrics were compared for missed (n = 12) and late (n = 12) meal challenges conducted during the hotel stay, home-phase, 40-g dinners (n = 27), and all home-phase meals containing 40 g of carbohydrates (n = 116).
Outcome measures for the physical activity challenge were CGM metrics for the 2 h following the physical activity.
Capillary HbA1c was measured and compared between the start and end of the study using a point-of care DCCT standardized capillary glycated hemoglobin measurement (DCA 2000 or DCA 2000+ or DCA Vantage utilizing the same reagents).
Outcomes were summarized as mean ± SD, unless otherwise indicated. Statistical analyses were performed by paired t-test. A P-value of <0.05 was considered statistically significant.
Results
The study was conducted between October 10 and November 11, 2018. Twelve participants, nine adolescents, and three young adults, with age range of 15 to 25 years, and HbA1c range of 6.6% to 8.4% at screening, started and completed the study. Participant characteristics are presented in Table 1. At enrolment, seven participants used CGM and five participants used flash glucose monitoring. All participants used Medtronic pumps before entering the study, two of whom used the predictive low-glucose suspend feature, two used it intermittently (only when using the sensor), and one participant used the suspend-on-low feature (Supplementary Table S1).
Baseline Patient Characteristics, n = 12
Median (IQR).
Excluding two adults.
HbA1c, hemoglobin A1C; IFCC, The International Federation of Clinical Chemistry Standardization units; IQR, interquartile range; SDS, standard deviation score.
Glycemic control
Glycemic parameters for each study phase are presented in Table 2. Between the run-in period and home-use phases, TIR (70–180 mg/dL) increased on average by 5.6%, while time in hypoglycemia (<70 mg/dL) decreased by 1.4%; these differences did not reach statistical significance. Capillary HbA1c levels decreased significantly from 7.1% (6.7, 7.9) at baseline to 6.8% (6.6, 7.4) at study end, after 4 weeks (P = 0.0027). During the night (00:00–06:00 h), TIR (70–180 mg/dL) increased significantly by 16.1% (P = 0.007), with no change in time in hypoglycemia (P = 0.15).
Glycemic Parameters and Insulin Delivery During the Run-in, Hotel, and Home Phases
Values are presented as mean (SD).
P-value calculated between run-in and home period.
SD, standard deviation; TIR, time in range.
Insulin treatment
Total daily dose of insulin was 57.8 U (11.4) in the run-in period and 53.9 U (11.9) during the home phase (P = 0.11), (Table 2). The percentage of insulin given as basal was higher during the run-in period than in the home phase, 54.3% (8.9) and 41.7% (4.4), respectively (P = 0.01).
Meal challenges
All the participants completed the missed bolus and late bolus challenges. The corresponding postprandial glycemic parameters are presented in Table 3 and Figure 1. TIR for the 5-h postprandial period was 55.2% ± 26.6% when no premeal bolus was given, and 48.1% ± 28.1% when the premeal bolus was delayed by 20 min (P = 0.57). Time in significant hypoglycemia (below 54 mg/dL) was 0.55% ± 1.8% and 1.3% ± 4.1% for the respective challenges (P = 0.63).
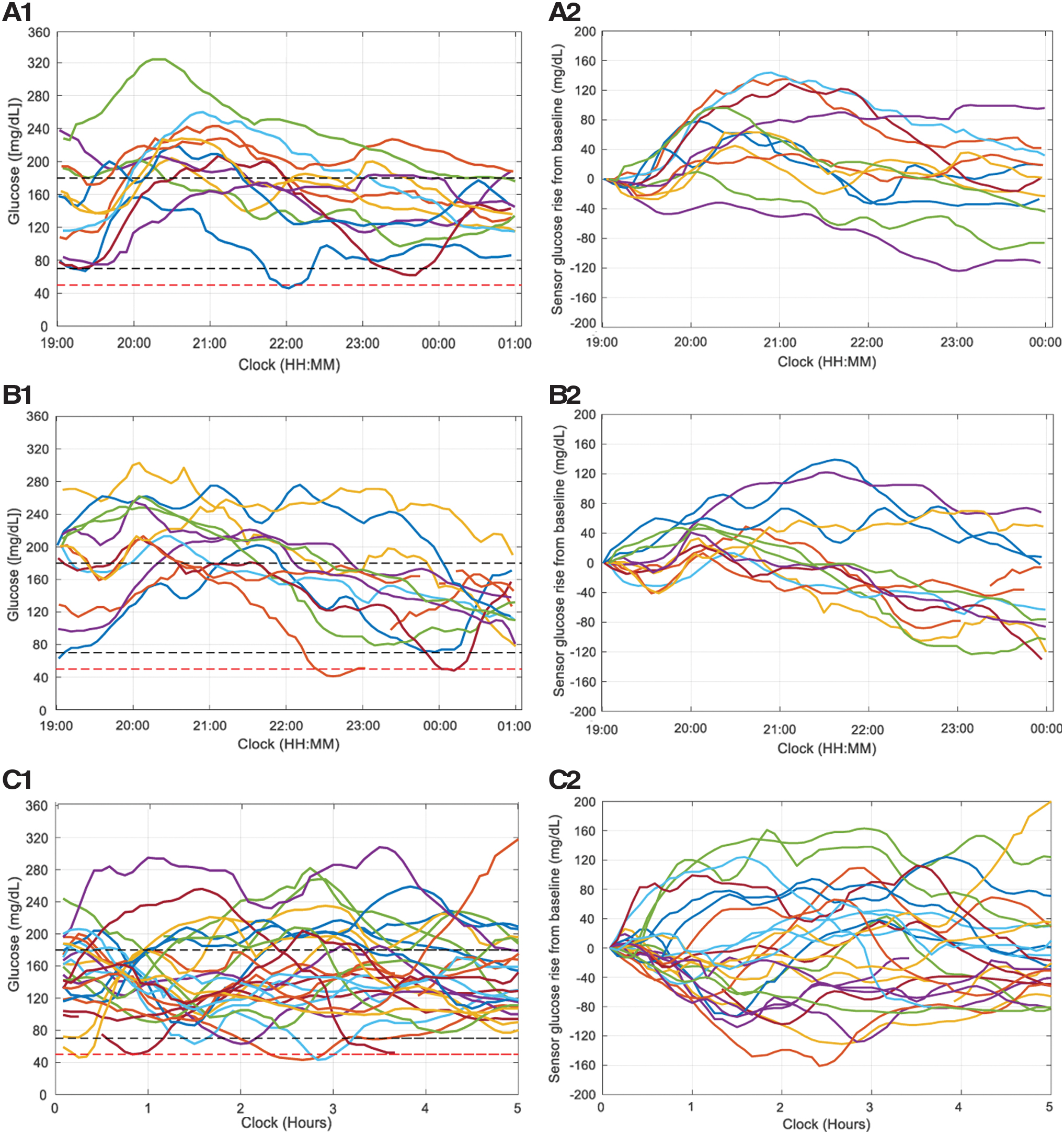
Postprandial glycemic response following missed and late meal bolus challenge and outpatient home dinner meals. Data gathered from 12 evening dinner meals during hotel study phase and 27 outpatient dinner meals, each including 40 g of carbohydrates.
Glycemic Parameters During Meal Challenges and Matched Home Size Meals
Values are shown as average ± SD.
Sensor glucose values were normalized by subtracting the sensor glucose value at the time of meal announcement.
Glucose level at the time of meal announcement, that is, 20 min after the start of the meal.
AUC, area under the curve; CGM, continuous glucose monitoring.
Data comparing the missed bolus meals (n = 12) during the hotel phase with matched meals containing 40 g carbohydrates, with premeal bolus, at dinner-time during the home phase (n = 27) is presented in Table 3 and Figure 1. For the missed bolus meal challenge, significant differences were not observed between the hotel setting and the home phase, in the peak glucose response (224.4 ± 40 and 215.3 ± 44.1 mg/dl, respectively, P = 0.55) or in the mean AUC above 180 mg/dL (P = 0.41). The average sensor glucose level 2 h after dinner meals at home was significantly lower than after meals with no bolus delivered at the hotel. Nevertheless, when normalizing the starting glucose at time of the meal, no significant difference was found between missed hotel and home meals. A similar comparison between CGM outcomes of the missed bolus meal challenge and all at-home, 40 g carbohydrate meal, is presented in Supplementary Table S2.
Physical activity challenge
Eleven participants completed the physical activity challenge. No carbohydrate supplementary was given. No hypoglycemia events occurred during the physical activity. Hypoglycemia below 54 mg/dL was not recorded during the 2 h period after exercise. The time spent below 70 mg/dL was 1.5% (4.8). The mean sensor glucose level during this period was 151.4 (31.8) mg/dL and the TIR was 65.5% (26.3).
Home phase, meal insulin-dose adaptation
During the closed-loop period, the insulin-to-carbohydrate ratio was strengthened in 8 of the 12 participants. The mean change was from 1:8 to 1:7.2, which is a reduction of mean 0.79 g of carbohydrate for 1 U of insulin (range −0.5 to 2 g). The initial, open-loop percentage of basal insulin of the total daily dose was 43.7% ± 10% for the four participants who did not need carbohydrate ratio adjustments, and 50.1% ± 5.2% for those who needed a change during the closed-loop.
System usage
Average CGM usage was 98.4% ± 2.7% during the run-in phase, 97.8% ± 3.2% during the hotel phase and 91.5% ± 5.5% during the home phase of the study. An average of 3.8 ± 0.6 fingersticks was taken per day throughout the study and the sensor median ARD was 10.5%. The AHCL system was in Auto Mode 98.7% ± 1.7% of the time during the hotel phase and 93.3% ± 4.7% during the home phase (Table 2). The total number of exits from Auto Mode averaged at 0.4 ± 0.4 times per week during the home phase. The causes for Auto Mode exits were sensor calibration failure and Auto Mode fail-safe timeout. The overall temporary target of 150 mg/dL was used for an average of 3.2 ± 4.9 h during the entire home phase period.
Adverse events
No serious adverse events were reported during the study. Two participants reported abdominal pain during the hotel phase, and one participant had common cold symptoms during the home phase.
Discussion
The use of the new AHCL system with enhanced features and automated insulin correction boluses was found to be feasible, safe, and effective, in controlling day and night glucose levels for adolescents and young adults with T1D.
The glycated hemoglobin level significantly improved, even though the observational period was short. The reduction in HbA1c was correlated with the observed 5.6% increase in TIR. Although the latter was nearly statistically significant, the magnitude of improvement was recently defined as clinically significant. 15 Time spent in hypoglycemia decreased during the AHCL versus the run-in open-loop period, although this change also did not reach statistical significance. During the overnight period, TIR significantly increased, by 16.1%, and the time in hyperglycemia significantly decreased, without a change in time in hypoglycemia. Notably, the improvement in TIR was achieved even though most adolescents and young adults who participated had targeted glycemia before the study. Furthermore, the improved glucose control was not accompanied by an increase in hypoglycemia, and a trend toward reduced hypoglycemia was even observed. In a small feasibility study of adults using an earlier version of the AHCL, TIR increased by 10%, from open-loop to closed-loop use, but the time spent in hypoglycemia below 70 mg/dL also increased. 13
We report high use of the system in Auto Mode (around 99% of the time). This supports previous evidence that the new system enables fewer exits from Auto Mode, in a safe manner. 12,13 Although not evaluated in this study, an increase in the time spent in closed-loop control has been shown to be directly related to increased TIR and better glucose outcomes. 16 Real-world data were recently obtained from a retrospective study of 92 participants aged 2–25 years who started using the MiniMed 670G closed-loop system. While TIR increased by a mean of 6.2%, one-third of the participants discontinued the closed-loop within the first 6 months of use. 17 The main reason reported was the inconvenience related to exits from the closed-loop mode and multiple system alarms. In another observational study, one-third of the 79 participants aged 9–61 years discontinued use of the closed-loop after a year. The main reason was sensor related issues such as alarms and sensor calibration. 18 We assume that the current AHCL will improve engagement, as it reduces the need to give manual correction boluses, the number of exits from closed-loop mode, and the frequency of system alarms, while there is still a need to measure blood glucose for sensor calibration.
The total daily amount of insulin delivered during the run-in period was comparable to the amount delivered during the closed-loop period. However, during the closed-loop use, a higher proportion of insulin was delivered as bolus than as basal, with about 60% of the total daily dose given as boluses. Previous closed-loop studies and open-loop studies with pump therapy have shown that a higher ratio of bolus to basal insulin is associated with better glycemic control 11,19 and lower glycated hemoglobin. 20,21 In comparison, a recent study of adolescents and young adults showed no changes in the total amount of insulin delivered, and in the bolus to basal ratio in the switch from open-loop to MiniMed 670G Auto Mode treatment. 22
The difference in insulin delivery between the two closed-loop systems lies in the capability of the AHCL system to deliver automated boluses. This feature yielded acceptable postprandial glucose control for missed bolus meals. Although the current study did not directly compare between missed meals and meals with prebolus, the comparison between matched carbohydrate meals from the home phase suggests that the AHCL can handle missed boluses similarly to premeal boluses, for meals that contain 40 g of carbohydrates. The capability of effectively compensating for missed meal boluses is important, especially among adolescents and young adults, for whom engagement with treatment can be low with frequent omission of insulin boluses for meals. 23,24 An interesting finding was that delivering the bolus after the meal (late meal bolus challenge) was associated with greater glucose variability and a tendency for late hypoglycemia, compared to missing a bolus for the meal.
During the closed-loop period, the insulin-to-carbohydrate ratio was strengthened for two-thirds of the participants. This is despite its being reviewed and optimized by a dietitian and a physician before the beginning of this period. The change in insulin-to-carbohydrate ratio enabled more aggressive treatment for meals. A similar observation was reported among users of the MiniMed 670G system, with a 0.5 reduction in the carbohydrate-to-insulin ratio for all three meals. 22 The ability to modify the basal rate at real-time enables delivering more insulin as a premeal bolus.
The AIT was fixed at 4 h during this feasibility study, although this parameter can be set in the range of 2–8 h, with increments of 15 min. This was an extended AIT determined for safety when testing the system for the first time, as even for the MiniMed 670G, the optimal setting for active insulin has been suggested to be 2–3 h. 22 The effect of the AIT on the AHCL system performance is much more significant than the commercial 670G. Shortening of the AIT will enable more timely correction boluses delivered by the AHCL system. Perhaps a shorter AIT would result in better overall glycemic control and more time spent in range, by increasing the frequency and size of the autocorrection boluses. This way of delivering automated correction boluses is a key differentiator between the AHCL system and the recently approved Control-IQ algorithm, which also incorporates automated boluses. The AHCL autocorrections can be delivered every 5 min rather than every 60 min. 25 –27
The system performed well during physical activity with no hypoglycemic events during and 2 h after exercise. This may be attributed, in part, to the use of a temporary target glucose of 150 mg/dL, which was set 2 h before exercise. We are aware that in practice, this manual action might be much to expect, particularly in adolescents.
As a feasibility study, the number of participants was small, the duration was short, and a control arm was not established. In addition, most of the participants recruited had targeted or near targeted glycemia before entering the study. The aim was to examine the safety in using the AHCL among adolescents and young adults. Therefore, study outcome measures should be interpreted accordingly.
In conclusion, the use among adolescents and young adults of the new AHCL system, with automated boluses, was found to be safe and effective, resulted in high TIR within the recommended range without increase in hypoglycemia, and provided reasonable glycemic stability after missed boluses. Larger and randomized control studies are of merit and in process. Direct comparisons between the commercially available Medtronic MiniMed 670G system and the new AHCL system with automated boluses and lower basal target setpoint should be examined and are ongoing.
Footnotes
Acknowledgment
We express our gratitude and appreciation to the participants and their families. We thank the Medtronic team for providing training and technical support during the study. The authors thank the study team members from Schneider Children Medical Center of Israel, the Institute for Endocrinology and Diabetes: Galit Shiovitch Mantzuri R.N M.N, Orit Choresh B.A. R.N, Irit Drutz B.A. R.N, Yehiel Nava B.S.N, R. N, Gila Fayman R.D, Tamar Propper-Lewinsohn R.D, Maayan David R.D, Alona Hemo M.Sc, Orna Hermon B.A, and Rachel Nave.
Authors' Contributions
R.N., M.P., and N.K. contributed to the study design. J.N., N.L., M.G.K., I.M., and E.A. assisted with implementation of the study. N.F.S. contributed to the article writing and data interpretation. B.G. and A.R. participated in data analysis and review of the article. All contributing authors advised on analysis or interpretation of the data and all authors commented on and revised the article and approved the submission. R.N, the corresponding author, had access to the study data and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Author Disclosure Statement
R.N. reports receiving grants from Helmsley Charitable Trust, Dexcom, and Insulet; personal fees and other from DreaMed Diabetes Ltd.; personal fees from Novo Nordisk and Eli Lilly; grants from Medtronic; In addition, R.N. owns DreaMed Diabetes Ltd. stock and has a patent DreaMed Diabetes Ltd. licensed. B.G, R.A, and N.K are Medtronic employees. J.N., N.F.S., N.L., and M.G.K., declared no conflicts of interest. I.M. and E.A. are DreaMed Diabetes Ltd. employees and own DreaMed Diabetes Ltd. stock. M.P. reports receiving grants from Helmsley Charitable Trust, Dexcom, and Insulet; personal fees and other from DreaMed Diabetes Ltd.; grants and personal fees from Medtronic, Novo Nordisk, grants from Roche, Eli Lilly, and Sanofi; grants from Lexicon, OPKO; personal fees from RSP Systems and QuLab Medical; In addition, M.P. owns DreaMed Diabetes Ltd. stock and has a patent DreaMed Diabetes Ltd. licensed.
Funding Information
This was an investigator-initiated study. The study was supported by a grant from Medtronic, which also provided the study devices and consumables.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.