
Abstract
The high-dose large-volume insulin injections that may become necessary during pregnancy due to marked pregnancy-induced insulin resistance may result in suboptimal therapeutic effectiveness. Use of U-500 insulin, a concentrated insulin formulation, has been suggested during pregnancy. However, the pharmacokinetic properties of U-500 insulin monotherapy can impede achievement of strict pregnancy glycemic targets. We propose a novel regimen for treatment of severe pregnancy-induced insulin resistance that enables precise delivery of U-500 basal insulin therapy through continuous subcutaneous insulin infusion (CSII) while maintaining the desired kinetics of prandial rapid-acting U-100 insulin therapy. This combination approach, guided by continuous glucose monitoring data, enabled achievement of pregnancy glycemic targets while reducing basal insulin requirements by approximately one-third. We report our method for (1) conversion to U-500 insulin delivery through CSII during pregnancy and (2) conversion from U-500 basal insulin delivery through CSII to U-100 intravenous insulin infusion therapy at delivery, to offer clinicians who encounter similar challenging scenarios a novel approach to diabetes management during pregnancy in the setting of marked insulin resistance.
Introduction
Marked insulin resistance is well known to occur during the second and third trimesters of pregnancy as a result of placental hormonal production, and substantially increased insulin doses requiring large-volume insulin injections may become necessary with advancing gestation. 1 However, decreased therapeutic effectiveness may result from large-volume insulin injections as a result of suboptimal subcutaneous absorption, pain, and difficulties adhering to the prescribed regimen, 2 which can lead to further deterioration of glycemia.
U-500 regular insulin is a concentrated insulin formulation, and its use has been suggested during pregnancy 2 –6 in an effort to mitigate the obstacles imposed by large-volume insulin injections. Although U-500 regular insulin use has well-known benefits in nonpregnant people with severe insulin resistance, there are sparse data guiding its use during pregnancy. 6 U-500 regular insulin is typically administered as 3–4 injections per day that are intended to cover both basal and prandial insulin needs. 2 Its delayed peak of action and prolonged duration of action, however, can impede achievement of the strict postprandial glycemic targets recommended during pregnancy. 7 These pharmacokinetic properties can also increase the risk of insulin stacking and delayed hypoglycemia.
To this point, one case report described the need for combined use of U-500 regular insulin as basal insulin with additional rapid-acting U-100 prandial insulin injections during pregnancy, due to the observed glycemic patterns of persistent postprandial hyperglycemia with premeal hypoglycemia that occurred with U-500 regular insulin monotherapy. 5 However, the augmentation of U-500 insulin injections with consistent prandial administration of rapid-acting U-100 insulin injections would require many injections per day (up to 3–4 daily injections of U-500 basal insulin and up to 3–5 injections of U-100 insulin before meals and snacks). Furthermore, the inherent peaks and troughs of multiple overlapping insulin doses with varying pharmacokinetic profiles hinder replication of physiological insulin patterns.
We report a case of successful use of U-500 regular insulin administered through continuous subcutaneous insulin infusion (CSII) for basal insulin coverage combined with conventional rapid-acting U-100 prandial insulin injections through pen in a pregnant woman with severe insulin resistance. This therapy allowed optimal achievement of glycemic targets as evidenced by continuous glucose monitoring (CGM) data, with significantly reduced insulin requirements, as compared with administration of conventional basal and prandial multiple daily injections of U-100 insulin.
Although limited reports of U-500 regular insulin use during pregnancy are available, a standardized protocol for antepartum conversion to U-500 regular insulin administered through CSII has not been reported, nor has CGM data from the pregnancies in which U-500 insulin was used. We report our method for conversion from U-100 basal insulin therapy to U-500 basal insulin therapy administered through CSII, guided by CGM data. In addition, we report our method for conversion of U-500 basal insulin therapy to the intravenous U-100 insulin protocols commonly used during the peripartum period.
Case
We present a 40-year-old G1P0001 woman with pre-existing type 2 diabetes complicating pregnancy. Medical history was notable for polycystic ovary syndrome with anovulatory infertility, obesity (pregravid weight 277 lb [125 kg], body mass index 44.6), and history of laparoscopic left salpingoophorectomy and infundibulopelvic ligament resection for a stage 1 granulosa cell ovarian tumor diagnosed ∼1 year before pregnancy. Her prepregnancy diabetes regimen was insulin glargine 24 units once daily and metformin 1000 mg daily; prepregnancy hemoglobin A1c (HbA1c) was 6.8% (51 mmol/mol). Pregnancy was achieved through letrozole and recombinant human chorionic gonadotropin therapy.
First trimester HbA1c was 6.1% (43 mmol/mol) at 12 weeks gestation (goal during pregnancy <6% [42 mmol/mol] 7 ). Initial insulin regimen at the first prenatal visit was insulin detemir, 30 units twice daily, and insulin lispro, 12 units before meals. Insulin doses were progressively increased with advancing gestational age. Notably, fasting glucose remained elevated despite multiple serial increases in the insulin detemir dose. By 31 weeks gestation, average total daily dose (TDD) was 311 units/day (2.4 units/kg per day), of which 175 units daily was basal insulin detemir administered as 4 injections of 40–50 units every 6 h.
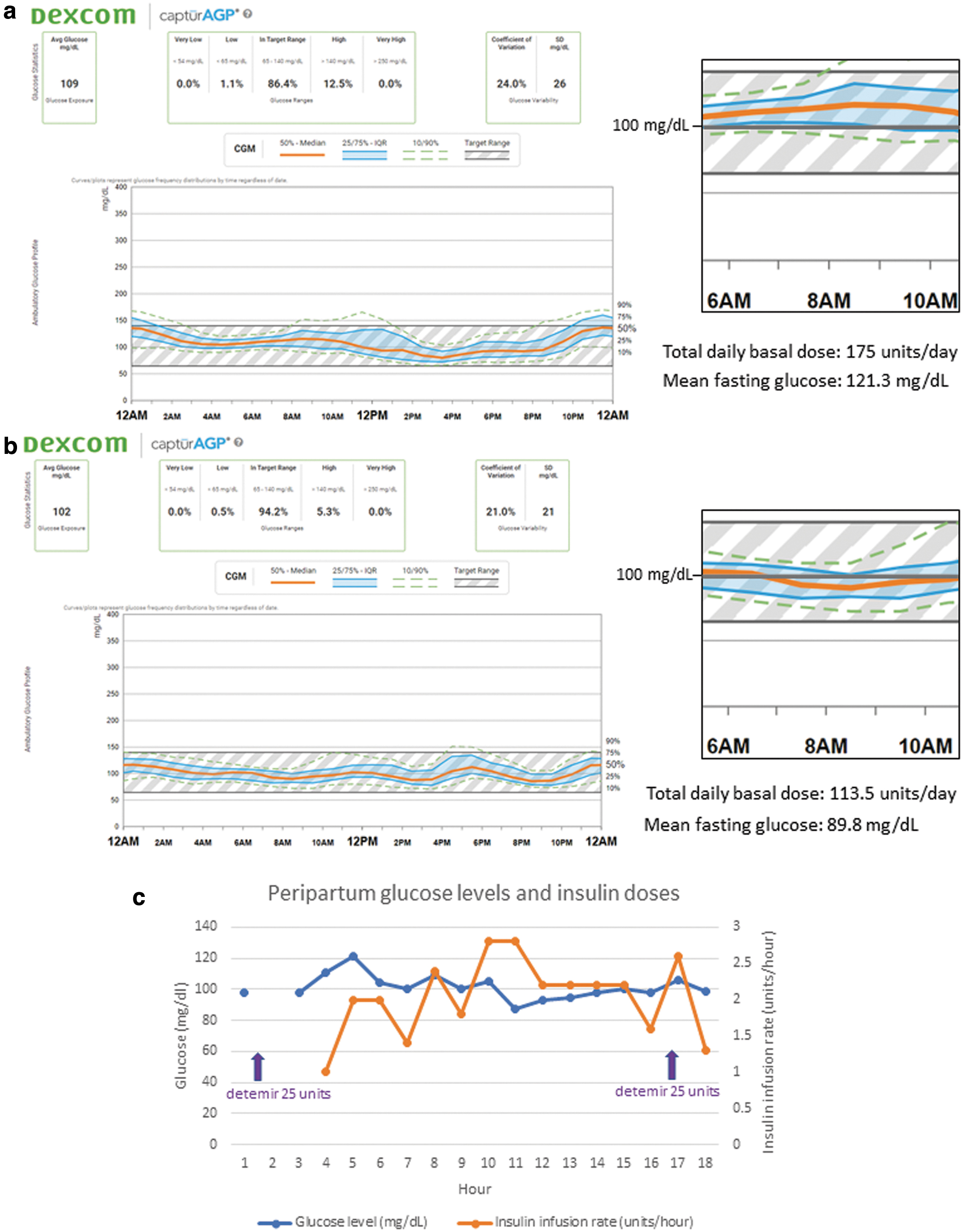
On this regimen, average fasting glucose (defined as mean of six consecutive values starting at 6:00 am and/or after at least 7 h fasting 8 ) remained above target at 121.3 mg/dL (target fasting glucose 70–95 mg/dL [3.9–5.3 mmol/L] 7 ; Fig. 1a). Given the suboptimal fasting glycemia and presumed suboptimal absorption of U-100 insulin at these doses, it was recommended to change the regimen from U-100 basal insulin through insulin detemir injection to U-500 insulin therapy through CSII.
A combined regimen of U-500 basal insulin therapy administered through CSII together with conventional prandial U-100 aspart injections through pen was chosen. U-500 regular insulin administered through CSII was chosen for basal insulin to allow more precise delivery of variable basal insulin rates, to match the variable basal insulin requirements observed over the day and night. The patient strongly preferred to continue conventional U-100 rapid-acting insulin injections through pen for prandial coverage due to her professed inability at work to administer mealtime U-500 insulin doses at least 30 min before meals as is recommended. 2
The continuation of conventional prandial U-100 rapid-acting insulin allowed the patient to administer the prandial insulin 15 min before meals. Administration of prandial U-100 rapid-acting insulin was also preferred due to the lower risk of overnight hypoglycemia, compared with U-500 insulin boluses, for which the duration of action is 6.5 to 10 h. 2
Basal insulin rates were calculated based on her TDD of 331 units/day of U-100 insulin. We modified the method of Grunberger et al. 9 to include an additional reduction of the pump TDD for the anticipated improved absorption upon changing from U-100 to U-500 insulin, as outlined in Table 1. We suggest empirically reducing the conversion dose by 10% to 20% if the HbA1c during pregnancy is 6.5% or lower (instead of the threshold of 8% recommended outside of pregnancy 2 ) to reflect the lower glycemic targets during pregnancy. 7
Calculations for Insulin Pump Settings Using U-500 Regular Insulin During Pregnancy
Modified from Grunberger et al. 9
Modified from Lane et al., 2 which recommends empiric reduction of conversion dose from U-100 by 10% to 20% if HbA1c <8% in nonpregnant population; lower A1c threshold selected recommended here is based on the lower HbA1c goals during pregnancy. 7
Adjusted by factor of 5 since U-500 regular insulin contains five times as much insulin in 1 mL as standard U-100 insulin.
HbA1c, hemoglobin A1c; ICR, insulin-to-carbohydrate ratio; ISF, insulin sensitivity factor; PU, pump units; TDD, total daily dose.
Per the method described in Table 1, the initial basal rate was 4.65 units/h (programed as 0.9 “pump units” (PU)/h in the insulin pump [Omnipod, Insulet Corporation, Acton, MA]). The insulin-to-carbohydrate ratio and insulin sensitivity factor were set as per Table 1, but the bolus calculator was not used by the patient, as she continued to administer prandial doses through U-100 aspart insulin pen.
Basal rates and prandial U-100 aspart doses were adjusted weekly based on glucose trends to achieve fasting glucose of 70–95 mg/dL (3.9–5.3 mmol/L) and 1-h postprandial glucose of 110–140 mg/dL (6.1–7.8 mmol/L). 7 Changes to the basal rates were initiated ∼2 h before the desired time of glycemic effect. 2 Soon after initiation of U-500 basal insulin through CSII, pregnancy fasting glucose targets were achieved. By 36 weeks gestation, basal rates were 12:00 am–7:00 am: 1.15 PU/h (5.75 units/h), 7:00 am–9:00 pm: 0.80 PU/h (4.0 units/h), 9:00 pm–12:00 am: 1.15 PU/h (5.75 units/h); total daily basal insulin 113.5 units/day.
On this regimen, mean fasting glucose decreased from 121.3 to 89.8 mg/dL, comparing the 14-day CGM period just before pump initiation with the 14-day CGM period before delivery. Notably, although fasting glycemia improved significantly, TDD of basal insulin decreased by 35% from 175 units daily of insulin detemir to 113.5 units/day of U-500 insulin administered through CSII, reflective of the expected improvements in absorption and effect resulting from use of both concentrated insulin and CSII (Fig. 1b). By the end of pregnancy, prandial U-100 aspart doses were 44 units before breakfast, 38 units before lunch, and 88 units before dinner.
Before delivery, third-trimester HbA1c at 36 weeks gestation was 5.7% (39 mmol/mol). At 37 weeks and 4 days gestation, the patient underwent induction of labor for superimposed pre-eclampsia on chronic hypertension; renal function was normal throughout the pregnancy. She was transitioned from U-500 regular insulin administered through CSII to the U-100 regular intravenous insulin infusion, and we simultaneously administered subcutaneous insulin detemir to lessen the anticipated high U-100 insulin hourly infusion rates required to transition from U-500 to U-100 regular insulin. Fifty percent of the anticipated 24-h intravenous insulin requirement, based on the starting hourly insulin infusion rate per institutional protocol (which was also equal to 0.2 units/kg every 12 h), was administered on arrival to the labor and delivery unit.
The insulin pump was removed 2 h after the first insulin detemir injection. The intravenous insulin infusion was adjusted hourly per the institutional peripartum insulin infusion protocol targeting intrapartum glucose 70–100 mg/dL. 10 Peripartum glucose levels and insulin doses are shown in Figure 1c. She underwent vaginal delivery of a female infant (birth weight 7 lb 1.1 oz (3.205 kg) with Apgar scores 8 and 9 at 1 and 5 min, respectively). Labor was complicated by shoulder dystocia of 40 s attributed at least, in part, to soft tissue obstruction. The infant did not have neonatal hypoglycemia. Postpartum, her diabetes regimen was insulin detemir 16 units twice daily and metformin 1000 mg daily; blood pressure was normal without antihypertensive therapy.
Discussion
Effective delivery of the large insulin doses required to overcome severe pregnancy-induced insulin resistance can be hindered by discomfort, inconvenience resulting from the need to divide insulin doses into multiple smaller injections, and the suboptimal absorption that results from a large subcutaneous insulin depot. 2 Although strict glycemic targets are of the utmost importance during pregnancy, these obstacles can impair both therapeutic effectiveness and patient adherence.
We report a novel therapeutic regimen combining U-500 regular insulin delivered through CSII used as basal insulin therapy with conventional U-100 prandial insulin injections during pregnancy complicated by severe pregnancy-induced insulin resistance. Although U-500 regular insulin use during pregnancy has been described in limited case reports and series, a standardized protocol for conversion to U-500 regular insulin administered through CSII is not currently available in the literature, nor is a protocol for conversion back to the U-100 intravenous insulin infusions commonly used in patients during the peripartum period. We report our method for (1) conversion to U-500 insulin delivery through CSII during pregnancy and (2) conversion from U-500 basal insulin delivery through CSII to U-100 intravenous insulin infusion therapy at the time of delivery.
Use of U-500 monotherapy for both basal and prandial insulin coverage during pregnancy has been reported but can be limited by both postprandial hyperglycemia and subsequent premeal hypoglycemia. 5 The pharmacokinetic profile of U-500 insulin, characterized by a delayed peak of action 11 and necessitating administration at least 30 min before meals for optimal effect, can make achievement of postprandial glycemic targets more difficult. Furthermore, the prolonged duration of action of U-500 insulin 11 predisposes to late postprandial and overnight hypoglycemia as well as insulin stacking when frequent meals or snacks are eaten, as is recommended as part of standard medical nutrition therapy during pregnancy. 12
The obstacles to U-500 regular insulin use for prandial insulin coverage are exacerbated during pregnancy compared with the nonpregnant state for several reasons. Outside of pregnancy, the permissive allowance of some degree of postprandial hyperglycemia mitigates the hypoglycemia risk with use of U-500 insulin for prandial coverage. During pregnancy, however, glycemic targets are lower and narrower than in the nonpregnant population, and achievement of postprandial glycemic control is a primary therapeutic target. 7
This narrower therapeutic window during pregnancy introduces a high risk of insulin stacking and hypoglycemia when U-500 insulin is used for prandial coverage during pregnancy. Our novel regimen combining U-500 regular insulin delivered through CSII used as basal insulin coverage combined with rapid-acting U-100 insulin injections for prandial coverage allowed us to successfully overcome these obstacles and to achieve pregnancy glycemic targets.
For these reasons, we propose a novel regimen for treatment of severe insulin resistance during pregnancy, which enables precise delivery of U-500 basal insulin therapy through CSII, while maintaining the desired kinetics of prandial insulin delivery afforded by rapid-acting U-100 insulin injections. In our patient, this combination approach enabled achievement of the recommended glycemic targets during pregnancy, while reducing total daily basal insulin requirements by approximately one-third.
Our therapeutic regimen was guided by real-time CGM data, which was not reported in previous descriptions of U-500 insulin use during pregnancy and provides important information regarding safety and therapeutic efficacy. Finally, we also report our method for conversion from U-100 basal insulin therapy to U-500 basal insulin therapy administered through CSII during pregnancy, as well as our method for conversion from U-500 regular insulin delivered through CSII to the U-100 intravenous insulin infusion therapy commonly used in patients in the peripartum setting.
We acknowledge that generalizability of our approach is limited by the need for a motivated patient and a diabetes treatment team comfortable with use of insulin pumps and concentrated insulin formulations. Though caution and vigilance are warranted until our protocol is validated in a larger population, publication of our novel regimen provides clinicians with a framework to adopt or adapt in this commonly encountered clinical scenario and may serve as springboard to studies evaluating its efficacy in a broader population.
Footnotes
Authors' Contributions
E.D.S. collected the data. E.D.S. and G.A. formulated the treatment plan and analyzed the data. E.D.S. and G.A. wrote the article. E.D.S. had full access to all the data and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Author Disclosure Statement
E.D.S. has no competing financial interests. G.A. has served as consultant for Dexcom, Inc., and Insulet Corporation and has received research support from Dexcom, Eli Lilly, and Insulet Corporation.
Funding Information
This study was supported by the Division of Endocrinology, Metabolism and Molecular Medicine at Northwestern University.