
Abstract
Background:
Adults with poorly controlled type 1 diabetes (T1D) who are missing meal boluses are typically excluded from clinical trials of diabetes technologies. We investigated the long-term real-life outcomes of the Tandem Control IQ automated insulin delivery (AID) system in adults with T1D who are missing meal boluses.
Methods:
In this single-center study with 30 adults with T1D, we evaluated efficacy (A1c and time in target range [TIR]) and safety (time below range [TBR]) in adults with T1D who initiated Tandem Control IQ with minimal or no user-initiated boluses (auto >90%) compared with age, gender, and diabetes duration matched adults with T1D with intermediate (auto 50%–90%) and high bolusing behaviors (auto 10%–49%).
Results:
Regardless of engagement with Control IQ system, there were significant improvements in A1c and TIR in all three groups over 3, 6, and 12 months. Compared with baseline, there was significant decrease in A1c by 1.6% ± 0.8% and increase in TIR by 19.3% ± 6.4% (P < 0.001 for both) over 12 months of Tandem Control IQ use in auto >90% use group without increasing TBR.
Conclusions:
Tandem Control IQ is effective in lowering A1c and improving TIR without increasing TBR regardless of users' engagement with the system. Therefore, adults with T1D with high A1c who are mostly missing meal boluses should not be considered as inappropriate candidates for Control IQ AID system.
Introduction
Significant improvement in diabetes technologies have led to improved glycemic control, patient-related outcomes, and decreased diabetes-related complications in type 1 diabetes (T1D). 1 Adults with T1D with high A1c (A1c >9%–10%) and missing meal boluses have not been considered as good candidates for insulin pump therapy, and generally excluded from clinical trials of diabetes technologies. 2 –5 The success of insulin pump therapy depends on basal/bolus settings, bolus frequency, self-monitoring blood glucose, and adherence to diabetes self-care management. 6
A survey study showed that majority of the endocrinologist (70%) use personal criteria to start insulin pump therapy. 7 Most of the criteria that have been used are using a certain upper limit of A1c, frequency of finger stick blood glucose monitoring, history of diabetic ketoacidosis, and frequency of health care provider visits. 7 None of these criteria are evidence based and it has been suggested that these may contribute to the health care disparities in the use of diabetes technologies among racial and ethnic minorities. 8
The Tandem Control-IQ automated insulin delivery (AID) system consists of the Tandem X2 insulin pump, a Dexcom G6 continuous glucose monitor (CGM) sensor, and a software algorithm that automatically adjusts basal insulin delivery to maximize the amount of time glucose is in target range. 9 The system works by automatically increasing the programmed basal insulin delivery rate when glucose levels are predicted to exceed 160 mg/dL. In addition to modulating the basal rates, the system can also deliver an automatic correction bolus dose of insulin if glucose levels are predicted to rise above 180 mg/dL. 9,10 This occurs up to once per hour during normal operation and delivers 60% of the dose calculated based on the user's insulin sensitivity factor.
Considering unique algorithm of Tandem Control IQ with hourly boluses and automated basal adjustment, we believe that generally perceived concept of not considering insulin pump and AID system in T1D adults with poorly controlled diabetes is not appropriate.
A recent subgroup analysis showed a significant reduction in glucose management indicator (GMI) and CGM metrics with Tandem Control IQ use over 12 months regardless of baseline estimated A1c (GMI >9% or GMI >10%). 2 However, the real-life long-term outcomes of Tandem Control IQ users that are not giving user-initiated boluses (missing mealtime boluses and/or corrections) have not been evaluated. We compared the efficacy (A1c and time in target range [TIR]) and safety (time below range [TBR]) over 12 months among T1D adults who initiated Tandem Control IQ with minimal or no user-initiated boluses (auto >90%) compared with age, gender, and diabetes duration matched T1D adults with intermediate (auto 50%–90%) and high bolusing behaviors (auto 10%–49%).
Methods
In this single-center study, 30 adults (age >18 years) with T1D duration >2 years and using continuous glucose monitoring (CGM) >6 months before Tandem Control IQ initiation were searched from medical records. Only patients who used Tandem Control IQ for >90% of the time over 12 months without any antidiabetic medications (e.g., GLP-1 RA or SGLT-2 inhibitors) were included in this study. Pregnant patients and patients taking steroids were excluded. This study was approved by the Colorado Multiple Institutional Review Board.
We identified adults with T1D (n = 10) who were on Tandem Control IQ with minimal or no user-initiated boluses (auto >90%). Auto bolus % is the percentage of bolus given by the system automatically and refers to the percentage makes up the total daily bolus. These patients were almost completely dependent for auto boluses since they did not give any boluses for meals or correction. We also identified age, gender, diabetes duration, and insulin pump use duration matched adults with T1D who were using Tandem Control IQ with intermediate (auto 50%–90%, n = 10) and high bolusing behavior (auto 10%–49%, n = 10).
Full 90 days of data on CGM and insulin delivery were extracted from T:Connect and/or Dexcom Clarity software every 3 months for total of 1 year to calculate CGM-based metrics such as TIR and TBR. We also collected data on A1c, weight, total insulin dose, basal insulin, and automatic correction bolus percentages over 1 year among these patients. Occurrence of severe hypoglycemia that requires third-party assistance and diabetic ketoacidosis collected from chart review.
This was a feasibility study and, therefore, sample size was not estimated and not powered to evaluate efficacy or safety outcomes. The data were presented as mean (standard deviation) or median (interquartile range) depending on normality of distribution or as percentage for categorical data. Efficacy was evaluated for reduction in A1c and improvement in TIR and safety was evaluated for CGM-based time spent below range (<70 and <54 mg/dL).
First, t-tests for univariate comparisons were used to compare mean A1c, TIR, TBR, weight, and insulin dose between three groups and then, change in these parameters over 1 year was compared over 3, 6 and 12 months for both within-group and between-group comparisons using linear mixed models. A P-value of <0.05 was considered statistically significant.
Results
Participants were matched on age, diabetes duration, and gender, and so as expected, there were no differences in these parameters by group (Table 1). Most of the participants were White reflecting the clinic population (70% White and 30% Hispanic and similar distribution in each group). At baseline, there was no statistical difference in A1c or CGM TIR between the three groups, but the auto 50%–90% group had a significantly higher weight than the auto >90% group (78.1 ± 7.5 vs. 70.8 ± 9.2, P < 0.05). Mean percentage of auto boluses were 27.7% ± 7.9% in the auto 10%–49%, 62.7% ± 5.7% in the auto 50%–90% and 93.1% ± 3.8% in the auto >90% and this bolusing behavior remained consistent within the group for throughout 1 year of follow-up.
Comparison of Baseline Characteristics Among Tandem Control IQ Users by Auto Bolus Percentages in Use
Data shown are mean ± SD and percentage.
SD, standard deviation; TIR, time in target range.
There was a significant improvement in A1c from baseline in all groups at 3, 6, and 12 months (P < 0.05 for all) in univariate within-group comparisons. Change in A1c is shown by group at the three time points in box and whisker plots (Fig. 1A). On average across all three groups, A1c improved by 1.6% ± 0.7% over 12 months of Tandem Control IQ use. At 6 months, the improvement in A1c was significantly greater in the auto 50%–90% group compared with the auto 10%–49% group, but no other between-group differences were observed for change in A1c in univariate models.
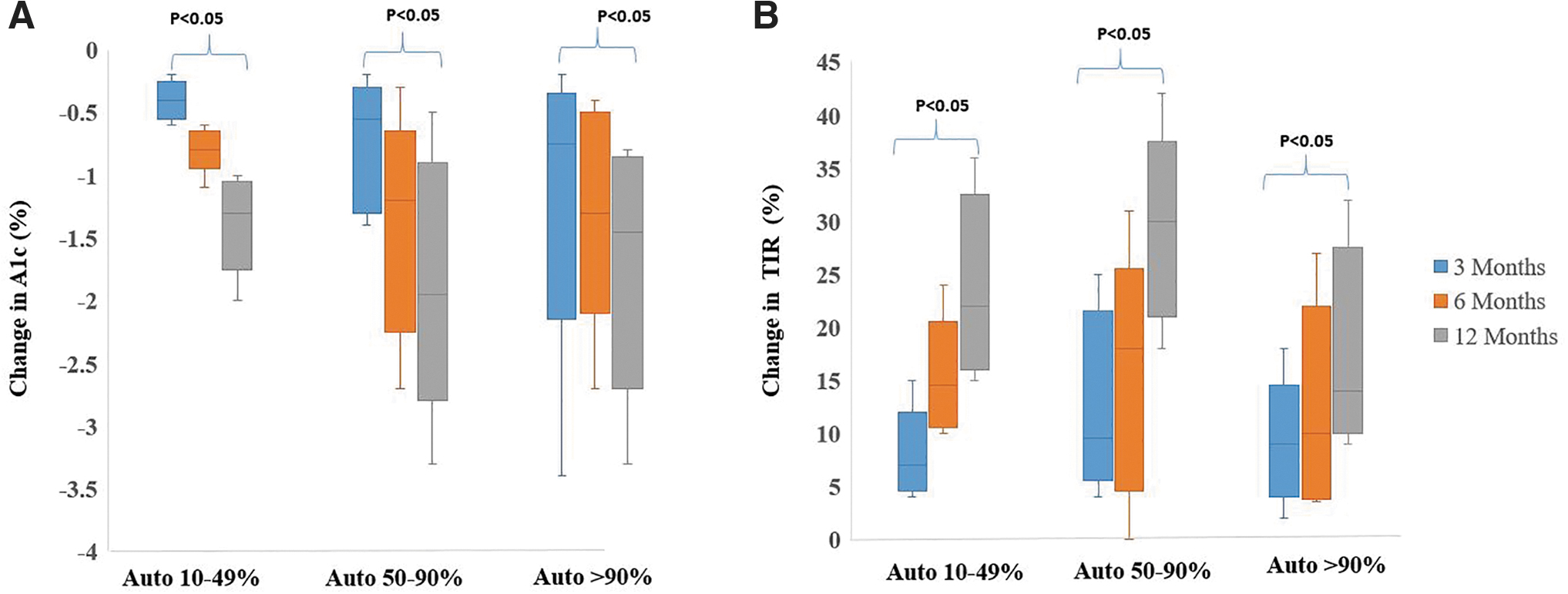
Change in A1c
CGM glucose TIR significantly improved from baseline at all time points for all three groups in the within-group comparison, with an overall mean improvement for all groups of 24% ± 8%. Change in TIR is shown by group at the three time points in box and whisker plots (Fig. 1B). There were significantly greater improvements in TIR in the 50%–90% auto group than in both the 10%–49% and >90% auto groups at 6 and 12 months. In addition, 3 out of 10 patients (%30) in auto >90% group achieved >70% TIR, international consensus target. Weight increased significantly in all groups at all three time points, but there was a greater increase in weight in the auto 50%–90% group at 12 months when compared with both the 10%–49% and >90% auto groups in univariate models (Table 2). There were no group differences at any time point in total daily insulin dose per kg body weight
Comparison of Tandem Control IQ Users by Auto Bolus Percentages in Use
Data shown are mean ± SD and %.
P < 0.05 compared with baseline.
P < 0.001 compared with baseline.
P < 0.05 compared with auto 10%–50% group.
P < 0.001 compared with auto 10%–50% group.
P < 0.05 compared with auto 50%–90% group.
P < 0.001 compared with auto 50%–90% group.
In linear mixed regression models adjusted for age, gender, and baseline A1c, there was no significant group effect on change in A1c over time (P = 0.07). For change in TIR, when adjusted for age, gender, and baseline TIR, there was a significant group effect over time (P = 0.024). At 3 months, there was no difference in the TIR by group, but at 6 and 12 months there was higher TIR in the auto 50%–90% group compared with both the auto 10%–49% and auto >90% groups. There was no overall difference in weight change by group over time (P = 0.37) in the linear mixed model adjusted for age, gender, and baseline weight. There were no severe hypoglycemia episodes that required third-party assistance and no instances of diabetic ketoacidosis in any group during the study as retrospectively reviewed.
Discussion
Our study suggests glycemic benefits of Tandem Control IQ in patients who were traditionally denied insulin pump therapy or hybrid closed-loop system due to high A1c and less adherence to diabetes self-management. This is the first study to show significant improvement in A1c and CGM metrics with Tandem Control IQ initiation in patients with T1D that had <10% user-initiated boluses.
Hybrid closed-loop pumps still require user input for meals and some corrections. Previously, the importance of bolusing and adjustment of insulin-carb ratio was shown in earlier hybrid closed-loop systems. 11,12 Tandem Control IQ has the capability of giving auto boluses as detailed in the introduction. For optimal glycemic control, users should bolus before meals and can also give user-initiated correction boluses. However, there are many patients who are not using the bolus feature as frequently as suggested for different reasons, for example, older adults with cognitive issues or young adults with busy schedules.
Traditionally, these patients are not considered good candidates for insulin pump therapy due to relatively high A1c and perceived negative bolusing behaviors. Actually, these patients' A1c are higher due to not bolusing with meals. In this study, we investigated the long-term outcomes of a hybrid closed-loop pump with auto bolus capabilities. Auto bolus is important for auto correction boluses to keep blood glucose in range in most of the users who bolus with meals; however, in patients who are not bolusing enough with meals, the auto bolus feature is the major determinator for improved glycemic results.
We still advocate using meal-time boluses and user-initiated correction boluses if necessary, in Tandem Control IQ users for optimal glycemic control. However, we think these data show compelling evidence that hybrid closed-loop pumps using Tandem Control IQ can achieve large improvements in glycemic control even among people who are not bolusing as seen in auto >90% group. In addition, in our study, auto 50%–90% group achieved better glycemic control compared with auto 10%–49% and auto >90%; it shows that overbolusing as much as underbolusing is a barrier to achieve optimal glycemic control and that emphasizes the importance of auto bolus feature in this system.
In consideration of the emerging studies, we should, therefore, not exclude patients who are not bolusing regularly from starting auto bolus-enabled hybrid closed-loop pumps. We believe the various pump initiation criteria that are used by providers should be evidence based and should be revised for auto bolus-enabled hybrid closed-loop pumps. Eliminating a major population with T1D from diabetes technology clinical trials and clinical use would further worsen the health care disparities in diabetes care. 13
Strengths of this study are that it is the first study of real-life outcomes of Tandem Control IQ users who relied almost completely on auto bolus corrections and using well-matched comparisons in a long-term (1 year) follow-up. Limitations of this study are the retrospective single-center design and we did not collect any patient-related outcomes and quality of life measurements. Use of sleep mode in different durations may also affect these results. These results should be further confirmed in larger prospective clinical trials.
Conclusion
The use of Tandem Control IQ is safe and effective in lowering A1c and improving TIR without increasing TBR in adults with poorly controlled T1D with missing meal boluses. Therefore, patients with higher A1c with missing meal boluses should not be excluded from clinical trials or offering hybrid closed loop (HCL) therapy in clinical practice.
Footnotes
Authors' Contributions
H.K.A. and V.N.S. designed the study. H.K.A. did data extraction. J.S.B. did data analysis. All authors read and approved the article.
Author Disclosure Statement
H.K.A. received research support through University of Colorado from Senseonics, Dexcom, Medtronic, REMD, Eli Lilly, IM Therapeutics, and IAFNS. V.N.S. received research support through University of Colorado from Sanofi, NovoNordisk, Eli-Lilly, Dexcom, Insulet, Abbott, JDRF, and NIH. V.N.S. received speaking fees or honorarium through University of Colorado from Dexcom, Insulet, Medscape, and Lifescan. J.S.B. has no conflict of interest.
Funding Information
No funding was received for this article.