
Abstract
Objective:
The use of continuous glucose monitoring (CGM) systems and continuous subcutaneous insulin infusion (CSII) devices adhering to the skin can lead to skin reactions. The objective was to determine the prevalence and consequences of skin reactions at CGM or CSII sites in a large unbiased population.
Research Design and Methods:
This is a cross-sectional multicenter study. All adult patients with diabetes seen in consultation over a period of 7 months and using or having used a system with skin adhesives (in the last 10 years) were included and filled out a self-assessment questionnaire.
Results:
Among 851 patients, skin reaction was reported in 28% with CGM and 29% with CSII. Patients reporting reactions were more frequently women using CGM and CSII, and CGM users had type 1 more often than type 2 diabetes (P < 0.001). Manifestations were similar for reactions to CGM and CSII: redness and pruritus in 70%–75% of patients with reactions, pain in 20%–25%, and vesicles and desquamation in 12%–15%. Manifestations occurred within the first 24 h of first use in 22%–24% of patients with reactions to CGM and CSII, but after more than 6 months in 38% and 47% of patients with reactions to CGM and CSII, respectively. Device use was definitively stopped in 12% of patients with reactions to CGM (3.2% of all users) and 7% with reactions to CSII (2.1% of all users).
Conclusions:
Skin reactions were common, with similar presentations in CGM and CSII users. Manifestations suggested skin irritation rather than allergies. These reactions rarely led to the definitive discontinuation of the use of the device.
Introduction
Continuous subcutaneous insulin infusion (CSII) is one of the gold standards for achieving glucose control in patients with type 1 diabetes. 1 –3 Continuous glucose monitoring (CGM) is combined with CSII or multiple daily injections of insulin to adjust insulin doses and can reduce glycated hemoglobin (HbA1c) levels in patients with type 1 and type 2 diabetes. 4 –6 Moreover, CGM and CSII are components of automated insulin therapy, which are expected to be widely used in the coming years. 7
Thus, the use of devices adhering to the skin for 3–14 days in patients with diabetes is constantly increasing. Unfortunately, skin intolerance reactions such as redness, desquamation, pruritus, sores, and infections are increasingly reported with these systems. 8 –13 An article reviewed the cases of allergic contact dermatitis (ACD) caused by insulin pumps and glucose sensors reported since the 1970s, culprit allergen(s), results of patch tests and/or chromatographic analysis, and preventive measures. 14
However, the precise semiological description of this skin intolerance and its prevalence in a large, unselected population are not known. Above all, the rate of permanent discontinuation of these systems due to skin intolerance must be established.
Our objective was to address these questions in a large, multicenter, retrospective cross-sectional study.
Research Design and Methods
Trial design
This is an observational, cross-sectional multicenter study involving four university hospital diabetology departments: Cochin Hospital, Lariboisière Hospital, Pitié-Salpêtrière Hospital, and Bichat–Claude Bernard Hospital, all members of Assistance Publique–Hôpitaux de Paris (APHP, France). Oral consent was provided by all participants and was reported in the electronic medical record.
The study design was approved by the ethics committee (Comité de Protection des Personnes Sud-Méditerranée I, ID RCB 2019-A03208-49) and has been registered with ClinicalTrials.gov, identifier NCT04853810.
Trial population
Based on a population of 1800 patients using adhesive devices, the sample size to estimate the prevalence of skin reactions (with a 3% margin of error) was 671 (calculated with
Concerned devices were insulin patch for tubeless CSII (e.g., OMNIPOD®,
Trial procedure
After giving consent, the patients completed a survey on a digital tablet. The questionnaire was developed using the Memento Database software (MementoDB, Inc.), with about 50 questions concerning demographic information, diabetes characteristics, use of CSII and CGM devices, history of atopic manifestations (asthma, eczema, and food allergies), and the description and consequences of potential skin reactions.
Several temporal parameters are retrieved to observe any changes over time: year of first use of each device for all individuals, year of first use of the device associated with a skin reaction, and time between the first use of the device and the first skin reaction. Scarring at the catheter insertion site was not considered a skin reaction.
The complete form is available in the Supplementary Material. This study was conducted between May 2021 and November 2021.
Outcomes and objectives
The primary endpoint was the prevalence of skin reactions to CSII and CGM independently, calculated by the ratio of the number of patients with a skin reaction to the total number of patients included in the study. Secondary endpoints were the semiological description of these skin reactions; clinical characteristics associated with these reactions; and consequences of the use of the devices, that is, avoidance strategies, change of devices, and potentially definitive discontinuation.
Statistical analyses
Nonparametric tests were used for quantitative values (Mann–Whitney or Kruskal–Wallis test) and the chi-squared test or Fisher's test for qualitative values. To assess clinical characteristics that were associated with skin reactions, we first performed univariate analyses, followed by logistic regression analyses, including all criteria associated with a P-value <0.05 in the first analysis.
All statistical analyses were done using the R software (version R 4.1.0), and figures were plotted with the R package, ggplot2, v3.3.5. 15
Results
Description of the population
We included 851 patients: 833 were CGM users and 374 were CSII users. Clinical data for CGM and CSII users are reported in Tables 1 and 2, respectively. Among CGM users, the median age was 46 (interquartile range [IQR] 34–60) years, 54% were women, and 76% lived with type 1 diabetes, as opposed to 15% with type 2 diabetes and 9% with another type of diabetes.
Clinical Characteristics of Continuous Glucose Monitoring Users According to the Presence of a Skin Reaction
Median (IQR) or n (%).
Data are n (%) for categorical variables and median (IQR) for continuous variables. Pearson's chi-squared test and Wilcoxon rank sum test were used. Model adjustment: age, sex, BMI, type of diabetes (type 1 as reference), insulin duration, and eczema.
CSII users among CGM users.
Reaction to CSII among CGM users with CSII.
BMI, body mass index; CGM, continuous glucose monitoring; CSII, continuous subcutaneous insulin infusion; HbA1, glycated hemoglobin; IQR, interquartile range.
Clinical Characteristics of Continuous Subcutaneous Insulin Infusion Users According to the Presence of a Skin Reaction
Median (IQR) or n (%).
Data are n (%) for categorical variables and median (IQR) for continuous variables. Pearson's chi-squared test and Wilcoxon rank sum test were used. Model adjustment: age, sex, BMI, type of diabetes (type 1 as reference), insulin duration, and eczema.
CGM users among CSII users.
Reaction to CGM among CSII users with CGM.
Diabetes was diagnosed, on average, 21 years before the study (IQR 13–30), with insulin use for an average of 19 (IQR 10–29) years. Regarding CSII users, 62% were women, with a median age of 40 (IQR 30–52) years, 91% lived with type 1 diabetes, and diabetes duration was on average 22 (IQR 14–31) years, with insulin use for an average of 21 (IQR 14–30) years.
Semiological description
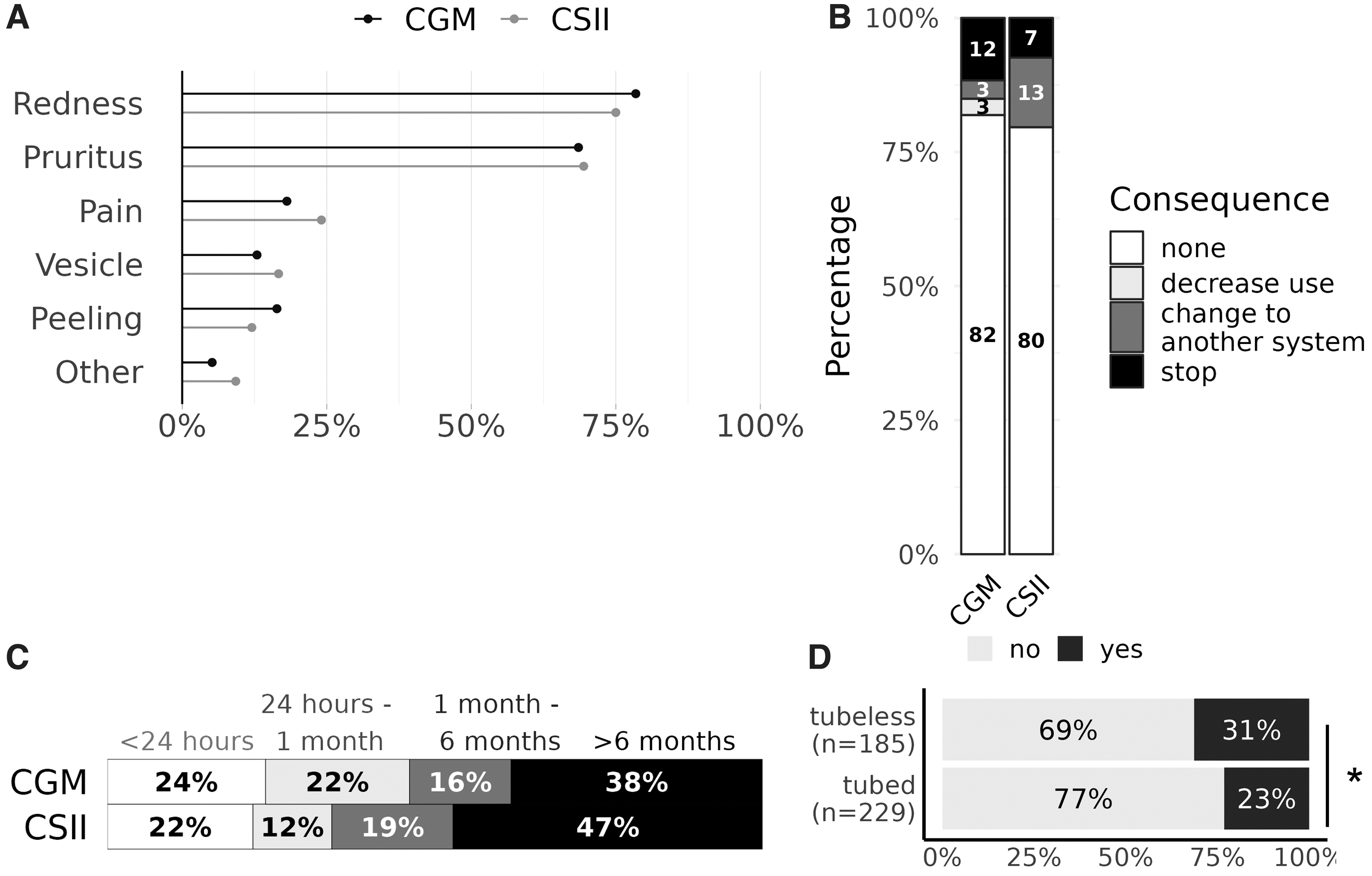
Among people with skin reactions (Fig. 1), similar prevalence rates for each sign or symptom were reported for both CGM and CSII and were, respectively, pruritus 69% and 69%, redness 78% and 75%, pain 18% and 24%, vesicles 13% and 17%, and desquamation 16% and 12% (Fig. 2A). These skin reactions were no larger than the adhesive in 89% of cases using CGM and 93% using CSII.
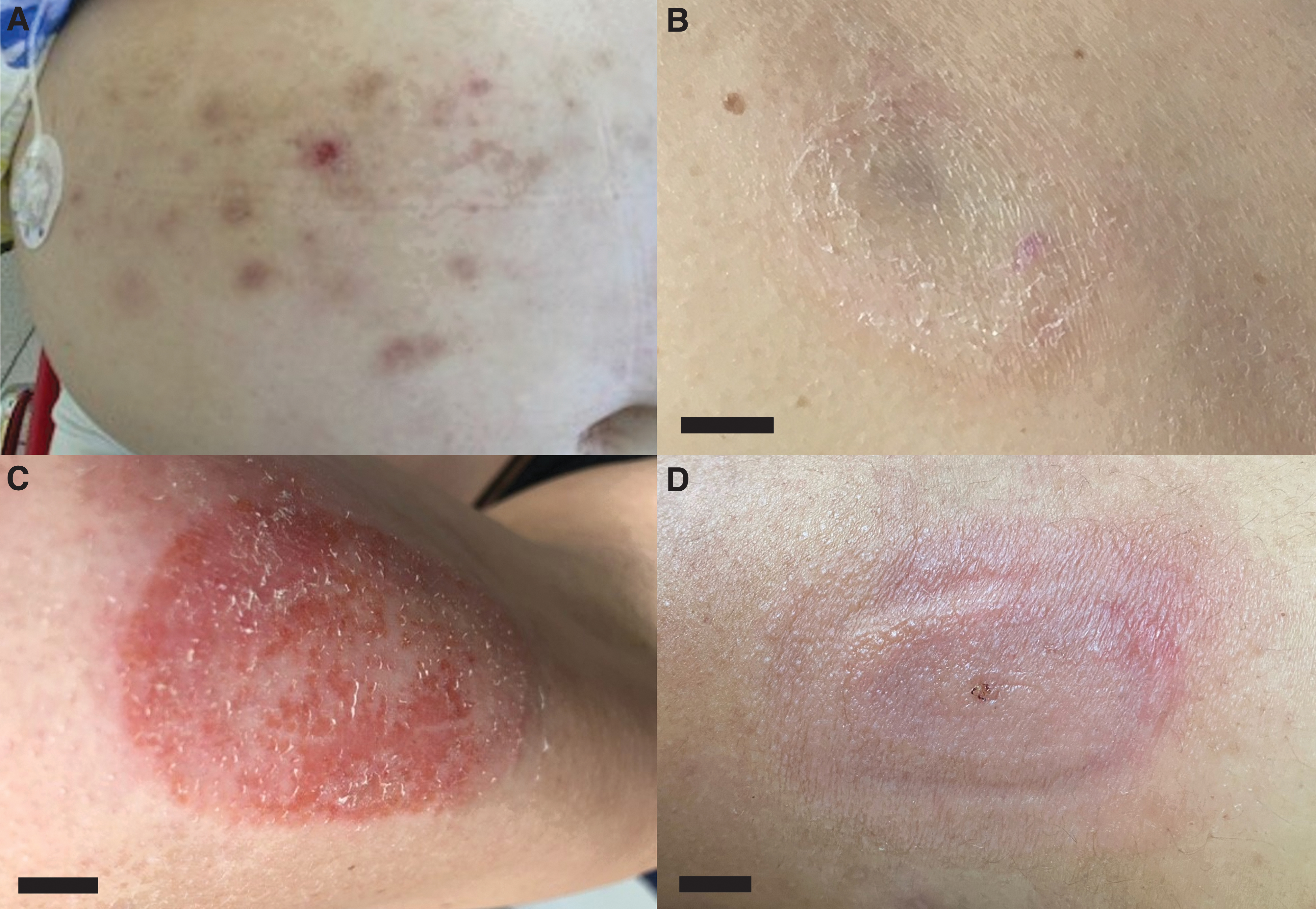
Skin lesions secondary to CSII or CGM: redness secondary to tubed CSII device use
For CGM users, manifestations resolved within 24 h in 29% of reactions, but lasted more than a week in 33%, and for CSII users, the rates were 20% and 27%, respectively. A permanent lesion (dark spots, scars, or hypochromic maculae) remained in 4.8% of patients with skin reactions to CGM (11/231) and in 0.9% with reactions to CSII (1/108).
Skin reaction prevalence and determinants
The prevalence of skin reactions was similar among CGM and CSII users: 28% (231/833) versus 29% (108/374). Among CGM users, those with a skin reaction, compared with those without, were more often female (63% of patients vs. 50%, P < 0.001), more often had type 1 diabetes (84% vs. 73%, P < 0.001) and a history of eczema (13% vs. 7%, P < 0.001), and were younger and thinner (detailed results in Table 1).
In a multivariate model (including age, sex, BMI, type of diabetes, insulin duration, and history of eczema), sex (P = 0.005, odds ratio [OR] 0.632, 95% confidence interval [CI] [0.456–0.871] for male patients), type of diabetes (P = 0.04, OR 2.135 [1.070–4.504] for type 1 diabetes), and a history of eczema (P = 0.02, OR 1.887 [1.098–3.210]) were independently associated with development of skin reactions. The skin reactions recurred with each sensor for 42% of the individuals, but with less than one out of two sensors for 44% of the individuals.
Concerning CSII use, patients with a skin reaction were also more often female (73% vs. 58%, P = 0.006) and had longer insulin use (24 [16–32] vs. 20 [14–30] years, P = 0.04) and a higher prevalence of history of eczema (20% vs. 5%, P = 0.003) than patients without skin reactions (detailed results in Table 2). In the same multivariate model, only sex (P = 0.007, 0.491 [0.289, 0.817], for male patients) and history of eczema (P = 0.0001, OR 4.157 [2.009–8.850]) were independently associated with development of skin reactions. The skin reactions recurred with each catheter or tubeless CSII for 33% of the individuals, but with less than one out of two for 58% of the individuals.
Skin reactions to CGM and CSII were significantly associated. Among 364 patients using both CGM and CSII, patients with a reaction to CGM were more likely to have a reaction to CSII, compared with patients without a reaction to CGM (relative risk [RR] = 2.4; 95% CI 1.8–3.3). Inversely, patients with reactions to CSII had more reactions to CGM (RR 2.5, 95% CI 1.8–3.4).
On the other hand, in this population using both CGM and CSII, 50% of patients with a skin reaction to CGM had no reaction to CSII (Table 1), and conversely, 51% of patients with a skin reaction to CSII had no reaction to CGM (Table 2). Among patients previously exposed to CSII with reactions, and using CGM, there was no association between the risk of skin reaction to CGM and how long the subjects had been using CSII or how severe their reactions were.
Outcome in patients with skin reactions
CGM and CSII usage was unchanged in 82% and 80% of patients with skin reactions, respectively. On the other hand, these skin reactions led to discontinuation of use in 12% of CGM users with cutaneous intolerance (3.2% of all CGM users, 27/833) and 7% of CSII users with cutaneous intolerance (2.1% of all CSII users, 8/374). In the remaining cases, patients changed to another device or decreased usage (Fig. 2B). There was no difference between CGM and CSII (P-value = 0.08).
Among patients changing to another device, no cutaneous reaction occurred in 88% (n = 7/8) of CGM users and 93% (n = 13/14) of CSII users. Manifestation duration was associated with discontinuation of CGM use: 3% of manifestations resolved within 24 h (2/67), 16% between 24 h and 1 week (10/87), and 25% after 1 week (15/75) (P = 0.001). This association was not found for CSII usage: manifestation duration was <1 day for 5%, (1/21), 1 day–1 week for 9% (5/54), and >1 week for 4% (1/28) (P = 0.10).
The first sign or symptom appeared within 24 h of the first use of the device for 24% of patients with reactions to CGM and 22% with reactions to CSII. However, this first reaction occurred more than 6 months after initiation for 38% of patients with reactions to CGM and 47% with reactions to CSII (Fig. 2C). There was no difference between CGM and CSII (P-value = 0.12). The cessation of device use did not differ according to the time of appearance of the first manifestation in CGM or CSII users.
In addition, cessation did not differ before and after 2019 for FreeStyle Libre users, the year FreeStyle Libre's glue composition was modified. 13
Reaction according to device type in CSII users
Skin reactions were more frequent for tubeless than for tubed CSII devices (31% vs. 23%, P = 0.04) and appeared earlier for tubeless CSII devices (Fig. 2D). The delay of the first reaction for tubeless versus tubed CSII devices was, respectively, <24 h, 31% versus 13%; 24 h–1 month, 15% versus 9%; 1–6 months, 20% versus 17%; and >6 months, 35% versus 60% (P = 0.04).
On the other hand, there was no difference for the type and number of manifestations, manifestation duration, or device discontinuation (Supplementary Table S1) between tubed and tubeless CSII devices. No semiological difference was found according to the type of CGM device (Supplementary Table S2).
Avoidance strategies
Among the 231 patients with skin reactions to CGM, 39 individuals changed the location, this being sufficient to decrease manifestations for 14 of them. Fifty-seven patients used an interface between their skin and the device (25%). Among the 180 patients with skin reactions to CSII, 26 patients changed the location, with a decrease in manifestations for 14, and 34 used an interface (31%). Only 3% of patients with skin reactions saw a dermatologist.
Discussion
In this large multicentric cohort, we report a high prevalence, about 25%, of skin reactions to either CSII or CGM, with redness and pruritus as the main manifestations. However, such skin reactions were associated with a device discontinuation rate of about 2%–3%. Manifestations were similar for tubed and tubeless CSII devices and all types of CGM devices.
Assessment of skin reaction frequency is particularly crucial since skin-adhesive devices are becoming common in the treatment of diabetes. With the advent of closed-loop insulin administration, skin reactions may occur and could thus limit its use. Several studies report the prevalence of contact dermatitis, but only with biased dermatology recruitment and in small cohorts 8,10,11,13 or only in children. 9
In our study, all patients seen in consultation and using or having used CSII and CGM (in the past 10 years) completed a survey, making it possible to define the actual prevalence of skin reactions, which was 28% and similar for CSII and CGM. A previous study 16 reported an even higher prevalence of 43%, but it concerned only 54 children with type 1 diabetes using CSII, without discontinuation of use.
In contrast to this high prevalence, skin reactions led to discontinuation of device use in only 2%–3% of concerned individuals. However, within the group having skin reactions, the discontinuation rate was 12% for CGM and 7% for CSII, suggesting that the risk of device discontinuation, especially CGM, is high for those experiencing skin reactions: more than 1 of 10 people experiencing skin reactions will stop using CGM or reduce their use of CGM.
Clinicians need to assess skin reactions and identify better solutions to manage skin reactions, and device manufacturers need to be diligent in reducing irritants in adhesives. It is important for the clinician to note that a reaction associated with the device could occur both in the days following its initiation and more than 6 months later.
Furthermore, such skin problems resulting from treatment with technology are associated with increased disease burden among adults with type 1 diabetes. 17 However, this prevalence is for adults only without ethnicity information, and more research is needed to identify the prevalence of skin reactions in youth using diabetes devices and the impact of skin reactions on device discontinuation.
Some patients with skin intolerance tried to change the location (17% and 14% using CGM and CSII, respectively), with partial success (<50%). Some others used an interface between the skin and the device (25%). However, our study could not evaluate the efficacy of this solution. In a study including 57 patients referred to the dermatology department because of skin reactions with FreeStyle Libre, barrier films had limited value in prevention. 11
We cannot precisely determine the physiopathology of these skin reactions, but reactions seem to be irritative rather than allergic in the vast majority of patients based on several arguments. First, reactions were no larger than the adhesive in 89% (CGM) and 93% (CSII) of patients, whereas an allergic reaction tends to extend beyond the adhesive area. Second, an allergic reaction reappears with each use, with increasingly shorter delays, which was not the case in our patients.
On the other hand, skin reactions were more frequent in patients with type 1 diabetes compared with other types of diabetes and in patients with a history of eczema. The prevalence of ACD caused by isobornyl acrylate (IBOA, one of the main allergic molecules in adhesives) was 3.8% in a previous study, 11 close to the discontinuation rate in our study. Interestingly, the only characteristic associated with discontinuation in our study was manifestation duration for CGM, with the probability of discontinuation increasing with manifestation duration.
Finally, cortisone ointment is used by several patients, generally with very good results—six patients with skin reaction to CSII and two to CGM used it in our study. However, both irritative and allergic reactions regress with this treatment, making it difficult to specify the etiology, which could be multifactorial. In our cohort, the number of referrals to dermatologists was low, around 3%, because only more severe or atypical lesions were the subject of a dermatology consultation and some lesions had not been reported to the diabetologist.
Another limit concerns the composition of the glue, protected by industrial secrecy, which we cannot directly relate to the reactions. Only targeted analyses with cutaneous tests, including selected molecules, can be performed. 18 In particular, IBOA was identified as a main allergen in FreeStyle Libre®. 19 In the newer models of FreeStyle Libre 2, no IBOA could be detected. 20
In the meantime, IBOA was also detected in the Omnipod patch pump 21,22 and in Medtronic's Enlite sensor, both in the sensor housing itself and in the skin patch. 23 –25 In contrast, IBOA has not yet been detected in either the patch or the sensor of DexCom G5 and G6. 23,26 In a conflicting study, however, a small quantity of IBOA was detected in DexCom. 27
IBOA remains an important allergen that requires patch testing. Some report that colophonium was the most frequently isolated sensitizing allergen (41.1% of cases). 28 Its presence in the adhesive of insulin sets and glucose sensors has been confirmed by the manufacturers of several devices, especially in Enlite in combination with the Medtronic® pump. 10 It is not included in FreeStyle Libre and DexCom. Therefore, it is crucial that manufacturers provide maximum transparency regarding patch and adhesive composition and communicate component changes.
While there was no difference in the reaction prevalence between CGM device types, we report a higher reaction rate for tubeless CSII compared with tubed CSII devices, possibly because the glue needs to be more powerful for tubeless CSII devices. For example, the tubeless Omnipod system measures 52 × 39 mm and weighs 25 g, compared with 35 × 35 mm and <1 g for the MiniMed™ Mio™ infusion set. Whereas Abbott changed the composition of the glue in its CGM FreeStyle Libre in 2019, 13 no difference in the incidence of these reactions or in discontinuation of FreeStyle Libre was found before/after this year in our cohort.
The last limit of our study is the use of self-questionnaires without dermatological expertise and the retrospective nature dependent on patients' memories. However, this method makes it possible to assess patient feelings without recruitment bias.
In conclusion, device skin reaction is more frequent than expected. Manufacturers must take into account these intolerance reactions to modify their components, in particular the glues in CGM and CSII devices. However, device discontinuation is observed in only a low percentage of patients, which is reassuring for closed-loop diffusion, including both CSII and CGM.
Footnotes
Acknowledgments
The authors would like to thank Eric Vicaut's team from the Fernand Widal Clinical Research Unit for the time taken to submit this study to the Comité de Protection des Personnes Sud-Méditerranée.
Authors' Contributions
A.S.-G., J.-P.R., and M.D. designed the study, conducted the analysis, and wrote the article. E.L. contributed to discussion and reviewed the article. C.P. designed the study, contributed to the discussion, and reviewed the article. A.C., L.P., A.H., S.J., T.V.-T., J.-F.-G, D.D.L., G.F., R.R., and J.-B.J. reviewed the article. J.-P.-R. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of data and accuracy of the data analysis.
Author Disclosure Statement
J.-B.J. reports grants, personal fees, and nonfinancial support from Novo Nordisk, Sanofi, and Eli Lilly. L.P. reports grants, personal fees, and nonfinancial support from Bayer, Novo Nordisk, Sanofi, Eli Lilly, Boehringer Ingelheim, and AstraZeneca. A.S.-G. is an advisory panel member for Abbott, Medtronic, and Lilly. J.P.R. is an advisory panel member for Sanofi, MSD, Eli Lilly, Novo Nordisk, Abbott, Alphadiab, Air Liquide, and Medtronic and has received research funding from and provided research support to Abbott, Air Liquide, Sanofi, and Novo Nordisk. Other authors have no conflicts of interest related to this work.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.