
Abstract
Background:
We assessed changes in glycemic control and person-reported outcome measures (PROMs) with t:slim X2 insulin pump with Control-IQ technology use among historically minoritized youth who are least likely to access hybrid closed loop (HCL) technology.
Methods:
This single-arm, prospective pilot study enrolled 15 publicly insured, insulin pump-naïve, non-Hispanic Black youth ages 6 to <21 years with type 1 diabetes and hemoglobin A1c (HbA1c) ≥10% in a 6-month study of HCL use. The primary outcome was absolute change in time in range (TIR) (70–180 mg/dL). Secondary outcomes included other continuous glucose monitor metrics, PROMs, and diabetic ketoacidosis (DKA) incidence.
Results:
For 13 youth (median 14.8 years, 53.3% female, HbA1c 11.7%) who completed the study, baseline TIR of 12.3% (6.3–27.1%) increased 23.7%-points (16.9, 30.5%; P < 0.001) or 5.7 h per day. Percent time >250 mg/dL decreased 33.9%-points (−44.8, −23.1%; P < 0.001) or 8.1 h per day from a baseline of 69.4% (51.6, 84.0%). Median time in HCL was 78.3% (59.7, 87.3%). Youth received 10.1 (9.2, 11.9) boluses per day, 71.7% (63.8, 79.3%) of which were HCL-initiated autoboluses. Diabetes-specific quality of life increased among parents (P < 0.001) and youth (P = 0.004), and diabetes distress decreased in both groups (P < 0.001, P = 0.005). Improvements in glycemia did not correlate with any baseline youth or parent PROMs. DKA was high at baseline (67 episodes/100-person years) and did not increase during the intervention (72 episodes/100-person years, P = 0.78).
Conclusion:
Improvements in glycemic control and quality of life exceeding pivotal trial findings without increased safety risks among historically minoritized youth emphasize the need for equitable access to HCL systems.
ClinicalTrials.gov:
Introduction
The use of insulin pumps and continuous glucose monitors (CGMs) among youth with type 1 diabetes has increased dramatically over the past decade but has also highlighted pre-existing health care inequities among people of different races, ethnicities, and socioeconomic statuses. 1 –6 Data from the Type 1 Diabetes Exchange (T1D Exchange) in 2020 showed that hemoglobin A1c (HbA1c) values were 2% higher, rates of CGM use were 23% lower, and rates of insulin pump use were 19% lower among non-Hispanic Black (NHB) individuals than among non-Hispanic White (NHW) individuals. 5 The characteristics of participants in randomized controlled trials of diabetes technologies mirror the racial/ethnic and socioeconomic inequities seen with real-world diabetes technology use. 7 Furthermore, studies to date have largely excluded youth with HbA1c values ≥10% despite evidence that those with the worst glycemic control have the greatest benefits with hybrid closed loop (HCL) system use. 8 –10
Interventional studies assessing the risks and benefits of HCL use among those who have historically been least likely to access these technologies are needed. We assessed changes in glycemic control and person-reported outcome measures (PROMs) during 6 months of Tandem t:slim X2 insulin pump with Control-IQ technology use among historically minoritized youth with suboptimal glycemic control.
Materials and Methods
Study oversight
This pilot study was approved by the Children's National Hospital institutional review board (Pro00013963) and was registered at
Study design and participants
Youth meeting the following criteria were eligible to participate: aged 6 to <21 years, NHB race and ethnicity, publicly insured to ensure ongoing access to HCL after study completion, type 1 diabetes managed with insulin ≥1 year, insulin pump naïve, HbA1c ≥10% upon enrollment and a second HbA1c ≥10% in the 2 years before enrollment, a total daily insulin dose of at least 10 U per day, and English fluency. Exclusion criteria included use of noninsulin diabetes medications, ≥3 episodes of diabetic ketoacidosis (DKA) in the year before enrollment, pregnancy, major illnesses other than type 1 diabetes, and significant cognitive limitations or major psychiatric disorders in the parent or child. Fifteen youth were enrolled between July 12, 2021, and May 24, 2022.
Point-of-care HbA1c values (DCA Vantage Analyzer; Siemens Healthineers, Erlangen, Germany) were used for eligibility screening and at study visits. Baseline CGM data on the usual diabetes care regimen were collected to be used as a comparator to the HCL period. To reduce observation bias, CGM data from 14 days prior enrollment were collected for youth who were previously using CGM and had ≥70% wear time (n = 5). CGM-naïve youth (n = 6) and those with insufficient wear time (n = 4) had a 10-day blinded Dexcom G6 Pro CGM placed to gather baseline glycemic data after enrollment.
After screening, youth and caregivers participated in CGM education and were taught the basics of insulin pump therapy at the initial visit. Families returned 15–30 days later to complete HCL education and initiated the Tandem t:slim X2 insulin pump with Control-IQ technology the same day. Youth who did not have a compatible smart phone (n = 2) were provided a locked-down Android phone to allow for CGM, but not HCL, data sharing during the study period. Basal rates, insulin-to-carbohydrate ratios, and correction factors were determined at the discretion of the research team after consideration of total daily insulin dose, pubertal status, and body weight. Participants were encouraged to use the bolus calculator to deliver meal boluses; however, decisions about the use of fixed meal carbohydrate counts and sleep mode were at the discretion of the investigators.
The research team communicated with families by phone daily during the 1st week of HCL use, twice weekly in weeks 2–3, and once during week 4 as per standard protocol for all youth initiating insulin pump therapy at our center. Beyond 4 weeks, the research team had access to real-time CGM data, but did not monitor these data or recommend changes to insulin pump settings unless contacted by participants. Families returned for follow-up in-person visits 3 and 6 months after starting HCL, which took the place of usual clinic visits. The study team reviewed CGM and insulin pump data at each visit to provide recommendations for changes to HCL settings and/or behavioral guidance. During each visit, participants were asked about adverse events and device issues. The study team helped interested participants to complete the paperwork needed to obtain insurance coverage for the HCL system to support ongoing use after study completion.
Predetermined criteria for study withdrawal included investigator concern that continued intervention would be unsafe, two episodes of severe hypoglycemia, or two episodes of DKA.
Glycemic outcomes
The primary outcome measure was the absolute difference in CGM time in range (TIR) (70–180 mg/dL) at baseline and during 6 months of HCL use. Secondary outcomes included change in HbA1c, episodes of severe hypoglycemia or DKA, mean CGM sensor glucose, coefficient of variation, percent time below range (<54, <70 mg/dL), percent time above range (>180, >250, >300 mg/dL), and insulin pump metrics (total daily insulin dose, total daily basal and bolus insulin, time in auto mode, user vs. Control-IQ-initiated boluses).
Person-reported outcome measures
PROMs were administered to youth ≥8 years and their primary diabetes caregiver at baseline, 3 months, and 6 months. Type 1 Diabetes and Life (T1DAL) uses a 5-point Likert scale to assess diabetes-specific health-related quality of life; scores range from 0 to 100 with higher scores reflecting greater quality of life. 11 Emotional distress related to diabetes was evaluated using problem areas in diabetes (PAID). 12,13 To account for different numbers of items in the age-specific versions of the PAID survey, scores were scaled from 0 to 100 with higher scores reflecting greater distress. 14,15 Insulin delivery Systems: Perceptions, Ideas, Reflections, and Expectations (INSPIRE) assesses positive expectancy of HCL systems; 16 scores range from 0 to 100 and higher scores reflect greater positive expectancy. Diabetes self-management behaviors were documented using the Diabetes Management Questionnaire (DMQ). DMQ scores range from 0 to 100 with higher scores reflecting greater engagement with diabetes care. 17
Statistical analyses
Study data were collected and managed using REDCap electronic data capture tools hosted at Children's National Hospital. To account for the small sample size, results are presented as medians and interquartile ranges (IQRs; 25th, 75th percentiles). Analyses were performed on a per protocol data set that captured all available CGM and insulin pump data from the t:slim X2 insulin pump during the intervention period. After graphical inspection of the data, multilevel mixed-effects regression was used to assess changes in CGM metrics, HbA1c, insulin requirements, and PROMs. Poisson regression with robust errors was used to contrast incidence rates. All P-values were considered significant at a two-sided level of 0.05. Pairwise correlations were used to assess the relationship between baseline HbA1c and youth and caregiver PROMs. Analyses were performed using STATA 17.0 (StataCorp, College Station, TX, USA) and the NumPy and SciPy modules in Python.
Results
Participant characteristics
Demographic characteristics of participants are reported in Table 1. One participant did not have baseline CGM data and could not be included in CGM analyses but is represented in all other data. Thirteen participants (86.7%) completed the 6-month study period. Study participation was discontinued in two participants: one participant on day 17 of HCL use due to protocol nonadherence and refusal to wear the HCL system and another on HCL day 142 after two episodes of DKA during a major depressive episode. All youth who completed the intervention opted to continue using t:slim X2 insulin pump with Control-IQ technology after completion of the study.
Demographic Characteristics of Participants
Note: Calculated values reported as median (IQR). Two participants were >18 years of age and did not have a parent participant.
CGM, continuous glucose monitor; DKA, diabetic ketoacidosis; IQR, interquartile range.
System usage
Median sensor use during the study period was 82.4% (71.0, 92.8%), whereas median time in HCL was 78.3% (59.7, 87.3%). Of the median 10.1 (9.2, 11.9) total daily boluses per day, 71.7% (63.8, 79.3%) were HCL-initiated autoboluses, whereas only 28.3% (20.7, 36.2%) were user initiated. Median total daily insulin dose decreased nonsignificantly from a self-reported baseline dose of 1.21 U/(kg·day) [0.94, 1.38 U/(kg·day)] on injection therapy to 1.07 U/(kg·day) [0.98, 1.34 U/(kg·day)] during the study period (P = 0.27).
Glycemic outcomes
Baseline TIR of 12.3% (3.0 h/day) improved by 23.7%-points (5.7 h/day) (P < 0.001) (Table 2; Fig. 1). Although no individual achieved >70% TIR, 100% had a ≥5% improvement in TIR, 92.9% had a ≥10% improvement, and 64.3% had a ≥20% improvement. Time above range >180 mg/dL decreased by 23.9%-points (5.7 h/day) (P < 0.001) from a baseline of 86.5%. Time above range >250 mg/dL decreased by 33.9%-points (8.1 h/day) (P < 0.001) and time >300 mg/dL decreased by 33.5%-points (8.0 h/day) (P < 0.001). Time below range <54 mg/dL and <70 mg/dL were low at baseline and did not increase during the study period. No individual participant had >4% time <70 mg/dL or >1% below 54 mg/dL. The coefficient of variation increased from 30.3% (22.1, 33.4%) to 39.0% (35.6, 40.9%) (P < 0.001).
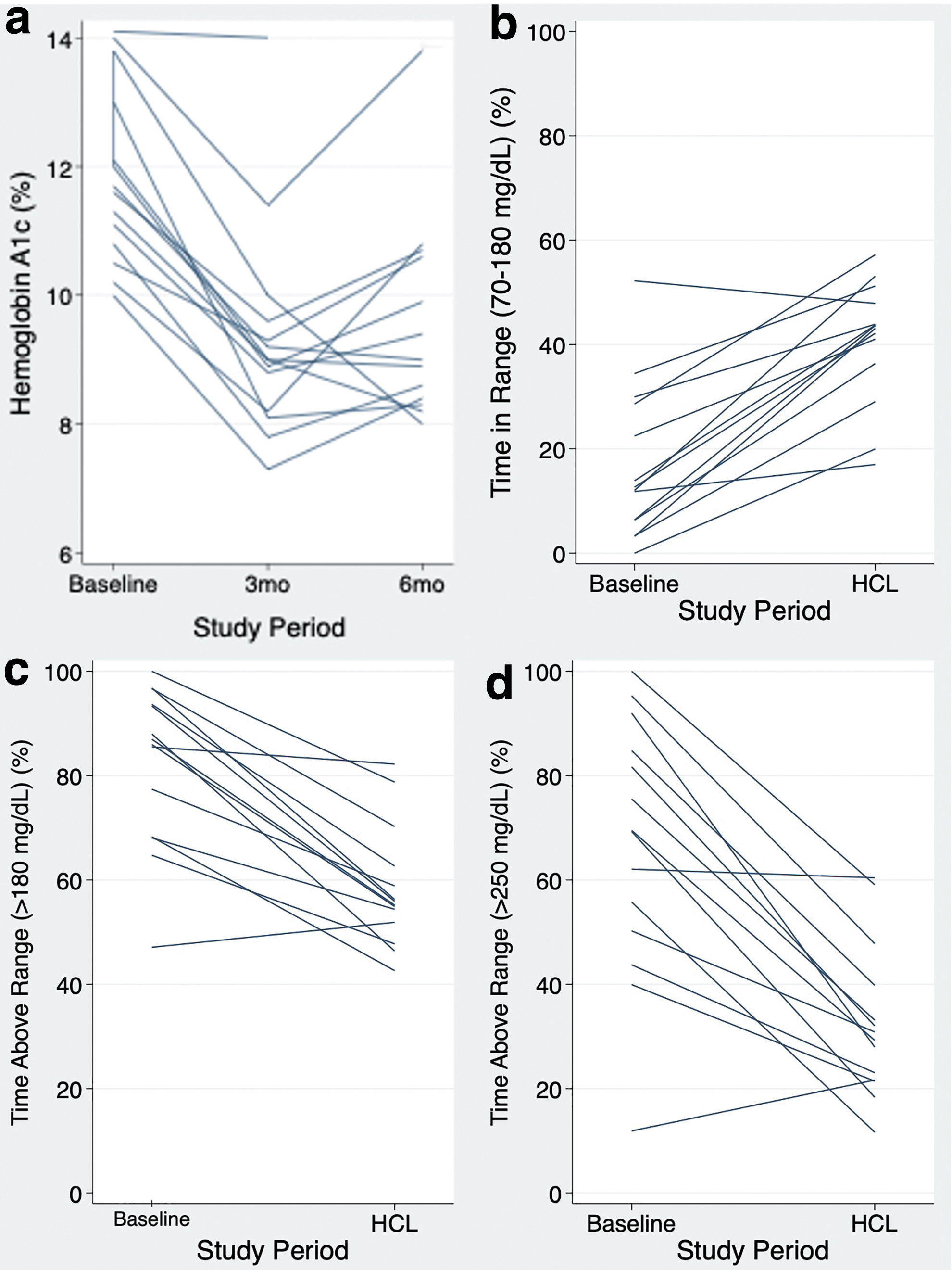
Spaghetti plots of individual data at baseline and during the intervention: HbA1c (%)
Changes in Glycemic Control and Youth and Parent Person-Reported Outcome Measures During the 6-Month Intervention
Note: Values for each timepoint reported as median (IQR).
Change reported as coefficient and 95% CI for multilevel mixed-effects regression analyses.
P-values reported reflect differences between baseline and the 90-day study period unless otherwise noted.
CI, confidence interval; DMQ, Diabetes Management Questionnaire; HbA1c, hemoglobin A1c; HCL, hybrid closed loop; INSPIRE, insulin delivery systems: perceptions, ideas, reflections, and expectations; PAID, problem areas in diabetes; T1DAL, Type 1 Diabetes and Life.
Glycemic outcomes were calculated separately for the daytime (06:00 to 24:00) and nighttime periods (24:00 to 06:00) (Table 3). Daytime TIR increased by 22.1%-points (P < 0.001) and nighttime by 28.5%-points (P < 0.001) (Fig. 2). Improvements in overnight TIR were greater than daytime improvements (P = 0.02). Greater than 20%-point decreases in time above range >180, >250, and >300 mg/dL were noted during the daytime and the nighttime (all P-values <0.001).
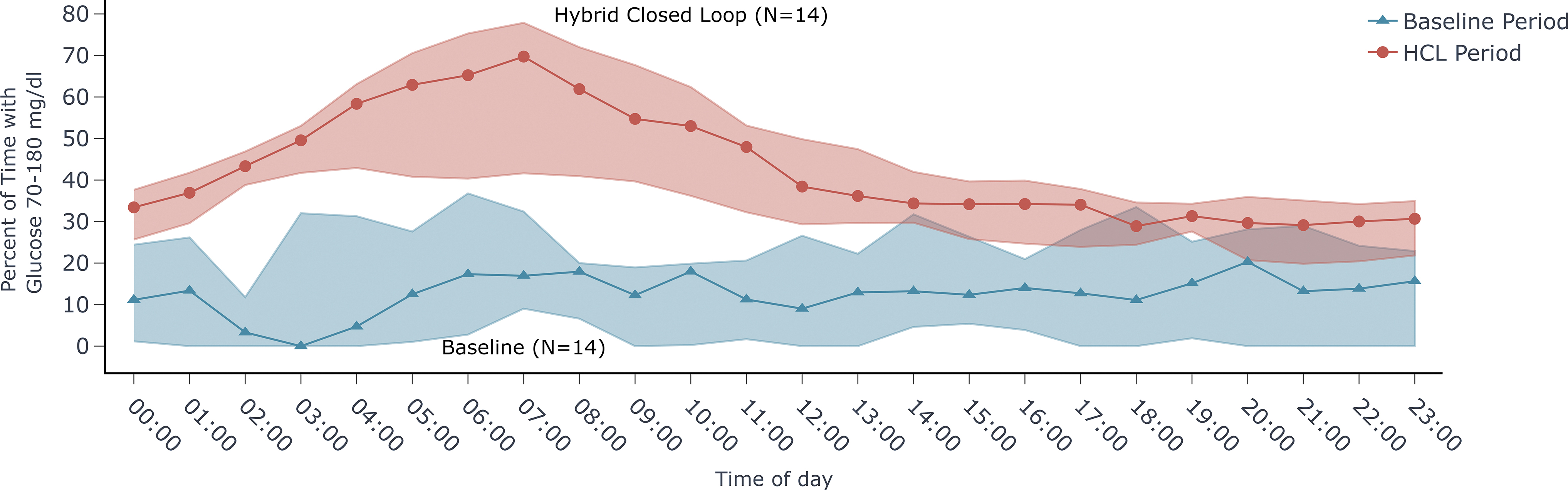
Envelope plot of hourly median time in range and baseline and during the HCL intervention period.
Glycemic Outcomes By Time of Day, Including Daytime (06:00 to 24:00) and Nighttime (24:00 to 06:00)
Note: Values for each timepoint reported as median (IQR).
Change reported as coefficient and 95% CI for multilevel mixed-effects regression analyses.
HbA1c decreased by 2.5%-points (95% confidence interval [CI] −3.1% to −2.0%; P < 0.001) from baseline (11.7%, IQR 10.8, 13.0%) to 3 months (9.0%, IQR 8.2, 9.6%). HbA1c improvements were maintained at 6 months (9.0%, IQR 8.4, 10.6%) with an overall decrease of 2.1%-points (95% CI −3.1 to −1.1; P < 0.001) from baseline; HbA1c did not change from 3 to 6 months (β = 0.5%, 95% CI −0.18% to 1.22%, P = 0.14).
DKA and severe hypoglycemia
In the 6 months before enrollment, five participants each experienced one episode of DKA (67 episodes per 100-person years). One participant experienced an episode of DKA after enrolling in the study, but before starting HCL. During the intervention period, 5 episodes of DKA occurred (3 participants each experienced 1 episode of DKA and 1 participant had 2 episodes; 72 episodes per 100-person years). After accounting for correlations in the paired data using a Poisson regression model with robust errors, rates of DKA did not increase during the study period (P = 0.78). Three of the four youth (75%) who had an episode of DKA during the intervention also had an episode in the 6 months before enrollment. No severe hypoglycemia occurred in the 6 months before enrollment or during the study period.
Person-reported outcomes measures
PROM data are presented in Table 2. Parent T1DAL scores reflecting diabetes-specific quality of life increased from baseline to 3 months (P = 0.002) and remained stable at 6 months (P < 0.001). Youth T1DAL scores increased from baseline to 3 months (P = 0.04) and baseline to 6 months (P = 0.004). Diabetes distress among parents, as captured by PAID scores, was high at baseline and decreased at 3 months (P < 0.001) and at 6 months (P < 0.001). Baseline youth PAID scores decreased at 3 months (P = 0.006) and 6 months (P = 0.005).
Baseline INSPIRE scores were equally high among youth and parents (P = 0.23). Positive expectancy of HCL did not change throughout the study among parents (3 months, P = 0.40; 6 months, P = 0.11) or youth (3 months, P = 0.29; 6 months, P = 0.76). Parent DMQ scores, reflecting diabetes self-management behaviors, increased at 3 months (P < 0.001), but were unchanged from baseline at 6 months (P = 0.20). A similar pattern was observed for youth DMQ scores, which increased at 3 months (P = 0.02) but were unchanged from baseline at 6 months (P = 0.08).
The relationship between baseline PROMs and changes in glycemia
Improvements in HbA1c from baseline to 6 months did not correlate with any baseline parent PROMs. Changes in HbA1c were not correlated with any baseline youth PROMs. Changes in HbA1c from baseline to 6 months were positively correlated with changes in parent INSPIRE scores from baseline to 6 months (r = 0.77, P = 0.006) and changes in parent DMQ scores from baseline to 6 months (r = 0.75, P = 0.008), but did not correlate with changes in parent T1DAL scores (r = −0.16, P = 0.68) or parent PAID scores (r = −0.21, P = 0.56). Changes in HbA1c did not correlate with changes in any youth PROMs.
Discussion
Among this cohort of publicly insured NHB youth with suboptimal glycemic control, TIR increased by 5.7 h per day, time in significant hyperglycemia (>250 mg/dL) decreased by 8.1 h per day, and diabetes-related quality of life improved in youth and parents without any increase in rates of DKA during 6 months of HCL use. To our knowledge, this pilot study is the first to examine the effects of HCL use specifically in a population of historically minoritized American youth with suboptimal glycemic control. Use of diabetes technologies improves glycemic control; however, increases in use over the past decade have highlighted inequities among youth of color and those of lower socioeconomic statuses. 2 Further data from studies specifically examining the safety and efficacy of HCL use in historically minoritized youth are needed to address inequities and to bridge the gaps in type 1 diabetes care and outcomes.
Our cohort of youth differs from those in previous HCL pivotal trials with respect to race, insurance, socioeconomic status, and glycemic control. We intentionally enrolled 100% NHB, publicly insured youth with HbA1c ≥10% to study the effects of HCL use in those who have been historically least likely to access these systems. According to the U.S.-based T1D Exchange registry, the type 1 diabetes population comprises 55% privately insured individuals, 73.5% NHW individuals, and 7.5% NHB individuals. 5 However, recent U.S.-based pivotal trials of HCL systems have failed to accurately represent this population, enrolling ≥90% privately insured participants, >60% from households with median income ≥$100,000, >80% with college degrees, and <4% NHB participants. 14,18,19 Notably, the recent Bionic Pancreas pivotal trial included a more racially diverse population with a greater range of baseline HbA1c values. 9,20 Youth enrolled in prior pivotal trials of HCL systems had a baseline TIR of 47%–53% and HbA1c of 7.6%–8.1%, 9,14,19 which stands in stark contrast with the most recent nationwide data demonstrating a median HbA1c of 9.3% among adolescents with only 17% of youth attaining the HbA1c target of <7%. 21 These nonrepresentative populations experienced TIR improvements between 10%–15%-points and HbA1c improvements of <0.8%-points 9,14,19 as compared with 23.7%-points improvement in TIR and 2.1%-points improvement in HbA1c in our study. Our findings align with prior data demonstrating the most substantial glycemic improvements among individuals with poorest baseline glycemic control 8 –10,22,23 despite previous studies failing to include those with the magnitude of hyperglycemia seen in our cohort.
Two international studies have set out to assess the impact of HCL on insulin pump-naïve youth with suboptimal glycemic control, although none have enrolled youth with the degree of hyperglycemia found in our cohort. 24,25 One enrolled youth had a baseline HbA1c of 10.5% and TIR of 27.6%, whereas the second cohort had a baseline HbA1c of 8.6% and TIR of 42.1%. These studies were conducted outside of the United States in health care systems different from our own in which ethnicity and measures of socioeconomic status may not be comparable. These two studies showed improvements in TIR (36%–39%-points) and HbA1c (2.1%–2.9%-points) comparable with our findings. Data from the Diabetes Control and Complications Trial (DCCT) showed an exponential relationship between the highest HbA1c values and microvascular complications. Although our participants did not achieve internationally accepted glycemic targets, the improvements in glycemia in these youth with the highest HbA1c values may carry greater clinical significance in reducing the risk for long-term microvascular complications than improving glycemia in those with lower HbA1c values. 26,27 Although mean glucose improved, glucose variability, which has been suggested to predict worse outcomes, 28 increased likely because patients were previously experiencing sustained hyperglycemia with little variability. Insulin doses decreased slightly though not significantly raising the possibility that baseline self-reported insulin doses were inflated. Glycemic improvements occurred despite limited user engagement with the HCL system, as evidenced by only 28% of boluses being user initiated. Notably, time in closed loop was ∼15% lower than in pivotal studies of HCL due to low active sensor time. 19,29 These findings suggests that additional supports, education, and strategies to promote sustained engagement with HCL may be helpful for increasing time in HCL and glycemic improvements.
Healthcare professionals are gatekeepers in access to technology. Their attitudes, biases, and use of subjective criteria to determine who is prescribed technology may result in inequitable distribution of these devices. 30,31 Positive expectancy of HCL in this historically marginalized cohort is no different from the groups in which HCL is more commonly used, 15 suggesting that clinician biases rather than differences in patient perceptions of HCL contribute to inequities in rates of HCL use. 30,31 All participants chose to continue HCL use upon study completion, demonstrating that use of the HCL system is acceptable to this population. The theoretical concern for DKA due to the potential for unrecognized pump site failure has been cited as a reason to withhold HCL therapy from youth with suboptimal glycemia. Although large-scale population data have in fact shown lower rates of DKA among insulin pump users, the inequities in real-world insulin pump use mean that youth of lower socioeconomic statuses and those with suboptimal glycemic control are likely under-represented. 32 As compared with large scale European population studies in which the incidence of DKA was 3.72 events per 100 person-years, 32 baseline rates of DKA in our cohort were markedly higher at 67 per 100 person-years. We found no change in the incidence of DKA in our cohort. These data demonstrating the safety and acceptability of HCL use have the potential to dispel provider misconceptions and increase equitable HCL prescribing practices among clinicians.
Previous studies of the psychosocial aspects of HCL use among predominantly NHW youth with better glycemic control (baseline HbA1c 7.7%–8.8%) have yielded inconsistent findings about changes in diabetes-specific quality of life and emotional distress. 33 Diabetes-related quality of life increased and diabetes distress decreased among parents and youth in our study, whereas positive expectancy of HCL was high at baseline and remained unchanged throughout the study period. At baseline, diabetes distress and diabetes-specific quality-of-life scores in our cohort were worse than in previously studied cohorts of youth using HCL systems. 34 –36 Two of these studies failed to show improvements in diabetes-related quality of life and diabetes distress, whereas one showed improvement in health-related quality of life with no change in diabetes distress. 34,35 Although the above-mentioned studies examined changes in PROMs among a cohort experienced with insulin pump use, few studies have specifically studied these changes in youth transitioning from multiple daily injections (MDIs) to insulin pump therapy. In a cohort of youth with mean baseline HbA1c <8% transitioning from MDI to insulin pump therapy, in whom racial and ethnic identities were not reported, overall caregiver burden decreased and diabetes-specific health-related quality of life improved in children 8–11 years but not in adolescents 12–16 years. 37 Despite a small sample size, we identified clear psychosocial benefits indicating that enrolling historically minoritized patients with suboptimal baseline glycemic control in HCL studies may identify previously unrecognized benefits of this technology. In addition, improvements in PROMs did not correlate with baseline glycemic control nor improvements in glycemia during our study, suggesting that glycemic measures may not be the most appropriate way to determine whether an individual is an appropriate candidate for HCL. With evidence demonstrating that diabetes distress is associated with suboptimal glycemic control and reduced self-care 38 and an inability to predict which individuals will benefit most from HCL use, these findings also support the need for improved HCL access for all youth with type 1 diabetes.
Limitations to our study include the small sample size and single-arm design for this pilot study. Our findings reflect improvements with the use of a single HCL system; additional studies using other HCL systems are needed to determine whether one system is more beneficial for historically minoritized youth with suboptimal glycemic control. Despite these limitations, significant improvements in glycemic control and quality of life in this cohort speak of the magnitude of the effect sizes in our study. Although our HCL training protocol and communications with families after HCL initiation mirrored clinical care at our institution, participants had ready access to the study team and were provided with the HCL system and pump and CGM supplies by the study team, thereby eliminating some of the challenges of navigating the American health care system. As in routine clinical care, fewer study team check-ins occurred between the 3- and 6-month follow-up visits that may have contributed to the decline in glycemic improvement and increases in DKA during this period. Although this study was intentionally modeled after real-world practices of pump initiation in our institution, providing additional touchpoints or incorporating a patient navigator or community health worker in the clinic to support this population of patients in the use of technology between appointments should be considered to further improve glycemic outcomes and decrease the risks of HCL use. The incidence of DKA was assessed and no differences were found; however, our sample size only provided 8.4% power to detect a significant difference. A sample size of 3675 would be needed to provide 80% power to assess for differences in the rates of DKA. Despite these limitations, this study was purposefully designed to address misconceptions about risks and benefits of HCL use that likely contribute to inequities in diabetes technology use and glycemic control among youth with type 1 diabetes. Youth represented in our study cohort have historically been under-represented in research, 7 have disproportionately poor glycemic control, and have increased rates of complications as compared with the privately insured predominantly NHW participants who are typically enrolled in clinical trials. 2,4,21,26,39,40
The inclusion of PROMs in addition to changes in glycemia also allows for a more comprehensive understanding of the benefits of HCL use in this population. Larger research studies and more real-world data from this historically minoritized group of youth with T1D are needed.
Conclusions
Inequities in type 1 diabetes care and outcomes are well known. Targeted interventions, in both research and clinical care, are needed to close the gap and support equitable access to and sustained use of HCL technologies that provide the greatest benefit to those who are struggling the most with type 1 diabetes. We demonstrate that this population which historically has the worst health outcomes and has been historically under-represented in type 1 diabetes research can be successful with HCL therapy and may experience additional benefits as compared with more commonly studied populations in terms of glycemic control and PROMs. These data are an essential step in working toward equity in access to diabetes technology and health care outcomes for youth with type 1 diabetes.
Footnotes
Acknowledgments
The authors thank all the youth and their families who participated in the trial and acknowledge Sneha Thanasekaran and Alex Trahan from Tandem Diabetes Care for assistance with data analysis.
Authors' Contributions
B.E.M. contributed to conceptualization, methodology, formal analysis, investigation, data curation, writing–original draft, writing–review and editing, visualization, project administration, and funding acquisition. J.B.G. was involved in investigation, data curation, and writing–review and editing. S.M. carried out investigation and writing–review and editing. M.M. and R.S. carried out conceptualization, methodology, and writing–review and editing. A.P. contributed to investigation, data curation, writing–original draft, writing–review and editing, and project administration. B.E.M. is the guarantor of this study and, as such, had full access to the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Author Disclosure Statement
B.E.M. is supported by the National Institutes of Health (NIH; PI: K23DK129827) and has received investigator-initiated research support from Tandem Diabetes Care, Inc. (TDC20210226), and the Cystic Fibrosis Foundation, industry-sponsored research support from Medtronic, and research supplies from Dexcom, Inc. and Digostics. J.B.G. is supported by the American Diabetes Association (7–21-PDFHD-09) and has received research supplies from Dexcom. S.M. has received a speaker honorarium from Dexcom. M.M. is currently employed by the NIH; this study was conducted before her employment at NIH. A.P. has received investigator-initiated research support from Tandem Diabetes Care, Inc. (TDC20210226), and research supplies from Dexcom. The other authors have no conflicts of interest to disclose.
Funding Information
Funding and product were provided by Tandem Diabetes Care (TDC20210226). Product support was also provided by Dexcom (AP-2020-020).