
Abstract
Background:
Postmeal hyperglycemia is difficult to avoid even with automated insulin delivery (AID) due to the delayed effect of subcutaneously administered rapid-acting insulin analogs. Inhaled technosphere insulin (TI, Afrezza®) has a more rapid onset of action with the potential to reduce the postmeal glucose rise. We evaluated the effects of a regimen of TI and degludec over 30 weeks.
Methods:
In total, 123 adults with type 1 diabetes (T1D) participated in a 17-week multicenter randomized controlled trial comparing a regimen of TI plus insulin degludec versus usual care, which consisted predominantly of AID or multiple daily insulin injections (MDI). Interested participants in the TI-degludec group continued this regimen for an additional 13 weeks, with no scheduled visits prior to a final visit at 30 weeks to approximate real-world care.
Results:
Of the 62 participants in the TI-degludec group, 58 completed the 17-week visit and 45 continued into the extension phase. Prior to the study, 44% were using AID, 9% a sensor-augmented pump without automation, and 47% MDI. Mean HbA1c was 7.6% ± 1.0% at baseline, 7.6% ± 1.0% at 17 weeks, and 7.4% ± 1.0% at 30 weeks. Mean HbA1c change from 17 weeks to 30 weeks was −0.21% (95% confidence interval −0.33% to −0.09%, P < 0.001). HbA1c was <7.0% in 21% at baseline, 30% at 17 weeks, and 42% at 30 weeks. Mean time in range 70–180 mg/dL was 52% ± 18% at baseline, 53% ± 20% at 17 weeks, and 54% ± 20% at 30 weeks. Mean percent time <54 mg/dL was 0.4% ± 0.6%, 0.4% ± 0.8%, and 0.6% ± 1.0%, respectively. Mean total daily TI dose at 30 weeks was 53 ± 31 U/day, which was about twice the total daily rapid-acting insulin analog dose of 24 ± 12 U/day at baseline prior to switching to TI.
Conclusions:
HbA1c levels were sustained over 30 weeks using a TI-degludec regimen after switching from AID or MDI. TI should be considered an option for people with T1D.
Introduction
Postmeal hyperglycemia is difficult to avoid even with automated insulin delivery (AID) systems due to the delay in effect of subcutaneously administered rapid-acting insulin analogs (RAA). Inhaled technosphere insulin (TI, Afrezza®,
In a 17-week randomized controlled trial (RCT) in 123 adults with type 1 diabetes (T1D) conducted at 19 U.S. sites, we reported that change in HbA1c was noninferior with a regimen of TI plus a basal insulin (degludec) versus a control group that continued their usual insulin delivery method consisting of either AID, a sensor-augmented pump (SAP) without automation, or multiple daily insulin injections (MDI). 6 With the TI-degludec regimen, almost twice as many participants achieved an HbA1c level <7.0% compared with usual care, and four times more participants improved HbA1c by >0.5%. However, a comparable number of participants had worsening of HbA1c by >0.5%. On completion of the 17-week RCT, participants had the opportunity to enter an extension phase and continue use of the TI-degludec regimen for an additional 13 weeks.
The objective of this article was to assess whether the glycemic outcomes using TI-degludec for 17 weeks would be sustained over an additional 13 weeks without any intervening study visits to approximate real-world care.
Methods
The protocol was approved by a central institutional review board and informed consent was obtained from each participant. The RCT protocol has been described previously 6 and is summarized below and on clinicaltrials.gov (NCT05904743).
Participants were ≥18 years old with T1D for at least 6 months using AID, nonautomated pump, or MDI for insulin delivery and continuous glucose monitoring (CGM) for glucose monitoring. After the collection of baseline CGM data with a blinded Dexcom G6 Pro sensor, participants were randomly assigned (1:1) to either the TI-degludec regimen or the usual care group. Participants assigned to the TI-degludec group discontinued their prestudy insulin delivery method (AID, SAP, or MDI) and initiated the use of degludec injected once daily and TI for meal bolusing and corrections.
During the first 4 weeks, the TI and degludec doses were titrated and subsequently adjusted as indicated. Participants were instructed to administer a correction dose of TI as soon as 60–90 min after a previous TI dose if the glucose level was >140 mg/dL, including at bedtime, and if the glucose level was >200 mg/dL overnight. At the 17-week visit, participants were offered the opportunity to continue use of the TI-degludec regimen in an extension phase for an additional 13 weeks.
In-clinic visits occurred at baseline (randomization), 17 weeks, and 30 weeks, and virtual visits occurred after 4, 8, 15, 22, 29, 56, and 91 days. At baseline, 17 weeks, and 30 weeks, the following were obtained: HbA1c was measured at a central laboratory, forced expiratory volume in 1 s (FEV1) was assessed using the Vitalograph asma-1™ respiratory monitor, CGM data analysis were collected using a blinded Dexcom G6 Pro sensor, and patient-reported outcome (PRO) surveys (diabetes distress scale, hypoglycemia confidence scale, freedom and flexibility questionnaire, and insulin treatment satisfaction questionnaire) were conducted.
At baseline following randomization and at 17 weeks, a meal challenge was performed using TI for the meal bolus, according to procedures previously published. 4 For the baseline meal challenge, the participant’s TI dose was based on their usual RAA bolus for the 37 g of carbohydrate in the BOOST® nutritional shake, which was consumed (doubling of RAA dose and then rounded down to the nearest 4-unit TI dose); participants using an AID system or nonautomated pump prior to the study continued its use during the baseline challenge. For the 17-week challenge, the TI dose was based on the typical TI dose for the amount of carbohydrate that had been optimized for the participant over the 17 weeks of the trial.
Study endpoints included HbA1c and CGM metrics. Means are presented with standard deviations and medians with interquartile ranges. Baseline CGM metrics (using blinded G6 Pro) were computed, while participants were using their prestudy insulin delivery method (AID, MDI, or nonautomated pump). Statistical comparisons were made between baseline and 30 weeks and between 17 weeks and 30 weeks. Continuous endpoints were analyzed using paired t tests and binary endpoints were analyzed using McNemar’s tests. Only participants completing the extension phase were included in the efficacy analyses; all participants were included in the safety analyses. The false discovery rate was controlled using the adaptive Benjamini–Hochberg procedure.
Results
Of the 62 participants randomly assigned to the TI group, 58 completed the 17-week visit and 45 continued into the extension phase. The mean age of the 45 participants was 47 ± 15 years; 53% were female, 87% were of White race, and 11% were of Hispanic ethnicity. Prior to the study, 44% of the 45 participants were using AID, 9% were using SAP, and 47% were using MDI.
Of the 13 participants completing the 17-week visit who did not continue into the extension phase, 8 (62%) were AID users prior to the study. A 17-week HbA1c measurement was missing for one of the 13 participants. For the other 12 participants, the mean HbA1c was 7.4% ± 0.8% at baseline and 7.7% ± 1.4% at 17 weeks (at the end of RCT); 2 (17%) had an HbA1c improvement >0.5% at 17 weeks, and 4 (33%) had a worsening of >0.5%. This compares with 10 (22%) improving and 11 (24%) worsening HbA1c >0.5% among the 45 who initiated the extension phase.
Glycemic outcomes
The 30-week visit was completed by 43 (96%) of the 45 participants who initiated the extension phase. Among the 43, the mean HbA1c was 7.6% ± 1.0% at baseline, 7.6% ± 1.0% at 17 weeks, and 7.4% ± 1.0% at 30 weeks. The mean change in HbA1c from 17 weeks to 30 weeks was −0.21% (95% confidence interval [CI] −0.33% to −0.09%, P < 0.001; Table 1). Between 17 weeks and 30 weeks, 6 (14%) participants improved HbA1c >0.5% and 1 (2%) worsened >0.5%. The HbA1c level was <7.0% in 21% at baseline, 30% at 17 weeks, and 42% at 30 weeks. A slight reduction in HbA1c between 17 weeks and 30 weeks was seen in each subgroup based on baseline HbA1c (<7.0%, 7.0%–7.9%, 8.0%–8.9%, ≥9.0%; Fig. 1).
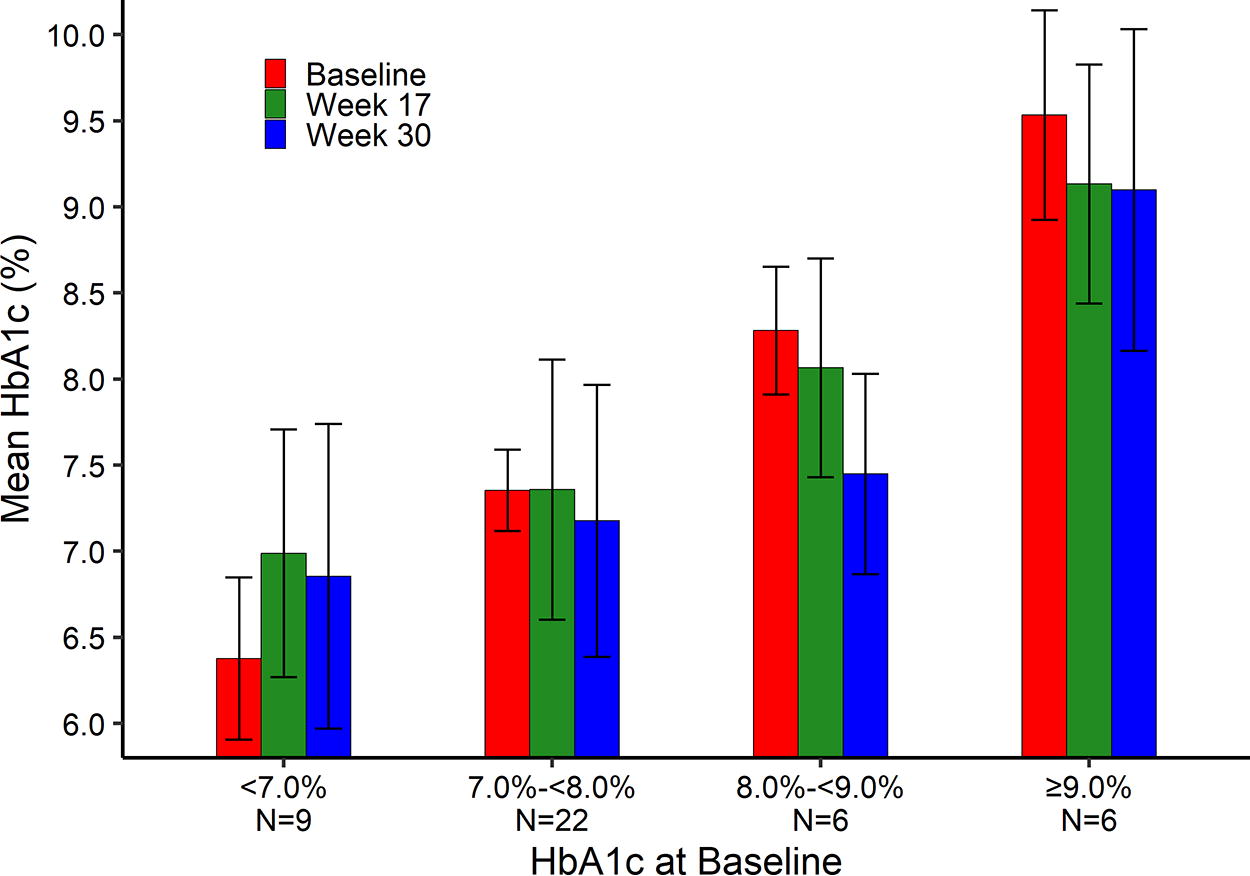
Change in HbA1c over time within subgroups of baseline HbA1c. The bars represent the mean HbA1c within each subgroup and the error bars show the mean ± 1 standard deviation.
HbA1c and Continuous Glucose Monitoring Endpoints
CGM, continuous glucose monitoring; CI, confidence interval; SD, standard deviation.
Mean change, 95% CI, and P value estimated using a paired t test.
Mean and standard deviation estimated using maximum likelihood. A generalized linear mixed effects regression model with the t-distribution for the error terms was used to estimate the mean change, 95% CI, and P value.
CGM-measured prolonged hyperglycemic events are defined as ≥90 cumulative minutes with CGM glucose >250 mg/dL within a 120-min period without ≥15 consecutive minutes ≤180 mg/dL. The prolonged hyperglycemic event ends after the CGM glucose is ≤180 mg/dL for ≥15 consecutive minutes.
CGM-measured hypoglycemic events are defined as ≥15 consecutive minutes with a CGM glucose <54 mg/dL. The hypoglycemic event ends after the CGM glucose is ≥70 mg/dL for ≥15 consecutive minutes.
The mean percent time in range 70–180 mg/dL (TIR) was 52% ± 18% at baseline, 53% ± 20% at 17 weeks, and 54% ± 20% at 30 weeks. The mean percent time >180 mg/dL was 46% ± 19%, 45% ± 22%, and 44% ± 22% and the mean percent time <54 mg/dL was 0.4% ± 0.6%, 0.4% ± 0.8%, and 0.6% ± 1.0% at the three time points, respectively. Figure 2 compares mean glucose by hour at baseline, at 17 weeks, and at 30 weeks and shows that mean glucose was lower overnight at baseline (using the prestudy insulin delivery method) compared with the TI-degludec regimen at 17 weeks or 30 weeks but lower during the day with TI-degludec.
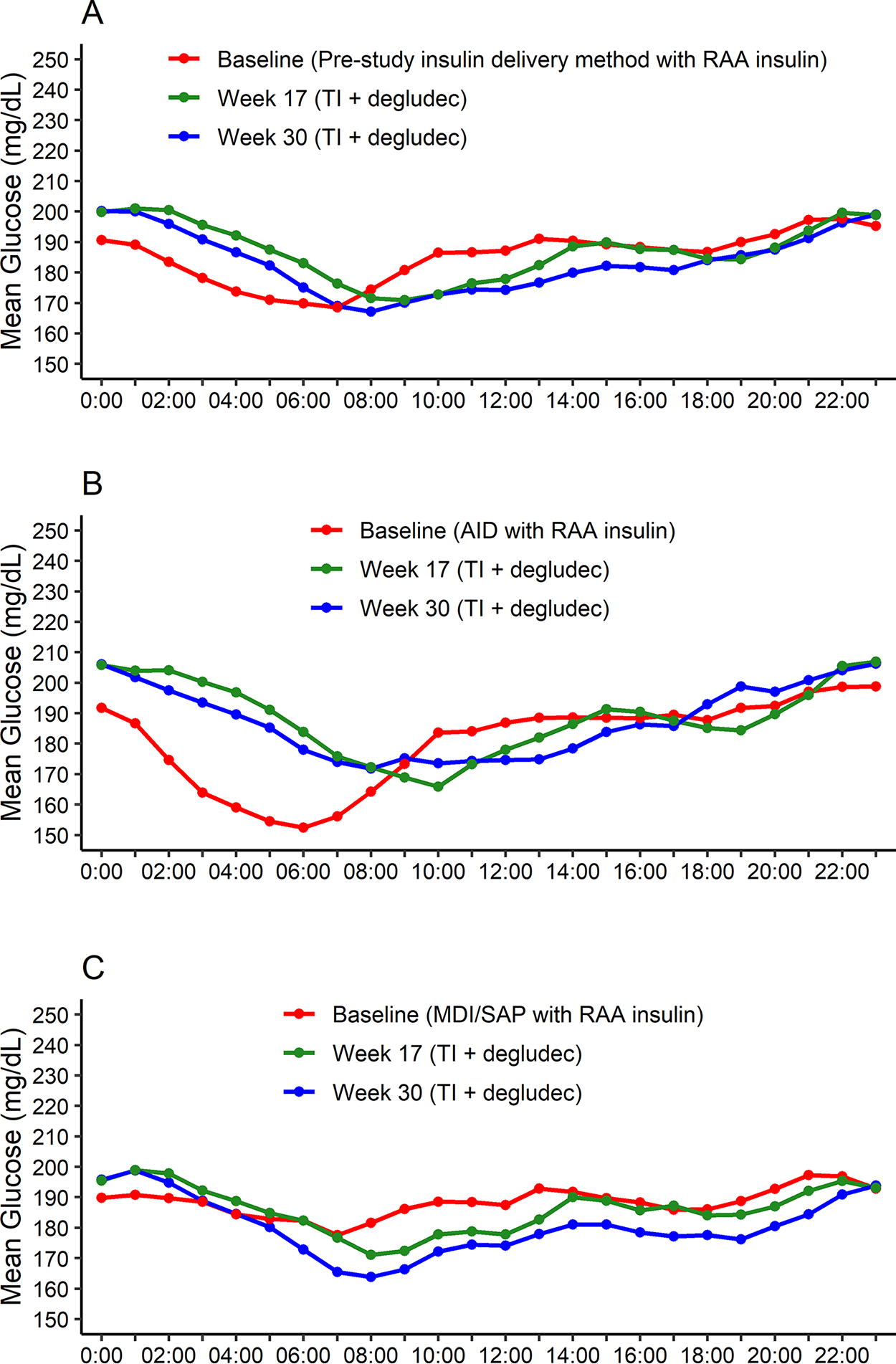
Mean glucose by hour of the day. The points represent the mean CGM glucose at each hour of the day. Means are shown separately at baseline (red), 17 weeks (green), and 30 weeks (blue). A: Overall. B: Prestudy AID users. C: Prestudy MDI/SAP users. AID, automated insulin delivery; CGM, continuous glucose monitoring; MDI, multiple daily insulin injections; SAP, sensor-augmented pump.
Table 2 shows the glycemic outcomes separately for prestudy AID users and MDI/SAP users. Among the 18 prestudy AID users, the mean change in HbA1c 30 weeks after switching to TI-degludec was 0.08 (95% CI −0.33 to 0.50, P = 0.63), and the mean change in TIR was −5.6% (95% CI −19.4% to 8.2%, P = 0.62). In contrast, among 25 MDI/SAP users, the mean change in HbA1c was −0.35 (95% CI −0.71 to 0.01, P = 0.06) and the mean change in TIR was +6.5% (95% CI −4.3% to 17.2%, P = 0.34). When assessing mean glucose levels over 24 h, it can be seen in Figure 2 that overnight mean glucose increased in participants who switched from AID to TI-degludec, whereas during the daytime, glucose levels with TI-degludec were similar to AID. In the prestudy MDI/SAP users, comparing TI-degludec at 30 weeks with MDI/SAP at baseline, glucose levels appeared similar overnight and slightly better with TI-degludec during the daytime.
HbA1c and Continuous Glucose Monitoring Endpoints According to Baseline Insulin Delivery Method
AID, automated insulin delivery; CGM, continuous glucose monitor; CI, confidence interval; MDI, multiple daily insulin injections; SAP, sensor-augmented pump; SD, standard deviation.
Mean change, 95% CI, and P value estimated using a paired t test.
Mean and standard deviation estimated using maximum likelihood. A generalized linear mixed effects regression model with the t-distribution for the error terms was used to estimate the mean change, 95% CI, and P value.
CGM-measured prolonged hyperglycemic events are defined as ≥90 cumulative minutes with CGM glucose >250 mg/dL within a 120-min period without ≥15 consecutive minutes ≤180 mg/dL. The prolonged hyperglycemic event ends after the CGM glucose is ≤180 mg/dL for ≥15 consecutive minutes.
CGM-measured hypoglycemic events are defined as ≥15 consecutive minutes with a CGM glucose <54 mg/dL. The hypoglycemic event ends after the CGM glucose is ≥70 mg/dL for ≥15 consecutive minutes.
Safety
During the 13-week extension phase, there were no severe hypoglycemia or diabetic ketoacidosis events. One participant reported cough related to TI inhalation that had not been previously reported. FEV1 measurements were available for 44 of the 45 participants in the extension phase. The mean FEV1 measurements were 3.0 ± 0.8 L at baseline, 2.9 ± 0.8 L at 17 weeks, and 3.0 ± 0.8 L at 30 weeks. No participants had an FEV1 reduction ≥20%.
Insulin dose
The mean daily dose of degludec was 24 ± 13 U/day at week 17 and 24 ± 15 U/day at week 30, whereas the mean total daily dose of TI was 47 ± 30 U/day at week 17 and 53 ± 31 U/day at week 30. The 53 U/day TI dose at 30 weeks was about twice the total daily RAA dose of 24 ± 12 U/day at baseline prior to switching to TI. The mean bolus:basal insulin ratio was 64%/36% at 17 weeks and 68%/32% at 30 weeks.
Meal challenges
For the 49 participants who completed both the RCT baseline and the 17-week meal challenges, the TI to prestudy RAA ratio was 1.8 for the baseline meal challenge and had increased to 2.8 for the 17-week challenge. The effect of the larger TI dose at 17 weeks can be seen in Figure 3, which shows a reduced postmeal glucose excursion at 17 weeks compared with baseline (when about half were using AID), although the difference in area under the curve 180 mg/dL was not significant (P = 0.20).
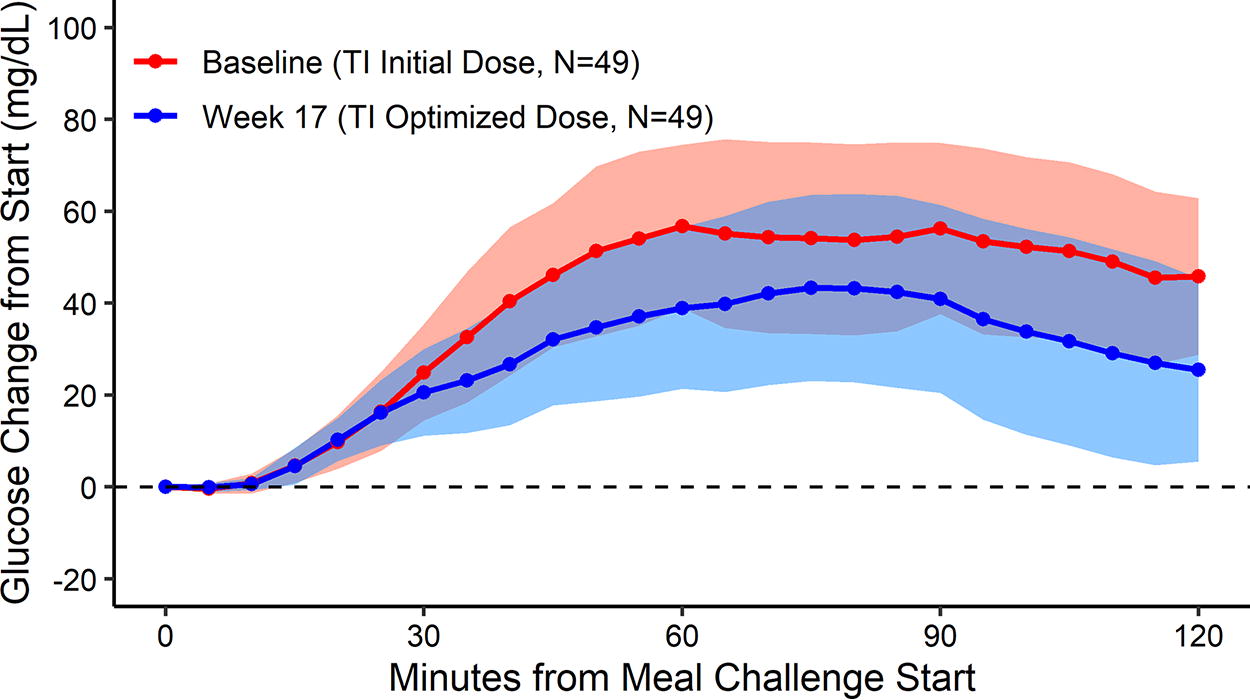
Glucose change from meal challenge start at baseline and 17 weeks. The points represent the mean CGM glucose at 5-min intervals following the start of the meal challenge (minute 0). The shaded bands represent the 95% confidence interval around the mean. Means and confidence intervals are shown separately at baseline (red) and week 17 (blue). CGM, continuous glucose monitoring.
Patient-reported outcomes
There were no significant differences comparing the PRO survey results at 30 weeks versus 17 weeks (Table 3). At the end of the trial, participants were asked whether they wanted to return to their prestudy insulin delivery method or continue to use the TI-degludec regimen. Overall, 44% of the 43 participants completing the extension phase expressed interest in continuing TI-degludec: 33% of 18 prestudy AID users, 50% of 4 prestudy nonautomated pump users, and 52% of 21 prestudy MDI users.
Patient-Reported Outcome Surveys
CI, confidence interval; SD, standard deviation.
Mean change, 95% CI, and P value estimated using a paired t test.
Discussion
In the INHALE-3 study, participants assigned to the TI-degludec group who continued using this regimen in an extension phase for an additional 13 weeks, mean HbA1c, which was unchanged from baseline at 17 weeks, showed a small but statistically significant reduction between 17 weeks and 30 weeks. This further reduction in HbA1c was associated with an increase in the total daily TI dose, suggesting that participants increased their TI dose as part of self-titration since there were no scheduled visits or contacts during the extension phase. There were no safety concerns identified during this extension phase.
The slight overall reduction in HbA1c between 17 weeks and 30 weeks was observed in both prestudy AID users and prestudy MDI/SAP users. During the daytime, glucose levels using TI-degludec appeared comparable with glucose levels at baseline using AID but overnight glycemic control appeared better with AID. In contrast, glucose levels were slightly lower during the day and similar overnight with TI-degludec compared with prestudy MDI.
The current U.S. labeling of TI, which followed the pivotal study conducted by Bode et al., 7 indicates that the starting initial dose should be 1.0–1.3 times the RAA dose for most of the dose range. However, this is based on the amount of powdered insulin in a cartridge and not on the amount that is actually absorbed across the lungs. The data from this study strongly support that an initial conversion of approximately 2:1 for bioequivalence, with a subsequent dose titration generally to a higher dose, is safe.
It was encouraging to see that not only were HbA1c levels sustained during the extension phase without scheduled visits for contacts but that there was an overall small improvement in HbA1c. Although we cannot ascertain the reason for this improvement, it is possible that participants became more comfortable with self-titration and perhaps dosed TI more frequently. The interpretation of these results has certain limitations. First, there was no concurrent control group, as the RCT control group was switched to TI-degludec for the extension phase. Second, not all participants elected to continue in the extension phase, which could be a source of bias.
Although we did not find significant changes in PRO survey results, 43% of participants expressed interest in continuing the TI-degludec regimen rather than returning to their prestudy regimen, even a third who were previously using AID. This finding and the results of the RCT and extension phase provide support for TI being an available option for people with T1D. Successful use of TI requires substantial engagement in diabetes self-management, including meal bolusing and potentially frequent correction dosing. If this is not done and meal boluses are frequently missed, glycemic levels may worsen, particularly when switching from an AID system. Thus, patient selection is important when prescribing TI. Future studies are needed to determine who is likely to be a good candidate for TI and who is not.
Footnotes
Authors’ Contributions
R.W.B. wrote the first draft of the article. All other authors provided critical review of the article, which was incorporated in the final version. P.C. and R.B. performed statistical analyses.
Author Disclosure Statement
R.W.B. reports no personal financial disclosures but reports that his institution has received funding on his behalf as follows: grant funding, study supplies, and consulting fees from Insulet, Tandem Diabetes Care, and Beta Bionics; grant funding and study supplies from Dexcom; grant funding from Abbott Diabetes Care, Bigfoot Biomedical, embecta, Sequel Med Tech, and MannKind; consulting fees and study supplies from Novo Nordisk; consulting fees from Vertex, Hagar, Ypsomed, Sanofi, and Zucara; and study supplies from Medtronic, Ascencia, Roche, and Eli Lilly. R.J.B. reports no financial disclosures. K.R.K. reports consulting fees from Novo Nordisk. K.R.K. has received research related contracts (paid to the institution) from Bayer, Boehringer-Ingelheim, Carmot, Diasome, Eli Lilly, Novo Nordisk, Rhythm Pharmaceuticals, and vTv Therapeutics. G.A. reports receiving consulting fees from Dexcom and Insulet and has received research support to her institution from Abbvie, Bayer, Fractyl Health, Insulet, Tandem Diabetes Care, and Welldoc. C.J.L. reports research support paid to her institution from Dexcom, Tandem Diabetes Care, Insulet, Novo Nordisk, and Abbott Diabetes and consulting fees from Dexcom and Tandem Diabetes Care. J.D. reports no disclosures. C.J. reports consulting, acting on an advisory board for and speaking on insulin pumps for Medtronic. C.M.L. reports receiving research support paid to her institution from Tandem Diabetes Care and Dexcom. P.C. reports no disclosures. K.J.R. reports no disclosures. I.B.H. reports consulting for Abbott Diabetes Care, Roche, Hagar, and Vertex and research support from MannKind, Dexcom, and Tandem Diabetes Care.
Funding Information
The trial was funded by MannKind, Inc. through a contract with the JAEB Center for Health Research, which then provided funding to the clinical sites.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.