
Abstract
Background and Aims:
Advanced hybrid closed-loop (AHCL) automated insulin delivery systems such as the MiniMed™ 780G have been shown to result in substantial improvements in disease management in people living with type 1 diabetes. The aim of the analysis was to assess the cost utility of the MiniMed 780G system compared with intermittently scanned continuous glucose monitoring (is-CGM) and multiple daily insulin injections (MDI) in people living with type 1 diabetes in France, to estimate the incremental cost-utility ratio (ICUR) and inform decision-making.
Methods:
The analysis was performed using the CORE Diabetes Model (version 9.5) and clinical input data were sourced from a randomized controlled trial, with glycated hemoglobin reductions of 1.54% (16.8 mmol/mol) and 0.2% (2.18 mmol/mol) assumed for the MiniMed 780G arm and is-CGM + MDI arm, respectively. The analysis was conducted from a national payer perspective over a 40-year time horizon; future costs and clinical outcomes were discounted at 2.5% per annum.
Results:
In the base case analysis, use of the MiniMed 780G system was associated with a mean gain in quality-adjusted life expectancy of 2.26 quality-adjusted life years (QALYs) compared with is-CGM + MDI (16.33 QALYs vs. 14.07 QALYs), while mean direct lifetime costs were EUR 78,509 higher (EUR 215,037 vs. EUR 136,528), resulting in an ICUR of EUR 34,732 per QALY gained. Findings from sensitivity analyses showed that analyses were robust to changes in assumptions in most input parameters.
Conclusions:
In people with type 1 diabetes in France not achieving glycemic target levels at baseline, the use of the MiniMed 780G system was projected to lead to substantial improvements in quality-adjusted life expectancy compared with continued use of is-CGM + MDI, with an ICUR of EUR 34,732 per QALY gained.
Introduction
In France, estimates relating to the number of people living with type 1 diabetes mellitus (T1DM) range from 196,000 to 260,000 people. 1,2 The clinical and economic burden associated with T1DM is substantial. Indeed, in France in 2022, health care expenditure for diabetes (including both type 1 and type 2 diabetes) totaled EUR 10.2 billion, which equates to EUR 2350 per person with diabetes. 3
The cornerstone of effective management of T1DM is regulation of glucose levels to minimize periods of hyper- and hypoglycemia. 4 The evolution of automated insulin delivery (AID) systems over the past decade, including enhancements to insulin dosing algorithms, has changed the landscape of management of T1DM, resulting in improved glycated hemoglobin (HbA1c) levels and reduced hypoglycemia compared with the use of multiple daily insulin injections (MDI) and fingerstick testing. 5 In France, health insurance covers care for people with T1DM (PWD), which includes complete coverage for diabetes-related medical expenses such as insulin pumps and continuous glucose monitors (CGM). 6
Adequate glycemic control in PWD reduces the risk of long-term complications, including both microvascular and macrovascular complications. For example, an increased risk of cardiovascular disease has been observed in PWD with a high HbA1c (∼10% [86 mmol/mol]) compared with lower HbA1c levels (∼8% [64 mmol/mol]). 7 Similarly, elevated HbA1c levels have also been linked with an increased risk for retinopathy and nephropathy. 8 The recent SAGE study demonstrated that, in Western Europe, only 23.9% (95% confidence interval [CI]: 21.4%–26.5%) of PWD achieved individualized HbA1c targets despite easy access to intermittently scanned continuous glucose monitoring (is-CGM), 9 highlighting the need for better disease management among a substantial percentage of PWD. In France specifically, social deprivation 10 and lack of human resources noted in some areas have been reported as being barriers to effective glucose control for some people, 11 supporting the need for better, and cost-effective, self-management of T1DM.
Modern AID systems such as the MiniMed™ 780G advanced hybrid closed-loop (AHCL) system (Medtronic Inc., Northridge, CA, USA) address many of the needs for improved diabetes management. A recent, investigator-initiated, multicenter, observational study in France showed that the MiniMed 780G resulted in statistically significant improvements in HbA1c and time-in-range (TIR) as well as a significant improvement in the percentage of people achieving a HbA1c target of <7%. 12 Furthermore, use of the MiniMed 780G has also been shown to improve patient-reported outcomes. 13 In addition, recent evidence from the ADAPT randomized controlled trial (RCT) showed that PWD using the MiniMed 780G had greater improvements in glucose control compared with those using is-CGM combined with MDI. 14
Since April 2022, the MiniMed 780G has been reimbursed for use in France for PWD aged at least 7 years and unable to achieve glycemic targets through continuous subcutaneous insulin infusion (also known as insulin pump therapy) with CGM/is-CGM for at least 6 months. Although AHCL AID systems have proven effective in managing T1DM, the costs of such systems can represent a barrier to uptake in some instances. A recent European cost-utility analysis showed the MiniMed 780G to be likely more cost-effective when compared with is-CGM combined with MDI for PWD not achieving glycemic targets. 15 To aid payers in France in continuing to make informed decisions on T1DM management, the objective of the current study was to evaluate the cost utility of the MiniMed 780G versus is-CGM combined with MDI in France.
Methods
Model structure
Version 9.5 of the IQVIA CORE Diabetes Model (CDM) was utilized for the analysis. Briefly, the CDM is a non-product-specific computer simulation model used to predict long-term clinical and economic outcomes and can be used for either type 1 or type 2 diabetes. It comprises 17 interdependent Markov sub-models that simulate the long-term natural history of people with diabetes via the occurrence of micro- and macrovascular diabetes-related complications. Details of the model structure and validation have been described previously by Palmer et al. 16,17 and McEwan et al. 18 In validation studies, the CDM achieved an R 2 value of 0.90 in T1DM against studies with a follow-up duration of less than 15 years and a R 2 value of 0.72 in a validation against 30-year outcomes from the Diabetes Control and Complications Trial. 18,19
Clinical data and cohort characteristics
The ADAPT RCT was used to inform the baseline cohort characteristics for the simulated population from which long-term outcomes were projected (as presented in Table 1; where input data were not available, model default settings were used). 14 Simulated patients had a mean baseline age of 40.6 years (standard deviation [SD] 12.35 years) and mean HbA1c of 9.04% (SD 0.85%) (75.3 [9.3] mmol/mol). Treatment effects associated with the MiniMed 780G and is-CGM were also taken from the ADAPT study; specifically, ADAPT reported an HbA1c reduction of 1.54% (16.8 mmol/mol) in the MiniMed 780G arm versus 0.2% (2.18 mmol/mol) in the is-CGM + MDI arm. In the base case analysis, no severe hypoglycemic events (events requiring either medical or nonmedical assistance) were assumed for either arm.
Simulation Cohort Characteristics at Baseline
Values are mean (standard deviation).
HbA1c, glycated hemoglobin.
Costs
The annualized device cost for the MiniMed 780G was EUR 8032, while annual costs of is-CGM were EUR 1678. Costs of the MiniMed 780G and is-CGM + MDI assumed use of 54 and 26 sensors per year, respectively. Insulin costs were based on the ADAPT study, with an assumed total for the MiniMed 780G of 54 units per day. 14
The annualized cost of the MiniMed 780G was calculated based on the procurement condition and on the outpatient “Liste des prestations et produits remboursables” (LPPR) tariffs in France at the time of the analysis. This calculation included the assumption that the device would be periodically replaced in accordance with the warranty terms. It was assumed that the GuardianTM 4 Link kit (including the transmitter, charger, cleaning plugs, battery, and One-press Serter) would be replaced annually.
All product and insulin costs in both arms, namely the MiniMed 780G and MDI + isCGM, and the additional payments to service providers for the initial pump training, quarterly follow-ups, and monthly delivery of consumables needed for the MiniMed 780G use, were sourced from the published LPPR tariffs.
Costs of diabetes complications incurred in the “index year” (i.e., the year of the event or the year of onset of chronic conditions), and costs incurred in subsequent years were modeled based on unit costs from a previous economic analysis 20 and inflated to 2023 values using the health consumer price index from the Institut national de la statistique et des études économiques 21 (Table 2).
Costs of Diabetes-Related Complications
All costs were sourced from a previous economic analysis by Roze et al. 20 and inflated to 2023 values.
NSHE, non-severe hypoglycemic event; SHE 1, severe hypoglycemic event requiring third-party assistance; SHE 2, severe hypoglycemic event requiring medical assistance.
Utilities
Utility values for acute and long-term diabetes-related complications were sourced from published literature. 22 –27 The analysis also included the impact of is-CGM + MDI and the MiniMed 780G on quality of life arising from a reduction in fear of hypoglycemia (FoH). FoH data from the ADAPT study were converted to utilities using research suggesting that a one-point improvement in FoH as measured by the Hypoglycemia Fear Survey resulted in a utility gain of 0.008. 28 Based on the ADAPT study, utility benefits of 0.0544 and 0.016 were assumed for the MiniMed 780G and is-CGM arms, respectively. While 12-month utility data were available for the MiniMed 780G, only 6-month data were available for the is-CGM + MDI arm, as people in the is-CGM + MDI arm were switched to the MiniMed 780G at 6 months for a 6-month continuation phase.
Time horizon, perspective, and discount rates
The base case analysis was conducted from a French national payer perspective over a 40-year time horizon. A 2.5% annual discount rate was applied to future costs and clinical accounts in line with 2020 recommendations by Haute Autorité de Santé. 29
Sensitivity and scenario analyses
Sensitivity analyses were conducted to test the uncertainty associated with parameter variability. Parametric uncertainty was explored through deterministic and probabilistic sensitivity analysis. Parameters explored in deterministic analyses included 20% changes in the 1.54 percentage point reduction in HbA1c, 20% change in the additional utility score for FoH, and 20% changes in complication costs.
Scenario analyses were also carried out to test the impact of certain modeling decisions, such as the time horizon, the choice of source to utility values (alternative sets of diabetes complication utilities were taken from reviews by Beaudet et al. 30 and Smith-Palmer et al. 27 ).
A scenario analysis was also conducted in which data from the recent Christensen et al. RCT were used to inform the baseline cohort characteristics and treatment effects. 31 Christensen et al. reported the findings of an RCT comparing the MiniMed 780G with CGM in concert with an insulin pump rather than MDI with CGM. Participants enrolled in the Christensen et al. RCT had a baseline HbA1c of 8.3% (SD 0.6%) (67 mmol/mol [SD: 7 mmol/mol]), a diabetes duration of 29 years (SD: 13 years), and a mean age of 52 years (SD 11 years). HbA1c decreased by 0.9% (95% CI: 0.6%, 1.2%) (10.0 mmol/mol [95% CI: 7.0, 13.0 mmol/mol]) in the group managed with the MiniMed 780G but remained unchanged in the usual care group (P < 0.0001).
Probabilistic sensitivity analyses were conducted by running 1000 iterations of 1000 patient cohorts through the model and generating incremental cost and quality-adjusted life expectancy estimates for each iteration. Each iteration was plotted on the cost-effectiveness plane, and a cost-effectiveness acceptability curve was generated showing the likelihood of the MiniMed 780G being cost-effective over a range of willingness-to-pay thresholds from EUR 0 to EUR 200,000 per quality-adjusted life year (QALY) gained.
Results
Base case analysis
Results from the base case analysis are presented in Table 3. In summary, in PWD unable to achieve adequate glycemic control with is-CGM + MDI, use of the MiniMed 780G resulted in an improvement in quality-adjusted life expectancy of 2.26 QALYs versus is-CGM + MDI. Total direct costs with the MiniMed 780G were EUR 78,509 higher than with is-CGM + MDI. The incremental cost-utility ratio (ICUR) for the MiniMed 780G versus is-CGM + MDI in PWD who have poor glycemic control in France was therefore EUR 34,732 per QALY gained (Table 3).
Results of the Base Case Analysis
EUR, Euros; ICUR, incremental cost-utility ratio; is-CGM + MDI, intermittently scanned continuous glucose monitoring plus multiple daily injections; MM780G, MiniMed™ 780G; QALY, quality-adjusted life year.
PWD managed with the MiniMed 780G were also projected to have substantially reduced incidence of diabetes-related complications over the 40-year time horizon; on average PWD managed with the MiniMed 780G experienced an additional 2.89 years alive and free of any complication (Fig. 1). The projected cumulative incidence of most long-term complications was also reduced in the MiniMed 780G arm. For example, the cumulative incidence for heart failure was estimated at 5.4% for the MiniMed 780G arm versus 7.0% for the is-CGM + MDI arm. Similarly, the cumulative incidence of stroke was estimated at 5.6% for the MiniMed 780G arm versus 7.3% for the is-CGM + MDI arm (Supplementary Table S1). Long-term complications such as cardiovascular or renal complications can be associated with high direct costs; the present analysis demonstrated that the higher device costs associated with the MiniMed 780G were at least partly offset over a long-term time horizon by the lower incidence of costly long-term complications (Table 3).
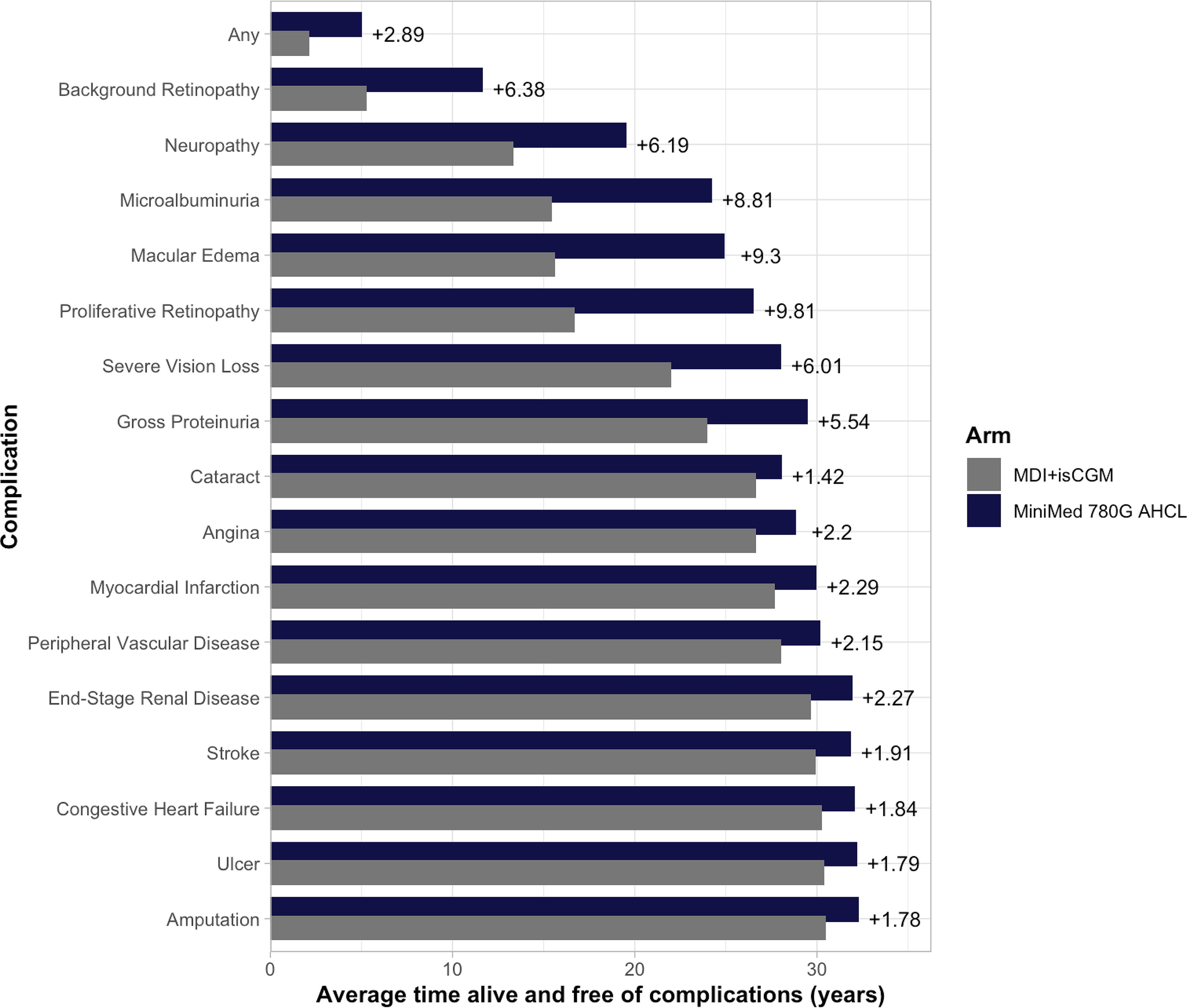
Average time alive and free of complications. AHCL, advanced hybrid closed loop; is-CGM + MDI, intermittently scanned continuous glucose monitoring plus multiple daily injections.
Sensitivity and scenario analyses
In analyses of parametric uncertainty, one-way sensitivity analysis showed that the model was relatively insensitive to changes in individual model parameters (Supplementary Fig. S1). Reducing the HbA1c benefit of the MiniMed 780G by 20% had a modest effect on the ICUR, increasing it to EUR 44,491 per QALY gained, with the changes driven by both higher incremental costs and a smaller improvement in quality-adjusted life expectancy relative to is-CGM + MDI. Reducing the utility benefit associated with reduced FoH (by 20%) resulted in the ICUR increasing to EUR 38,781 per QALY gained and abolishing the effect on FoH derived from ADAPT increased the ICUR to EUR 55,430 per QALY gained, driven by the reduction in incremental quality-adjusted life expectancy from 2.260 QALYs in the base case to 1.416 QALYs without the FoH utility. Additionally, in the base case, no severe hypoglycemic events were assumed to have occurred in either arm; if these were changed to 32 per 100 patient-years for AHCL and 64 per 100 patient-years for is-CGM + MDI, the ICUR was lower than in the base case analysis at EUR 31,625 per QALY gained. Overall, none of the parameters tested in the deterministic analyses of the clinical effects had more than proportional impact on the ICUR.
In addition, scenario analyses testing modeling choices relating to time horizon and comparator were conducted (Table 4). Specifically, a 30-year analysis resulted in an ICUR of EUR 41,816 per QALY gained, driven by the shorter time frame over which the longer-term benefits of improved glycemic control could manifest. The scenario analysis reporting the findings of a comparison based on Christensen et al.’s RCT showed that the MiniMed 780G would be dominant over the combination of CGM and an insulin pump, reducing costs by EUR 7003 over a 40-year time horizon and leading to an improvement in quality-adjusted life expectancy of 0.817 QALYs (Table 4).
Summary of One-Way Sensitivity Analysis Results
AHCL, advanced hybrid closed-loop; CSII, continuous subcutaneous insulin infusion; FoH, fear of hypoglycemia; is-CGM + MDI, intermittently scanned continuous glucose monitoring plus multiple daily injections; PSA, probabilistic sensitivity analysis; SHE, severe hypoglycemic event.
In the probabilistic sensitivity analysis, 99.9% of results from the 1000 model iterations fell in the northeast quadrant of the cost-effectiveness plane, corresponding to increased costs and increased quality-adjusted life expectancy with the MiniMed 780G versus is-CGM + MDI (Fig. 2). The average ICUR for the MiniMed 780G versus is-CGM + MDI over 1000 model iterations was EUR 37,926 per QALY gained, closely aligned with the deterministic base case analysis (EUR 34,732 per QALY gained). Using the 1000 model iterations to plot a cost-effectiveness acceptability curve showed that, as expected, the likelihood of the MiniMed 780G system being considered cost-effective increased as the assumed willingness-to-pay threshold increased (Fig. 3).
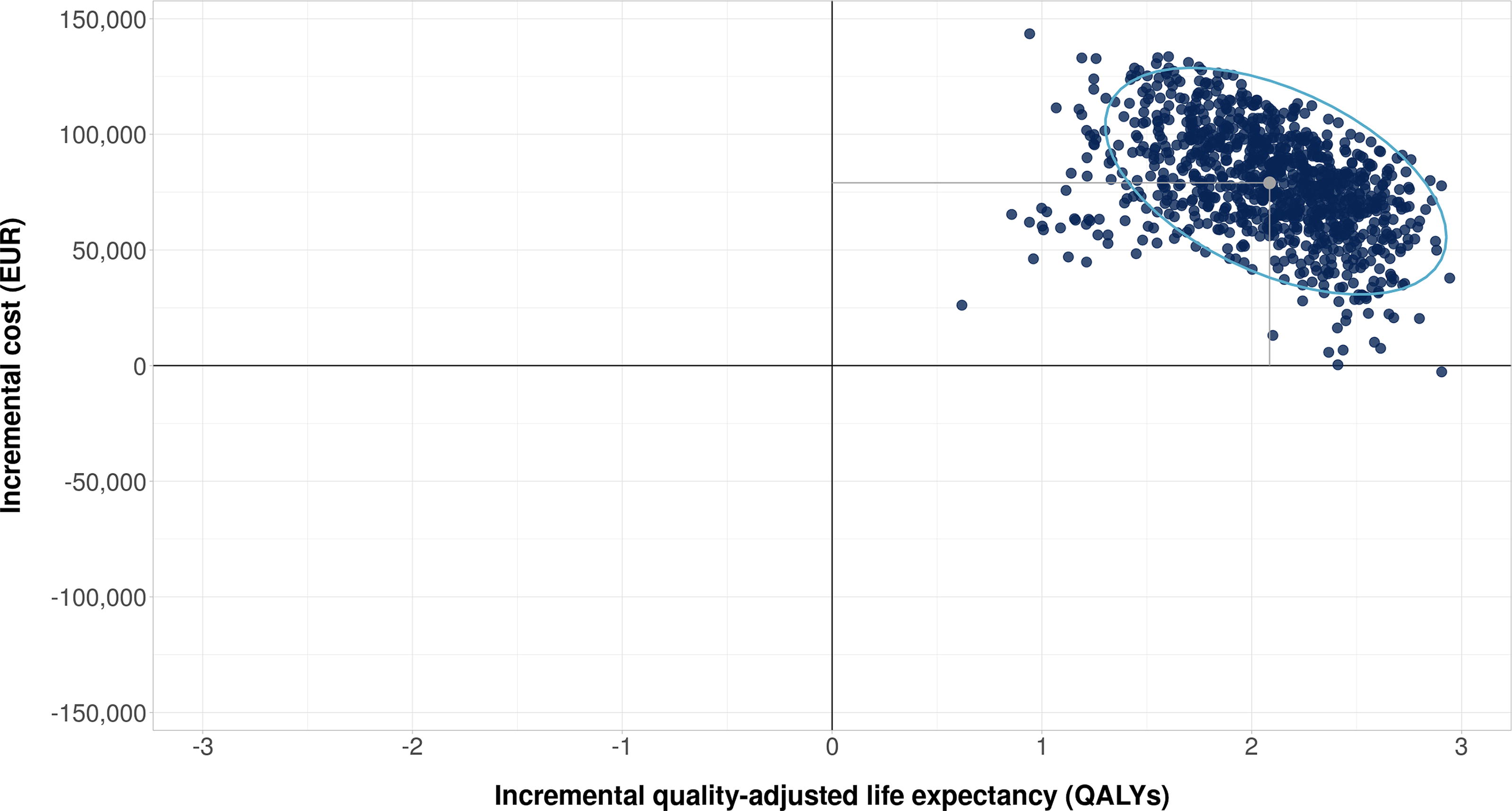
Cost-effectiveness scatter plot from the probabilistic sensitivity analysis. Gray point represents mean incremental cost and quality-adjusted life-year (QALY) outcomes from all iterations. Blue ellipse is a data ellipse at the 95% level assuming a multivariate T-distribution.
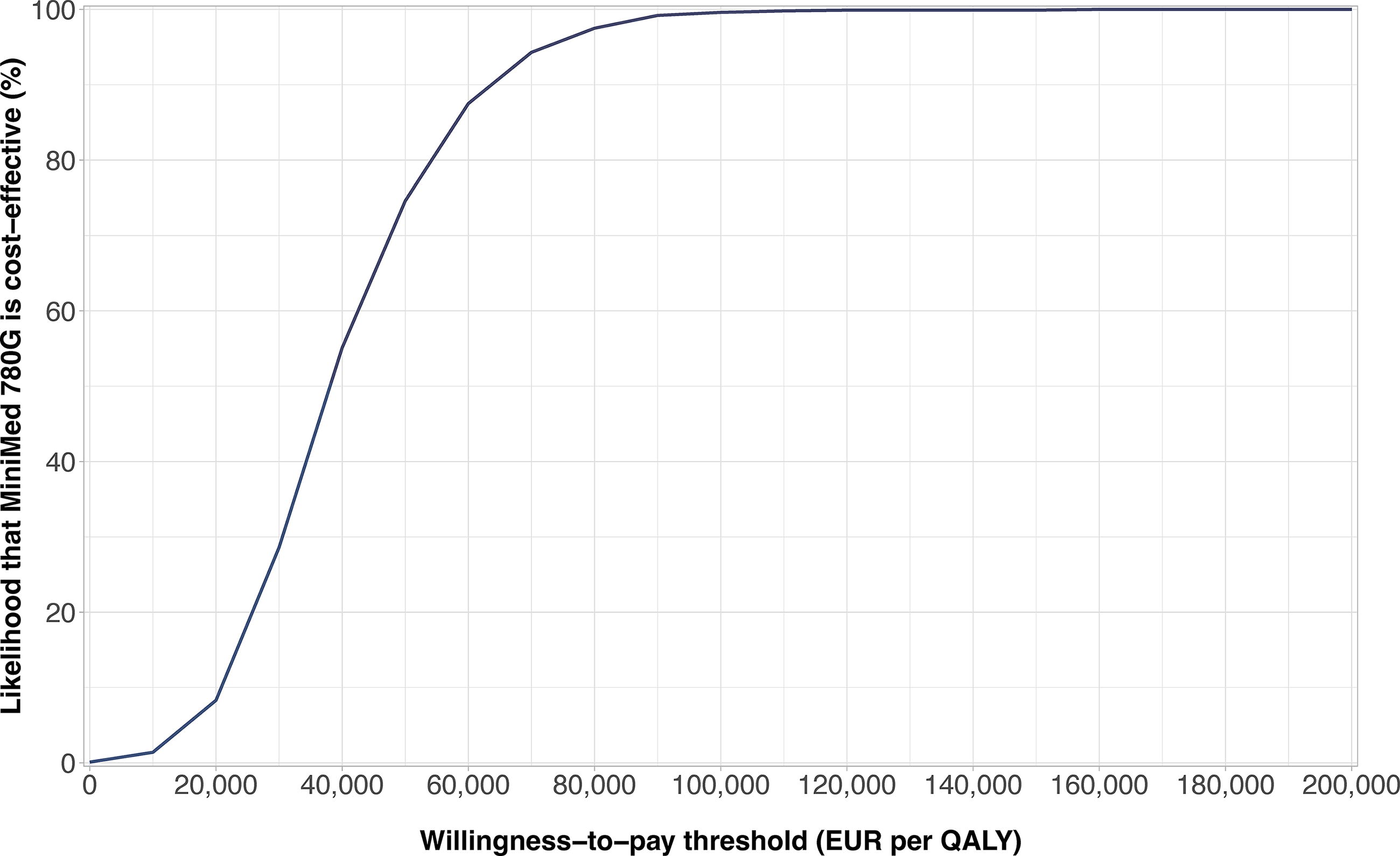
Cost-effectiveness acceptability curve based on 1000 iterations from the probabilistic sensitivity analysis over willingness-to-pay thresholds from EUR 0 to EUR 200,00 per QALY.
Discussion
The present analysis demonstrated that, in PWD who were unable to achieve adequate glycemic control with is-CGM + MDI, the use of the MiniMed 780G resulted in an improvement in mean quality-adjusted life expectancy versus is-CGM + MDI. This was driven by the substantial HbA1c benefit in the MiniMed 780G arm. Clinical input data were sourced from the ADAPT RCT, as such the modeled reductions in HbA1c were −1.54% (SD 0.73) in the MiniMed 780G arm and −0.2% (SD 0.8) for is-CGM + MDI. The clinical evidence base from the ADAPT trial has been consolidated with a growing body of evidence from large-scale real-world studies, showing the MiniMed 780G is also highly effective in routine clinical practice, particularly when optimal system settings are utilized. 32 For example, a recent 12-month observational study in France showed that initiation of the MiniMed 780G led to a significant improvement in the percentage of people able to achieve a HbA1c target of <7% at 12 months post-initiation compared with baseline. 12 Of note, trials and real-world analyses of AID systems frequently include endpoints such as TIR and time-below-range. However, in the CDM, outcomes are largely driven by HbA1c; the model does not currently have the functionality to incorporate TIR as studies on TIR and long-term outcomes are currently lacking. Evidence from the ADAPT RCT is now supplemented by a large body of real-world analyses, which have consistently shown that use of the MiniMed 780G is effective across a broad spectrum of patient populations. For example, in terms of age-groups, real-world effectiveness has been demonstrated people aged under and over 15 years as well as in older adults. 33,34 In the ADAPT study specifically, a significantly higher proportion of MiniMed 780G users achieved a TIR greater than 70% compared with users of is-CGM + MDI (P < 0.0001). 14
Despite the clinical benefit, a potential barrier to the widespread uptake of the MiniMed 780G is the higher cost relative to is-CGM + MDI. However, due to the significant improvement in glycemic control with the use of the MiniMed 780G, the relatively high treatment cost is partially mitigated by the reduced incidence of diabetes-related complications and the subsequent costs of care. This improvement in glycemic control was projected to lead to a more favorable long-term disease trajectory. Over 40 years, the use of the MiniMed 780G was projected to result in a substantial reduction in the cumulative incidence of long-term complications as well as a projected extra 2.89 years free of any long-term complications compared with is-CGM + MDI. Diabetes-related complications lead to a significant economic burden in France, costing a reported EUR 4.2 billion annually. 6 Therefore, any reduction in the incidence of complications would be beneficial clinically, economically, and logistically when considering health care system capacity. It is important to note that, as the population of this analysis are PWD who have suboptimal glycemic control, the cost-effectiveness of the treatments in those between adequate HbA1c levels and 9% could not be assessed. However, in a recent small-scale RCT in 40 adults with T1DM with a baseline HbA1c of 8.3%, after 14 weeks, use of the MiniMed 780G was associated with a reduction in HbA1c of 0.9%. HbA1c did not change significantly in the usual care arm, which consisted of PWD using insulin pumps in combination with CGM. 31 A scenario analysis was conducted based on this analysis, and here the MiniMed 780G was dominant versus insulin pumps plus CGM in this population with a baseline HbA1c of 8.3%. Further studies would be required to examine the HbA1c treatment effects with the MiniMed 780G versus is-CGM + MDI with baseline HbA1c values between 7% and 9%. Such an analysis would likely be of considerable interest in the French setting specifically as a recent study estimated the median (interquartile range) HbA1c in PWD aged ≥25 years in France to be 8.0% (7.0%–9.0%). 35 Allied to this, another burdensome aspect of T1DM that was quantified in the present analysis is FoH, which can be a barrier to good glycemic control. 36 In the ADAPT study, use of the MiniMed 780G was associated with a more pronounced effect on FoH than is-CGM + MDI. 14 The benefit of reduced FoH was captured in the present analysis through the assumption that reduced FoH would lead to an improved quality of life. Indeed, if the utility benefit associated with reduced FoH was entirely removed, the ICUR increased substantially to EUR 55,430 per QALY gained. Further studies are needed to more directly assess the relationship between FoH and quality of life and also to examine the effect of AHCL on FoH in people with different levels of glycemic control.
Although this is the first cost-utility analysis comparing the MiniMed 780G and is-CGM + MDI in France, the findings are supported by previous studies including a multi-country study, which also demonstrated the MiniMed 780G to be cost-effective versus is-CGM in multiple European settings. 15 Two other recent analyses were conducted in Greece and Sweden, and, while they pre-dated the availability of results from the ADAPT study, they also found the MiniMed 780G to be cost-effective, 37,38 corroborating the findings of the present study in yet more European health care settings.
In ascertaining whether health care interventions are cost-effective in the French setting, it is important to note that there is currently no official reference value for the assessment of the cost-effectiveness of new technologies in France. New interventions for which the manufacturer claims either moderate or major added value are evaluated based on a combination of factors including clinical benefit, disease severity, safety, and place in therapy relative to existing interventions. 39 However, in a review of health economic analyses with opinions published over the period 2014–2016, half of those assessed (6/12) had ICURs that exceeded EUR 50,000 per QALY. 40 A more recent analysis of opinions published by the Commission d’évaluation économique et de santé publique showed that in 2023 alone, there were 25 published opinions (with 27 results in total, including subpopulations reported in terms of cost per QALY gained). Overall, 19 out of the 27 (70%) reported ICURs of over EUR 50,000 per QALY gained. 41 The ICUR reported in the present analysis was EUR 34,732 per QALY gained; based on mean incremental costs of EUR 78,509 and a mean incremental utility benefit in excess of two QALYs, the analysis suggests that PWD with suboptimal baseline control can derive substantial long-term clinical benefit from use of the MiniMed 780G. The ICUR is in line with those reported for other new interventions in France, falling below the EUR 50,000 per QALY threshold utilized to stratify analyses in the review by Cartier-Bechu et al. 40 The ICUR reported here is also likely to be considered good value if considering the approach of Tehard et al. in terms of the value of a statistical QALY in France. 39
The present analysis was carried out from a French national payer perspective and therefore omitted the societal perspective benefits of treatment with the MiniMed 780G. Specifically, indirect costs associated with lost productivity were not captured. Given the lower rates of complications projected for the MiniMed 780G arm, this would be anticipated to translate into lower costs associated with lost productivity, and the omission of such costs would therefore likely be conservative from the MiniMed 780G perspective. Furthermore, economic analyses are not designed to capture more intangible aspects such as caregiver burden or parental distress, which has been shown to be reduced with the use of the MiniMed 780G. 42 Nevertheless, clinical benefits would be consistent irrespective of perspective, and, moreover, in the sensitivity and scenarios performed, the results were shown to be robust to changes in input parameters and assumptions. Additionally, given the potential benefits of modern T1DM management technologies from the patient perspective, it has been suggested that patient preferences should be considered in the selection of an appropriate treatment. Indeed, a 2021 consensus report from the American Diabetes Association and the European Association for the Study of Diabetes noted that “management strategies should adapt to new therapies and technologies as they become available, according to the wishes and desires of the person with diabetes.” 4
The analysis presented here is associated with limitations. In particular, short-term data were used to project long-term complications, although in the absence of long-term clinical data over the time horizon to match that of the analysis, this was unavoidable. The EuroQoL 5DPSA: probabilistic sensitivity analysis (EQ-5D) utility values used were also derived from multiple studies across different settings and were not specific to the French population. Van Dongen et al. recently showed that utility values can vary considerably across different settings, which the authors attributed to sociocultural differences. This may, in turn, have a considerable impact on the findings of cost-utility analyses. 43 However, it was not possible to source a full set of values specific to the French population from a single study. The use of utility values derived from methods such as standard gamble or time trade-off was not explored; there are both advantages and limitations around the use of methods for obtaining utility values.
In conclusion, the results of the analysis showed that the use of the MiniMed 780G in PWD not achieving target HbA1c levels with is-CGM + MDI resulted in improved quality-adjusted life expectancy compared with remaining on is-CGM + MDI. Moreover, the findings of the analyses were found to be robust and parametric uncertainty was low. These results may provide a useful insight for decision makers. The higher up-front cost of the MiniMed 780G from a payer perspective should be considered alongside the substantial clinical benefits associated with its use, leading to a reduction in the long-term incidence of complications of T1DM and the associated clinical and economic burden, thus suggesting the MiniMed 780G is a worthwhile investment in improving the lives of PWD.
Footnotes
Author Disclosure Statement
A.Z.O.S., S.D.P., P.K., and O.C. are current employees of Medtronic. N.N. and R.F.P. are current employees of Covalence Research Ltd., which has received consulting fees in relation to the preparation of this article from Medtronic. C.S. and A.G. are current employees of Vyoo Agency, which has received consulting fees from
Funding Information
Funding related to the preparation of this article was provided by Medtronic International Trading SARL, Tolochenaz, Switzerland.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.