
Abstract
Periodontal infections can increase patients' serum C-reactive protein (CRP) level, which is a predictive marker of future cardiovascular events. Serum CRP may be a key mediator associating periodontitis with cardiovascular disease. It is not yet clarified whether the chemotactic activity of monocytes changes with increased serum CRP. This study investigated the influence of CRP on monocyte chemotaxis and the effects of CRP on CC chemokine receptor 2 (CCR2) expression by monocytes in vitro. Monocyte cell line THP-1 was cultured with human recombinant CRP of different final concentrations, which were 2, 4, 6, 8, and 10 mg/L, respectively. After 24 h incubation, Transwell chambers were applied to analyze the chemotactic activity of pretreated monocytes. Flow cytometry analysis and real-time reverse transcription–polymerase chain reaction (RT-PCR) were applied to detect the CCR2 protein and gene expression levels. In Transwell chambers, more cells were attracted in CRP-pretreated groups than that of blank control with no CRP (p<0.05). The chemotaxis activity was stronger in higher CRP concentration groups than lower ones (p<0.05). The CCR2 protein and mRNA expression was increased in a CRP concentration-dependent manner (p<0.05). CRP stimulation may induce CCR2 overexpression on monocytes and then promote the chemotaxis ability of monocytes. This result suggests that increased serum CRP concentration of periodontitis patients may be associated with high risk of cardiovascular disease.
Introduction
Inflammation caused by periodontitis can lead to increase of serum CRP levels. Increased serum CRP levels were found to be a strong and independent risk factor of future cardiovascular events (Ridker et al., 1997, 1998, 2000, 2002, 2008; Koenig et al., 1999). More than just a risk marker, a growing body of evidence suggests that CRP may indeed participate in atherogenesis. Published data have demonstrated that CRP localizes in athersclerotic, but not normal, intima, induces production of cell adhesion molecules, decreases endothelial nitric oxide synthase expression, triggers oxidation of low-density lipoprotein cholesterol and mediates low-density lipoprotein uptake by macrophages (Inoue, 2006; Singh et al., 2008). Therefore, serum CRP may be a key mediator associating periodontitis with CVD (Ridker and Silvertown, 2008). There are few studies about the influence of increased serum CRP on monocyte chemotactic activity. This study aimed to investigate effects of CRP on chemotactic activity of monocytes in vitro and its possible mechanism to explore the role of CRP as an inflammation mediator in connecting periodontitis and CVD.
Materials and Methods
Cell culture and pretreatment
Monocyte cell line THP-1 was supplied by State Key Laboratory of Oral Disease, Sichuan University. THP-1 cells were cultured in RPMI 1640 medium (HyClone). The concentration of cells was adjusted to 5×105 cells/mL and 1.98 mL cell suspension was inoculated in each well of a 24-well plate. Human recombinant CRP (1 mg/mL; Calbiochem) was added at different final concentrations, which were 2, 4, 6, 8, and 10 mg/L in Groups 1, 2, 3, 4, and 5, respectively. Culture medium was added to make total volume reach 2 mL in each well. Moreover, no CRP was applied to stimulate monocytes in the control group. Cells were incubated under 5% carbon dioxide (CO2) at 37°C for 24 h.
Chemotactic activity analysis
Transwell chambers (Costar) were used to analyze the chemotactic activity of monocytes pretreated with CRP. The pretreated monocytes were collected by centrifugation, washed three times, and resuspended in phosphate-buffered saline solution (PBS). Monocyte suspension was transferred into upper chambers; medium with monocyte chemoattractant protein-1 (MCP-1) (500 ng/mL; Peprotech) was in the lower chambers. A nitrate cellulose membrate (pore size 5 μm) separated the upper and lower chambers. Each group contained a negative control, in which antibody to MCP-1 was applied in the lower chamber to neutralize chemotaxis of MCP-1. Every group was replicated in three chambers.
The transwell chambers were incubated in 5% CO2 at 37°C for 60 min. The filter membrane was obtained, and the upper side next to the cell suspension was rinsed and wiped to remove nonspecific attached cells. The membrane was fixed with 1% paraformaldehyde. Gimesa stain was applied to dye monocytes attached to the membrane. The number of cells was counted under a microscope. The final number of chemotactic cells was calculated by the mean number of three replicates of each group minus that of the corresponding negative control.
Flow cytometry analysis
Monocytes incubated with CRP were harvested from the 24-well plate and resuspended in PBS. The cells were collected by centrifugation. Murine IgG was supplemented in each group to block nonspecific Fc receptors. CC chemokine receptor 2 (CCR2) was detected by specific antibody. The homotype antibody was used to control for nonspecific antibody binding.
The cells treated with antibodies were incubated at 37°C for 40 min and washed with PBS to remove unbound antibodies. Then, the cells were centrifuged and suspended in PBS for flow cytometry analysis. Every test was repeated three times. The quantity of relative CCR2 expression was evaluated by mean fluorescent intensity, which was obtained by mean fluorescent intensity of test groups minus that of the corresponding control group. All data were analyzed by CeLLquest software (Becton Dickinson).
Real-time RT-PCR analysis
Total RNA of pretreated cells was extracted using Trizol (Invitrogen) and was used as template in RT-PCR to produce complementary DNA. The primers for CCR2 were 5′ ATGCCTCATTACCTTGTGCTAATCC 3′ (forward) and 5′ CCCATTCATCTGTGCCTGTCA 3′ (reverse). The primers for glyceraldehyde phosphate dehydrogenase (GAPDH), which acted as a reference, were 5′ GCACCGTCAAGGCTGAGAAC 3′ (forward) and 5′ TGGTGAAGACGCCAGTGGA 3′ (reverse). Real-time RT-PCR system included 10 μL of 2X Takara SYBR Premix Ex Taq™, 0.4 μL of 50X ROX Reference, 10 nM CCR2 or GAPDH primers, 2 μL cDNA, and diluted with H2O for a total volume of 20 μL. Preliminary experiments were carried out to optimize the reaction conditions: denaturation at 95°C for 5 s, annealing at 60°C for 31 s, and extension at 72°C for 30 s, repeated for 40 cycles. PCR products were tested by electrophoresis. A standard curve was calculated with LightCycler software 3.5 and the quantity of CCR2 mRNA determined.
Results
THP-1 monocytes were stained bluish violet by Gimesa and spread over the filter membrane between the upper and lower chambers. The numbers of chemotactic cells stimulated by CRP are shown in Table 1. More cells were attracted in the CRP-pretreated groups than that of blank control with no CRP (p<0.05). The variance of cell quantity among test groups is statistically significant (p<0.05). Chemotactic cell quantity was positively related to CRP concentration.
Test group versus blank control: p<0.05.
Test group versus test group: p<0.05.
CRP, C-reactive protein.
CCR2 protein on the cell surface in each test group was more intensively expressed than that of blank control (p<0.05). When compared among test groups, stronger CCR2 protein expression was detected in the higher CRP-pretreated group (Fig. 1A) (p<0.05). The CCR2 protein level of Group 5, in which CRP concentration was 10 mg/L, was 1.74-fold of control (Table 2). The CRP-induced CCR2 protein increase was consistent with the change of CCR2 mRNA, which was 2.5-fold higher in the 10 mg/L CRP group than control.
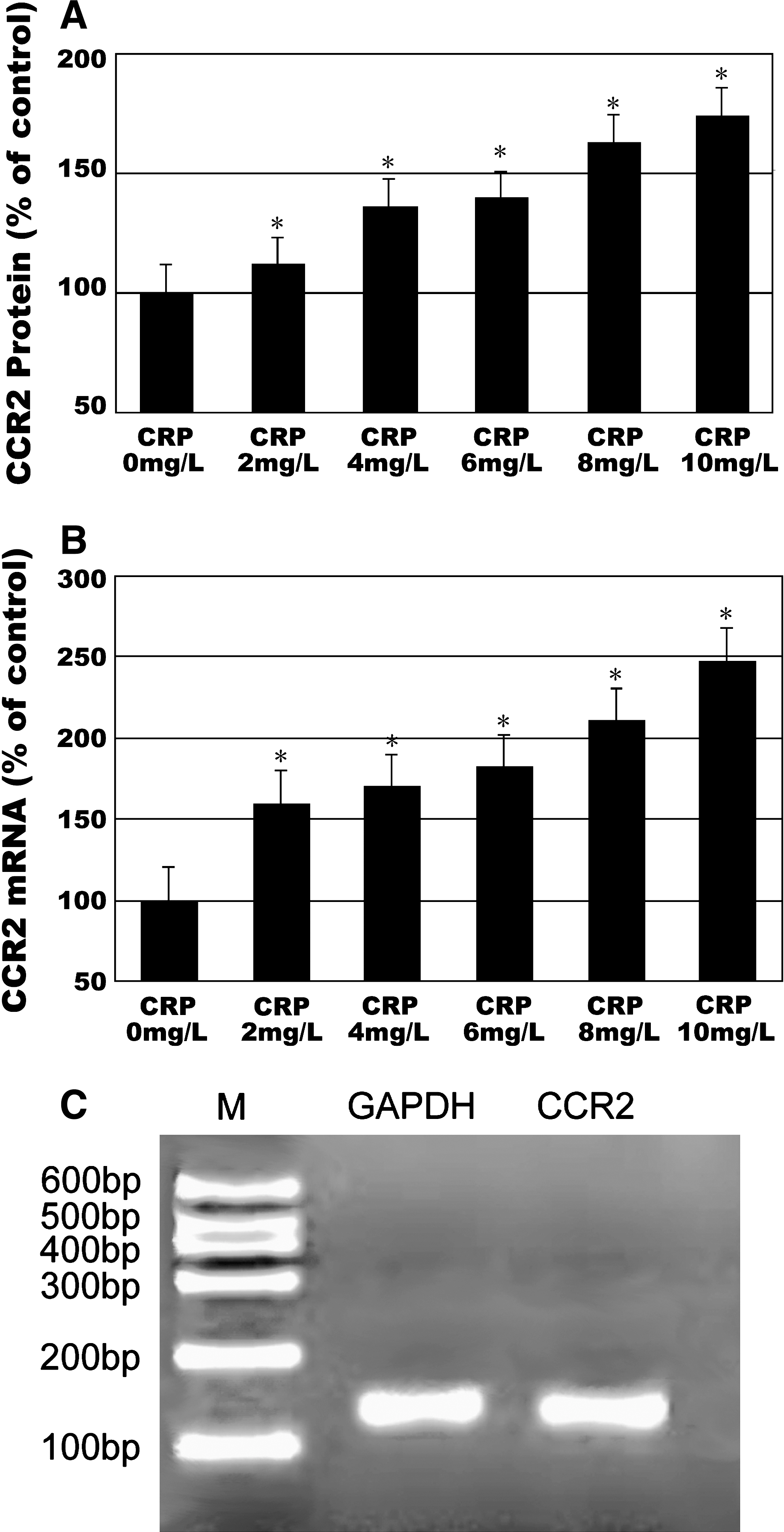
CRP stimulated CCR2 protein and mRNA expression.
Test group versus blank control: p<0.05.
Test group versus test group: p<0.05.
CCR2, CC chemokine receptor 2.
The CCR2 and GAPDH PCR products were analyzed by gel electrophoresis. Bands of the expected sizes (137 and 138 bp) were detected (Fig. 1C). Melting curves of real-time RT-PCR ascertained that CCR2 and GAPDH were the only amplicons. Standard curves showed linear correlation between Ct value and log DNA concentration (data not shown).
The relative quantity of CCR2 mRNA in monocytes of each test group was greater than in the blank control (p<0.05). The number of CCR2 mRNA copies increased as CRP concentration rose (Fig. 1B). The variance among different groups was statistically significant (p<0.05). When CRP reached 10 mg/L, the relative quantity of CCR2 mRNA increased to 247.61% of the control (Table 2).
Discussion
CVD is characterized by atherosclerosis; however, the conventional risk factors for atherosclerosis can account for only about 50%–70% of cardiovascular events in the general population. Accumulating evidence suggests that chronic infections, such as periodontitis, are associated with increased risk for CVDs. Several prospective studies have suggested a 1.5–2.5-fold increased risk of developing complications of atherosclerosis among patients with periodontal disease (DeStefano et al., 1993; Beck et al., 1996; Morrison et al., 1999; Wu et al., 2000a). The inflammation of periodontitis causes a systemic inflammatory response, as evidenced by elevated peripheral CRP (Wu et al., 2000b).
The American Heart Association has stated that CRP concentration is regarded as predictive marker of future cardiovascular events. CRP concentrations less than 1.0 mg/L are regarded as low risk, 1.0–3.0 mg/L, average risk, and more than 3.0 mg/L, high risk (Lloyd-Jones and Levy, 2003). However, serum CRP concentrations range from 1 to 10 mg/L in healthy periodontitis patients (Ebersole et al., 1997; Slade et al., 2000, 2003; Noack et al., 2001; Liu et al., 2010). Therefore, patients with periodontitis, who are otherwise healthy, may be included in the group of average or high risk for cardiovascular events. In patients with moderate or serious periodontitis, mean CRP concentration was 4.5 mg/L after adjusting confounding factors, and patients with CRP concentrations higher than 10 mg/L were 12.5% of this population (Slade et al., 2000). Thus, a majority of periodontitis patients are included in the high-risk population for cardiovascular events.
The present study has simulated the elevated serum CRP condition of periodontitis patients and proved that CRP can increase monocytes attracted by MCP-1 in a concentration-dependent manner, which suggests that chemotaxis activity of monocytes is positively associated with CRP levels. At the same time, increased expression of CCR2 protein and mRNA was detected in CRP-pretreated monocytes. Therefore, CRP may induce monocytes chemotaxis through upregulation of CCR2 and influence atherosclerosis development.
The CRP concentrations selected in our study ranged from 0 to 10 mg/L, which was designed to simulate the increasing serum CRP conditions in periodontitis patients of different severity. Moreover, in chronic inflammation such as periodontitis, serum CRP may gradually accumulate over a long period of time. As the serum CRP half-life is 19 h, the CRP treatment time was 24 h.
The THP-1 monocyte cell line was used in this study. Although human peripheral blood monocytes are an ideal experimental system to simulate the actual clinical pathophysiological conditions, the clinical samples would differ in the number and activity of monocytes for age, sex, heredity, environmental conditions, and physical conditions of the individual donor. These differences may increase the experimental error. The THP-1 monocyte cell line has greater cell numbers and consistency. Previous studies indicated that the CCR2 expression level of THP-1 cells is similar to that of freshly isolated human monocytes, and the cells show comparable chemotactic responses to MCP-1 (Tangirala et al., 1997; Han et al., 1998). The major advantage of using THP-1 cells is the homogeneity of the cell line, allowing comparison of findings in different experiments. For this reason, THP-1 cells were used in the present study to examine monocytes' chemotaxis to CRP, even though they were not absolutely identical to human peripheral monocytes.
MCP-1, also known as CC chemokine ligand 2 (CCL2), binds with CCR2 on the cell surface and mediates chemotaxis activity. Other cytokines, such as tumor necrosis factor-α and interleukin-1, can act as chemokines and CRP can stimulate tumor necrosis factor-α production of monocytes (Kleemann et al., 2008). In our study, after CRP pretreatment for 24 h, cells were centrifuged and rinsed before the chemotaxis experiment to exclude the chemokine activity of other cytokines promoted by CRP stimulation. In the negative control group, antibody to MCP-1 was applied in the lower chamber to neutralize chemotaxis of MCP-1 and block the chemotaxis activity of monocytes. As the concentration of MCP-1 was identical in each group, the number of attracted monocytes was determined by the amount of specific receptors expressed on cell surface. Circulating blood monocytes are the primary source of the lipid-laden foam cells in atherosclerotic lesions. There is evidence that MCP-1 plays a critical role in the recruitment of monocytes from the blood into early atherosclerotic lesions (Gerrity, 1981; Charo and Taubman, 2004). The effect of MCP-1 is mediated by the seven-transmembrane–spanning G protein–coupled receptor CCR2, which has been also recently designated as cluster of differentiation 192. CCR2 is a prominent receptor for MCP-1, a chemokine that specifically mediates monocyte chemotaxis (Boring et al., 1998; Guo et al., 2005). A previous study demonstrated that when the homeostasis of internal environment is acquired, a single monocyte expresses about 5000 CCR2 molecules on the cell surface, which is relatively low compared with other receptors (Tangirala et al., 1997). Thus, even a minimal alteration of receptor number would affect CCR2-mediated monocyte chemotaxis substantially. Reduction in CCR2 expression could attenuate monocyte chemotaxis and decrease atherosclerosis, and any increase in CCR2 expression could enhance the chemotactic response to MCP-1 and may promote the initial recruitment of monocytes to atherosclerotic lesions.
As a pro-inflammatory factor, CRP can influence expression of chemokines and their receptors. Several studies indicate that CRP can induce MCP-1 production by several cells to aggravate the inflammatory response (Zhong et al., 2006; Ryu et al., 2007; Bisoendial et al., 2009). In a previous study, CRP stimulation led to high concentrations of CCL expression, such as CCL2, CCL3, and CCL4, and downregulation of corresponding chemokine receptors CCR1, CCR2, and CCR5 in adherent monocytes, but not in circulating monocytes (Montecucco et al., 2008). The adherent monocytes (adhesion to polystyrene and endothelial monolayer) show a different response to CRP stimulation within suspension (mimicking circulation in the bloodstream), which may account for the different results obtained in our study. On the other hand, recent research found that CCR2 blockade treatment can inhibit MCP-1 binding and reduce serum CRP levels significantly in patients at risk for atherosclerotic CVD (Gilbert et al., 2011). We concluded that serum CRP increased by periodontitis may stimulate the chemotaxis of monocytes through CCR2 upregulation, suggesting that periodontitis patients may be at higher risk of atherosclerosis and CVDs. Further studies are necessary to investigate the interactions of CRP and chemokines/chemokine receptors.
Footnotes
Acknowledgment
This research was supported by the National Natural Science Fund of China (No. 30471890).
Disclosure Statement
No competing financial interests exist.