
Abstract
Ovarian cancer remains a challenging disease for which improved treatments are urgently needed. Tim-3 acts as a negative regulatory molecule and plays a critical role in immune tolerance. In the current study, we investigated the expression of Tim-3 on peripheral CD4+ T and CD8+ T cells in ovarian cancer. A total of 52 ovarian cancer patients and 56 healthy controls were recruited and leukocytes from peripheral blood mononuclear cells were analyzed for Tim-3 surface expression by flow cytometry. Data showed that expression of Tim-3 was significantly increased in both CD4+ and CD8+ T cells in ovarian cancer cases than in controls (p<0.0001 and p<0.0001, respectively). Patients who had recurrent ovarian cancer had a higher proportion of Tim-3+CD4+ T cells than when they were newly diagnosed (p=0.013). When analyzing Tim-3 expression with cancer progression, results revealed elevated Tim-3 expression in both CD4+ and CD8+ T cells in cases with advanced International Federation of Gynecology and Obstetrics (FIGO) staging (III/IV) than those with stage I and II (p=0.009 and p=0.037, respectively). We also tested Tim-3 with tumor grade, and observed that patients with a higher tumor grade (G3) demonstrated further augmented Tim-3 expression in CD4+ and CD8+ T cells compared to those with lower tumor grades (p=0.010 and p=0.042, respectively). Our study suggested that Tim-3 may participate in the development and progression of ovarian cancer by its negative regulation on various T-cell subsets, and Tim-3 expression in CD4+ T cells could serve as a predictive marker for anticancer therapies.
Introduction
Tim-3 is one of the Ig superfamily members and is preferentially expressed on fully differentiated Th1 lymphocytes, but not on Th2 cells (Monney et al., 2002). Studies have shown that Tim-3 may not contribute to the T-cell differentiation, but might perform a critical function in the Th1 cell transportation (Wang et al., 2008). The inhibitor activity of Tim-3 was first described in a series of autoimmune diseases (Monney et al., 2002). In the autoimmune disease model, the administration of Tim-3 antibody would result in the activation and expansion of the macrophage population, and then the more severe clinical symptom would be occurred (Sabatos et al., 2003). Another research showed that the administration of Tim-3-Ig in vivo would result in T-cell hyperproliferation and would abrogate the induction of tolerance during the development of immune responses (Zhu et al., 2005). When Tim-3 was interacted with its ligand, galectin-9, the Th1 responses would be a blockade by promoting the death of IFN gamma inducing Th1 cells (Geng et al., 2006). In the previous functional study, experimental data demonstrated that the soluble form of Tim-3 would reduce the antigen-specific T-cell responses and downregulate the anti-tumor immunity in vivo by inhibiting the Th1 responses (Van de Weyer et al., 2006). Recent studies have shown an important role of Tim-3 T-cell exhaustion in cancer. Tim-3-expressing CD4+ and CD8+ T cells, which produce reduced amount of cytokines, are significantly increased in lung cancer patients (Geng et al., 2006). Tim-3 and programmed death-1 (PD-1), another marker of T-cell exhaustion, are coexpressed on CD8 tumor infiltrating lymphocytes (TILs) in mice bearing transplanted tumors as well as on NY-ESO-1-specific CD8+ T cells in patients with advanced melanoma (Kuchroo et al., 2003). Blockade of Tim-3 pathways is effective in controlling tumor growth, suggesting that the Tim-3 pathway may act as one of the key factors in establishing T-cell exhaustion (Kuchroo et al., 2003).
It has been reported that ovarian tumors with dense CD3+CD8+ T-cell infiltrates are strongly associated with favorable clinical outcomes, suggesting that host immunity may play a role in delaying or preventing tumor recurrence after standard treatment (Nelson, 2008). Since Tim-3 downregulates T cell activation, we hypothesize that Tim-3 may affect the pathogenesis of ovarian cancer. In the present study, we examined the expression of Tim-3 on peripheral blood mononuclear cells (PBMCs) in ovarian patients and explored its correlation with various clinical characteristics.
Materials and Methods
Patients and controls
The study group included 52 ovarian cancer patients and 56 controls recruited from the Maternal and Child Health Hospital of Jinan City. The diagnosis of epithelial ovarian cancer was confirmed by histopathologic examination. Patients with nonepithelial-type neoplasia, patients treated before operation, and patients who were not treated surgically were excluded. Borderline tumors of the ovary were also excluded from this study.
The control population was recruited from people who came for general health examinations from the same hospital, and they were confirmed to be without any malignant diseases. All subjects were of Han Chinese ethnicity and were unrelated to each other. Each participant was interviewed in person with a structured questionnaire that elicited information on demographic factors and health characteristics. Venous blood was collected from each of the study participants. The study was performed upon the approval of the Review Board of the Maternal and Child Health Hospital of Jinan City.
Staining and flow cytometric analysis
The peripheral blood sample was incubated for 30 min in 4°C in a dark room with monoclonal antibodies or isotype matched control. Pe-Cy5-conjugated anti-human CD3, FITC-conjugated anti-human CD4, Pe-Cy5-conjugated anti-human CD8, PE-conjugated rat IgG2a isotype control (all from eBioscience), monoclonal PE-conjugated anti-human Tim-3, and human PD-1 affinity purified polyclonal antibody (R&D Systems) were used for flow cytometric analysis. At least 10,000 cells were analyzed using a Beckman Coulter flow cytometer (FC500) and the data were analyzed using the Cell Quest Program.
Statistical analysis
All data were analyzed using the GraphPad Prism 5 (GraphPad Software, Inc.). The student t-test and the Mann–Whitney nonparametric U test were used for comparison between groups. The Pearson correlation analysis was used to calculate the correlation coefficient. Value of p<0.05 is considered as a significant difference.
Results
Characteristics of the study population
The distributions of selected characteristics of the cases and controls are presented in (Table 1). Ovarian cancer cases and controls did not reveal any significant difference in age (p>0.05). Of the 52 ovarian patients, 34 (65.4%) cases were newly diagnosed and 18 (34.6%) were recurrent cancer. Most of the patients (48.1%) were histologically serous papillary carcinoma, whereas endometrioid carcinoma and clear cell carcinoma accounted for 21.2% and 19.2%, respectively. The International Federation of Gynecology and Obstetrics (FIGO) staging were also shown, in which 23.0% were in stage III and 48.1% were in stage IV. Analysis of the tumor grade revealed that 78.8% cases were in advanced tumor grade (grade 3).
Tim-3 expression on peripheral CD4+ and CD8+ T cells in ovarian cancer
Although Tim-3 was first cloned in differentiated Th1 CD4+ cells, many studies have indicated the expression of Tim-3 on various immune cells such as CD8+ T cells, which plays roles in antitumor responses (Kuchroo et al., 2003). We investigated the expression levels of Tim-3 on CD4+ T cells and CD8+ T cells from peripheral blood of 52 ovarian cancer cases and 56 healthy controls. As shown in (Figure 1A), increased proportion of Tim-3+ cells was detected on CD4+ T cells in ovarian cancer patients than in controls (mean±SEM 4.89%±0.38% vs. 0.75%±0.10%, p<0.0001). Similarly, the proportion of Tim-3 in CD8+ T cells was also significantly elevated in cases compared to controls (2.91%±0.30% vs. 1.07%±0.11%, p<0.0001) (Fig. 1B). The patient group included 34 cases who had primary cancer and 18 cases who developed to recurrent cancer after treatment. We compared the expression of Tim-3 on CD4+ T and CD8+ T cells between patients with primary cancer and healthy controls. Data showed that the expression of Tim-3 on CD4+T and CD8+ T cells was elevated in patients with primary cancer than in controls (4.12%±0.37% vs. 0.75%±0.10%, p<0.001; 2.89%±0.31% vs. 1.07%±0.11%, p<0.001). These results indicated that Tim-3 may be involved in the pathogenesis of ovarian cancer by its regulation on various immune cells.
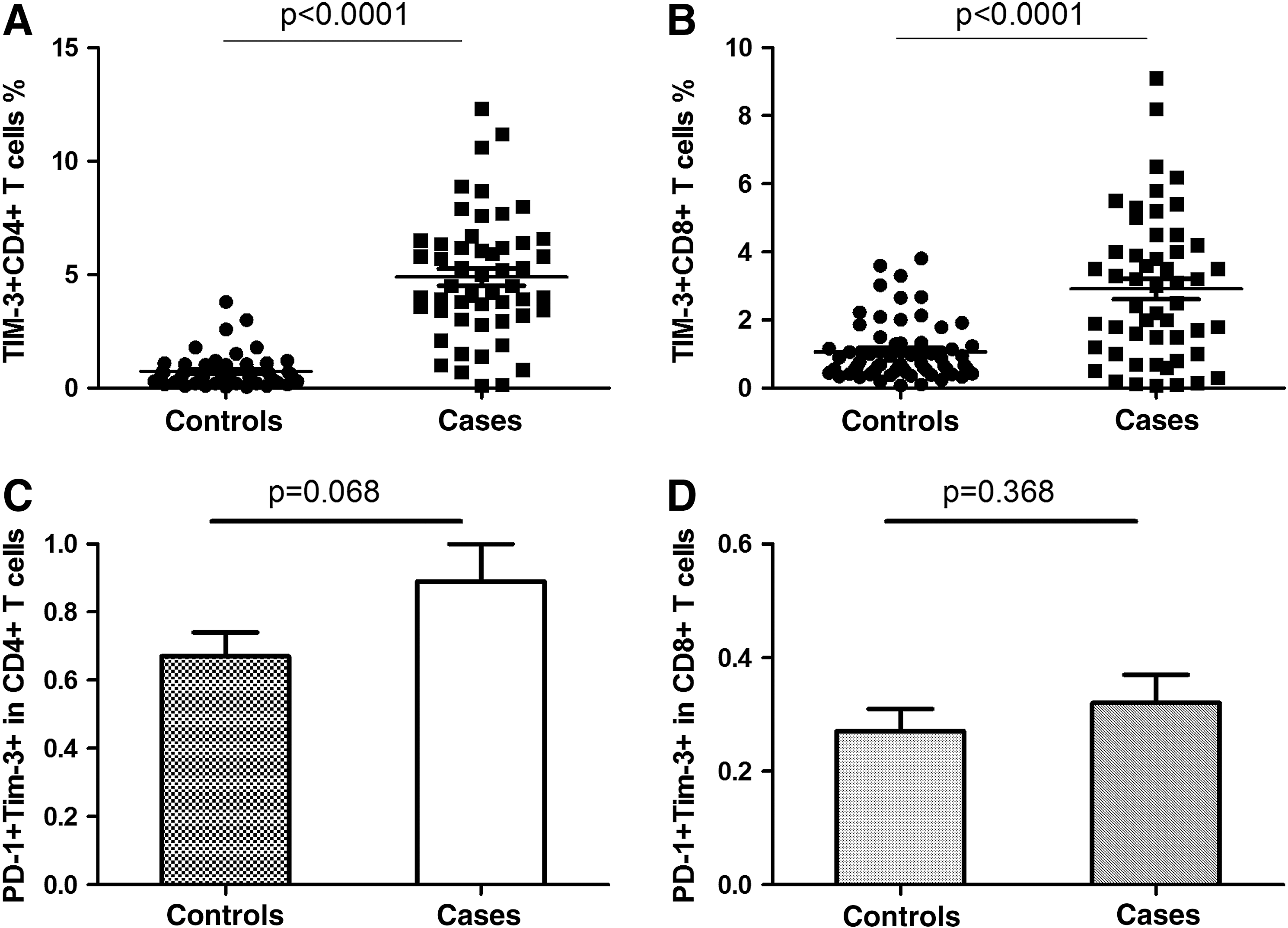
Tim-3 expression was increased on CD4+ and CD8+ T cell in ovarian cancer patients than in healthy controls.
PD-1 and Tim-3 coexpression on CD4+ and CD8+ T cells in ovarian cancer
Since Tim-3+PD-1+ T cells exhibit an exhausted phenotype of intratumor T cells in patients with advanced cancer (Sakuishi et al., 2010), we analyzed PD-1 expression in Tim-3+ CD4 and CD8 T cells. Our results showed that the proportion of PD-1+Tim-3+ in CD4+ T cells was increased in ovarian cancer patients than in healthy controls (0.89%±0.11% vs. 0.67%±0.07%). However, the difference did not reach statistical significance (p=0.068, Fig. 1C). Similarly, expression of PD-1+Tim-3+ in CD8+ T cells was slightly, but not significantly elevated in ovarian cancer patients (0.32%±0.05% vs. 0.27%±0.04%, p=0.368, Fig. 1D). It would be interesting to conduct an independent research on Tim-3 and PD-1 expression on TILs of ovarian cancer for comparison.
Tim-3 expression with the recurrence of ovarian cancer
Many ovarian cancer patients suffer from recurrence of the disease. We therefore investigated the correlation of Tim-3 expression on CD4+ T cells and CD8+ T cells with cancer recurrence. Of the 18 cases with recurrent cancer, 15 were diagnosed and treated in our department when they had primary ovarian cancer. We compared Tim-3 levels between the time they were newly diagnosed and the time they came for the recurrence of the disease. Results presented that patients progressed to recurrent disease had a significantly higher level of Tim-3 on CD4+ T cells than when they were at primary cancer status (6.95%±0.64% vs. 4.99%±0.36%, p=0.013, (Fig. 2A). However, we did not observe any obvious changes in the expression of Tim-3 on CD8+ T cells between recurrent disease and primary disease (3.81%±0.56% vs. 3.02%±0.39%, p=0.176, Fig. 2B). In addition, our results revealed that patients who did not progress to recurrent cancer and survived more than 5 years after surgery had significantly lower levels of Tim-3+CD4+ T cells and Tim-3+CD8+ T cells than when they were just diagnosed with ovarian cancer (1.92%±0.13% vs. 3.63%±0.17%, p=0.012; 1.53%±0.11% vs. 2.85%±0.20%, p=0.023, respectively). These data indicated that Tim-3 expression could have a predictive value for patients after therapeutic intervention. In addition, we compared the primary status of Tim-3 expression between patients who responded to the treatment well (more than 5 years of survival) and those who progressed to recurrent cancer. Data demonstrated that at the time of primary diagnosis, patients progressing to recurrent cancer at a later stage had significantly higher levels of Tim-3+CD4+ T cells (4.99%±0.36% vs. 3.63%±0.17%, p=0.035), but not Tim-3+CD8+ T cells (3.02%±0.39% vs. 2.85%±0.20%, p=0.855, respectively). These results demonstrated that Tim-3 expression on CD4+ T cells was associated with the recurrence of ovarian cancer, could serve as a predictive marker for anticancer therapies.
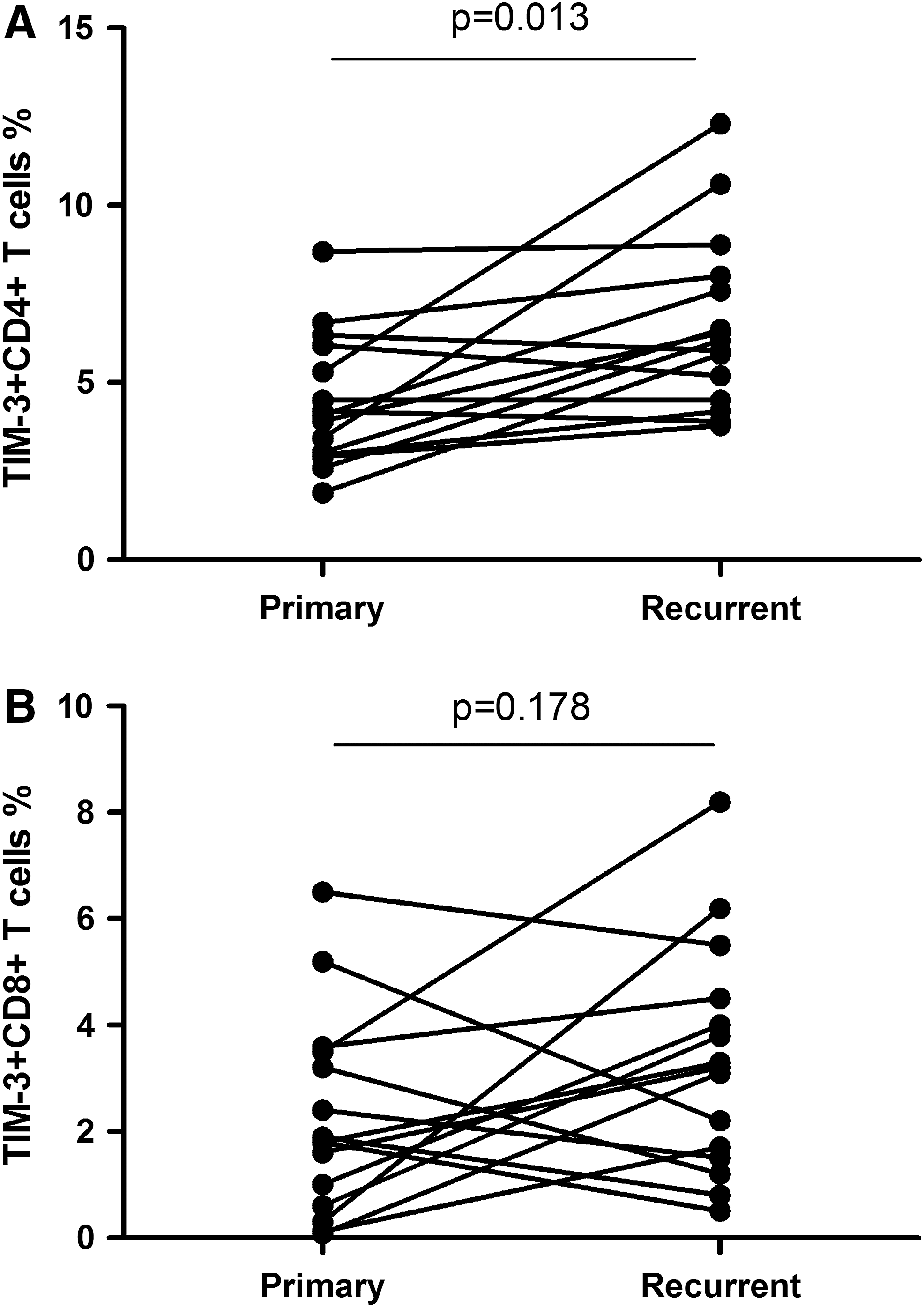
Comparison of Tim-3 expression on CD4+
Tim-3 expression on CD4+ and CD8+ T cells in patients with different FIGO stages
To learn whether Tim-3 may affect the spread of the tumor, we examined the Tim-3 level with the FIGO stage of patients. Data showed that proportion of Tim-3+CD4+ T cells in cases with high FIGO stages (III/IV) was 1.63-fold higher than those with low FIGO stages (5.51%±0.43% vs. 3.38%±0.63%, p=0.009) (Fig. 3A). Similarly, the expression of Tim-3+CD8+ T cells in cases with high FIGO stages (III/IV) was 1.70-fold higher than those with low FIGO stages (3.30%±0.36% vs. 1.94%±0.43%, p=0.037) (Fig. 3B). These data suggested that Tim-3 expression could be used as a marker for the progression of ovarian cancer.
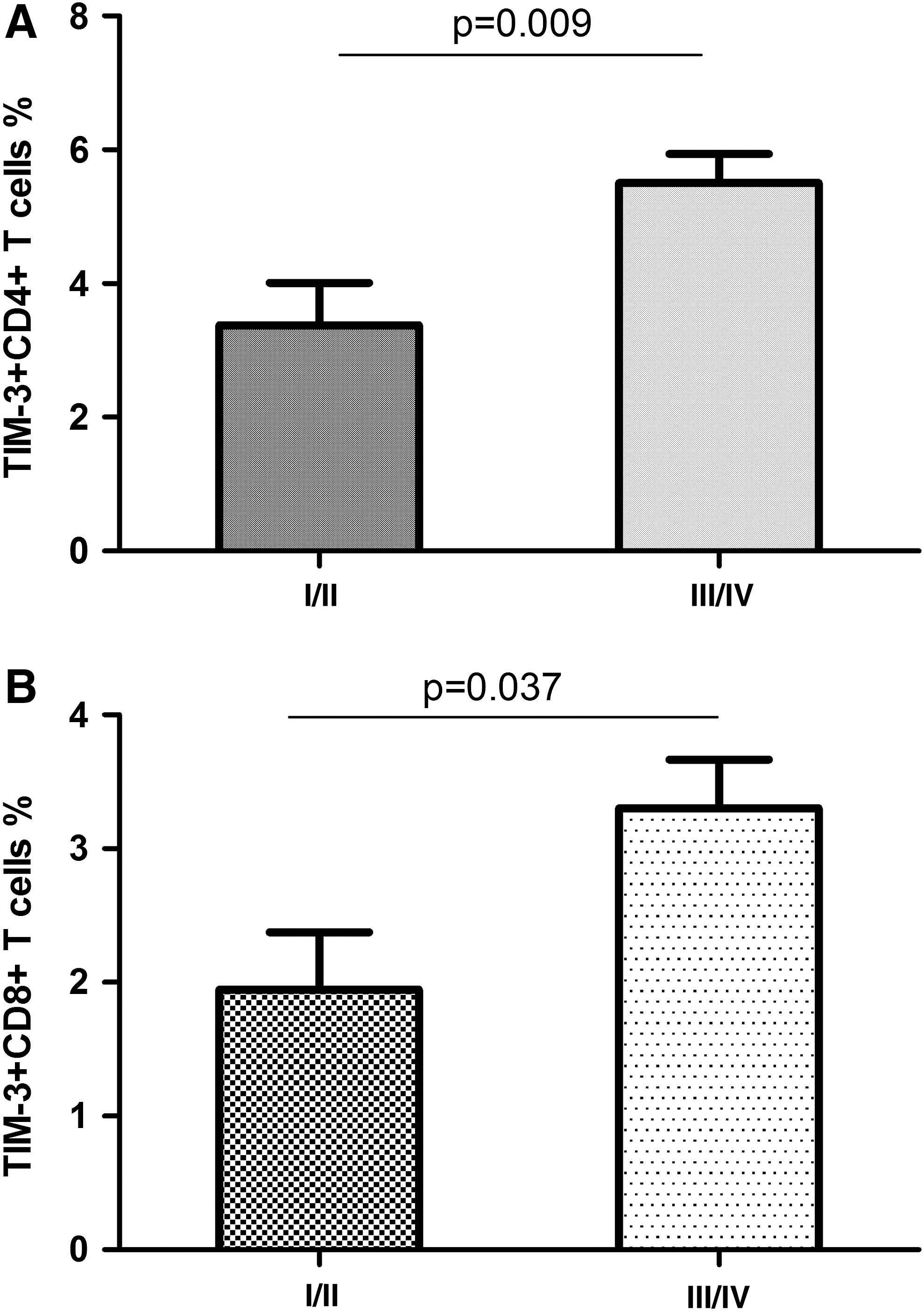
Comparison of Tim-3 expression on CD4+
Tim-3 expression on CD4+ and CD8+ T cells in patients with different tumor grades
Ovarian cancer patients with high tumor grade (G3) are undifferentiated and carry a worse prognosis. We compared Tim-3 expression on CD4+ and CD8+ T cells in patients with different tumor grades. Data showed that cases with high tumor grades had significantly higher proportion of Tim-3+CD4+ T cells than those with low tumor grades (5.39%±0.43% vs. 3.04%±0.52%, p=0.010) (Fig. 4A). Similarly, the expression of Tim-3+CD8+ T cells was also increased in patients with high tumor grades (3.22%±0.34% vs. 1.75%±0.49%, p=0.042) (Fig. 4B). These data suggested that Tim-3 expression could be used as a marker for the prognosis of ovarian cancer.
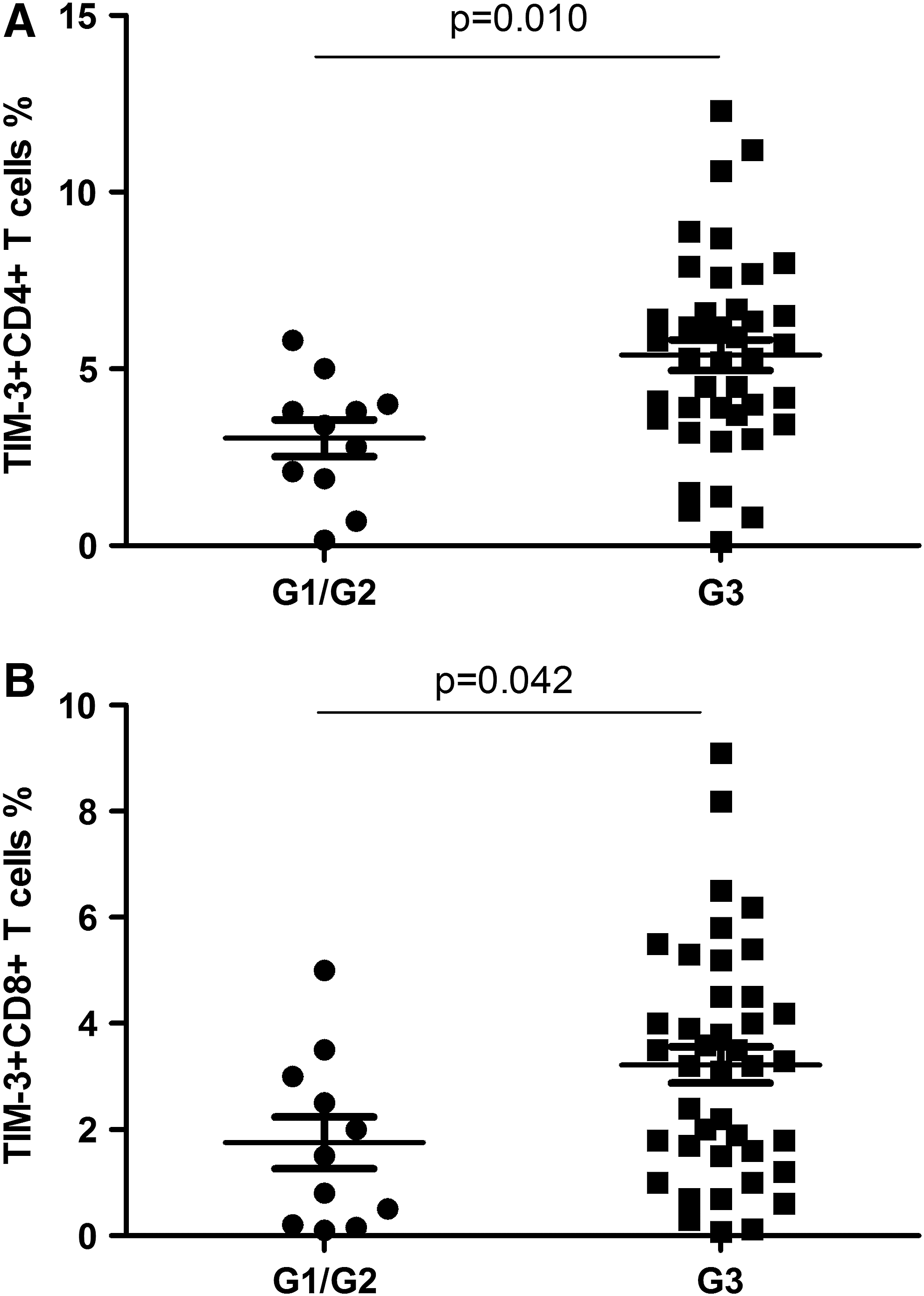
Comparison of Tim-3 expression on CD4+
Discussion
Tim-3 plays a pivotal role in immune regulation and immune tolerance. However, it is unknown whether Tim-3 is correlated with the pathogenesis of ovarian cancer. In this study, we examined Tim-3 expression on various immune cells in ovarian cancer patients and further explored its correlation with parameters of disease progression. Our data provided direct evidence for the first time that Tim-3 was involved in the development and progression of ovarian cancer by regulating CD4+ and CD8+ T-cell subsets.
The effect of Tim-3 on cancer is poorly understood. It is possible that Tim-3 plays a significant role in tumor progression by maintaining the tumor immunosuppressive environment through regulatory T cells (Tregs) (Monney et al., 2002; Nakayama et al., 2009; DeKruyff et al., 2010). A study has suggested that Tim-3+ Tregs in lung cancer tissues could be derived from natural Tregs upon chronic TCR stimulation by tumor antigens (Bai et al., 2013). PD-1 ligand B7-H1 and Tim-3 ligands such as galectin-9 and apoptotic cells within the tumor tissue might be important for maintaining the number and function of Tim-3+PD-1+ Tregs. In the transplantation setting, Tim-3 has been shown to regulate allospecific Treg activation (Chae et al., 2004a, 2004b; Bruck et al., 2008; Cao et al., 2010). It has been reported that the Tim-3-Tim-3L-sensitive pathway is involved in the functional generation of donor-specific Tregs upon administration of tolerizing treatments (Sabatos et al., 2003; Sanchez-Fueyo et al., 2003). Many different epithelial cancers are found to contain TILs, and T-cell infiltrates in particular are frequently associated with a favorable prognosis (Renesto et al., 2007; Nelson, 2008). Ovarian cancer is no exception, as a large number of studies have documented infiltration by both CD4+ and CD8+ T cells, as well as other leukocytes. TILs are strongly correlated with prognosis in ovarian cancer, with the balance of effector to regulatory T cells being a critical parameter. A recent study reported the lymphocytes isolated from the tumor tissues of ovarian carcinoma patients contained significantly greater proportion of Tim-3+ CD4+ T cells (Yan et al., 2013). Our study observed augmented Tim-3 expression on both CD4+ T-cell and CD8+ T-cell subsets (Fig. 1). However, further increase of Tim-3 was only identified on CD4+ T cells, but not CD8+ T cells in recurrent patients (Fig. 2B). These findings indicated that Tim-3 induced T-cell exhaustion may appear more frequently on CD4+ T cells in ovarian cancer, and suggested that Tim-3 may be used as a marker for the progression of the disease. Besides T cells, Tim-3 is important to regulate immune responses of NK cells, macrophages, and dendritic cells (Chiba et al., 2012; Ndhlovu et al., 2012). It is possible that Tim-3 expression on NK cells, macrophages, and dendritic cells might be correlated with the development and prognosis of ovarian cancer. Further studies on Tim-3 and these cells in ovarian cancer would be necessary.
Ovarian cancers are categorized by stages, depending upon how far they have spread beyond the ovary. The lower the stage number, the better the situation. Interestingly, a significant positive correlation was observed between FIGO stages and Tim-3 expression on CD4+ T cells and CD8+ T cells (Figs. 3). It is the first report showing surface marker on cells and can be associated with FIGO stages of ovarian cancer patients. In addition, biopsies that are taken from the ovary are also graded for how abnormal or ugly they look when viewed through a microscope. Ovarian cancers are given a grade from 1 to 3. Grade 1 represents cells that are more normal looking and therefore usually better behaved. Grade 3 cells look very abnormal, almost unrecognizable, which usually means the cancer is more aggressive. Our data demonstrated that cases with grade 3 had significantly higher proportion of Tim-3+CD4+ and Tim-3+CD8+T cells than those with grade 1 and grade 2 (Fig. 4). These results confirmed that peripheral blood immune cells may play a role in the development and progression of ovarian cancer.
In summary, the expression of Tim-3 is upregulated on CD4+ T and CD8+ T cells from PBMCs in ovarian cancer, in which Tim-3 is further increased in CD4+ T cells in recurrent patients. In addition, Tim-3 expression on CD4+ and CD8+ T cells is positively correlated with FIGO stages as well as tumor grades. Our data suggest that Tim-3 might be a potential diagnostic marker for the progression of ovarian cancer and might be as a therapeutic target for the treatment of this disease.
Footnotes
Disclosure Statement
No competing financial interests exist.