
Abstract
At present, severe acute respiratory syndrome coronavirus 2 is spreading and has caused over 188 million confirmed patients and more than 4,059,101 deaths. Currently, several clinical trials are done using mesenchymal stem cell (MSC) therapy in patients with coronavirus disease 2019 (COVID-19). These cells have shown safety and effectiveness, implying a promising clinical application in patients with COVID-19. Studies have shown that abnormalities in hematological measures such as white blood cells count, neutrophilia, elevated neutrophil to lymphocyte ratio, inflammatory markers, and lactate dehydrogenase can be used to assess the severity of COVID-19 disease and the response to therapy following MSC treatment. Our study has aimed to review the role of hematological factors in determination of responsiveness to MSC therapy and disease severity in COVID-19 patients.
Introduction
Coronaviruses (CoVs) belong to the family of Coronaviridae, the order Nidovirales, and the genus Coronavirus. During the 21 century, CoVs caused two important outbreaks, including severe acute respiratory syndrome coronavirus 1 (SARS-CoV-1) in 2002 (Bosch et al., 2004) and Middle East respiratory syndrome coronavirus in 2012 (Golchin et al., 2020). Human coronavirus (HCoV)229E, HCoVOC43, HCoVNL63, and human coronaviruses U1 (HKU1) are other HCoVs that have been identified so far (Zhu et al., 2020). HCoVs can transfer from person to person through aerosols and direct/indirect contact (Mohamadian et al., 2021). A novel member of the HCoVs, subsequently called “severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)”, has emerged in Wuhan, Hubei Province, China, in December 2019. The World Health Organization (WHO) named the new disease Coronavirus disease 2019 (COVID-19) and announced it as a global pandemic in March 2020 (Kooshkaki et al., 2020).
COVID-19 is characterized by distinct medical signs and symptoms such as high fever, chills, cough, shortness of breath, trouble in breathing, and finally death in severe cases (Golchin et al., 2020; Alsharif and Qurashi 2021; Taleghani and Taghipour 2021). The WHO has recorded 526,876,304 confirmed cases, 6,299,321 fatalities, and 496,689,236 recovered COVID-19 patients globally as of May 22, 2022 (“World Meter Corona Virus Update (Live)” 2021; Majumder and Minko, 2021). In terms of diagnosis, real-time PCR (RT-PCR) assay is the main molecular test for COVID-19, while antibody-based techniques serve as supplementary tools (Tang et al., 2020b). Recently, the use of mesenchymal stem cells (MSCs) as a treatment has piqued the interest of patients with COVID-19. Several indicators can be utilized to predict clinical response to MSCs based on the current findings.
Abnormalities in hematological measures such as white blood cells (WBC) count, neutrophilia, increased neutrophil to lymphocyte ratio, inflammatory markers, and lactate dehydrogenase (LDH) have been shown in studies to assess the severity of COVID-19 illness and response to therapy following MSC treatment. Our study has aimed to review the role of hematological factors in determination of responsiveness to MSC therapy and disease severity.
The Immune System Response in COVID-19
SARS-CoV2 infection and the covid-19 disease can be divided into three phases: (1) an asymptomatic phase with or without detectable virus; (2) a nonsevere symptomatic phase with upper airway involvement; and (3) a severe, potentially lethal disease with hypoxia, in the lung and progression to acute respiratory distress syndrome (ARDS) with high viral load (Nile et al., 2020). Clinical information shows that death in COVID-19 patients often results from a process called a cytokine storm in ARDS. Cytokine storm is the hyperproduction of cytokines that are associated with alveolar injury, vascular barrier damage, capillary damage, diffuse alveolar damage, multiorgan failure, and eventually death (Shimizu, 2019; Wang et al., 2020c).
Studies showed higher plasma levels of proinflammatory cytokines (tumor necrosis factor alpha [TNF-α], interleukin 1 beta [IL-1β], IL-1 receptor antagonist [IL-1RA], IL-6), monocyte chemoattractant protein-1 (MCP-1), macrophage inflammatory protein (MIP)-1A, granulocyte-colony stimulating factor (G-CSF), IL-7, and interferon gamma (IFN-γ) in patients infected with SARS-CoV-2, compared with controls (Jayaramayya et al., 2020). Hyperproduction of cytokines leads to an influx of various immune cells, including macrophages, neutrophils, and T cells from the circulation into the site of infection with destructive effects on human tissues (Fajgenbaum and June, 2020). The effective balance maintained by innate and adaptive immunity is vital for preventing the progression of COVID-19. SARS-CoV-2 has structural (such as S protein and nucleocapsid) and nonstructural proteins and the genome has nearly 80% similarity to the SARS-CoV-1.
SARS-CoV-2 via Spike proteins enter into host cells. In this process, angiotensin-converting enzyme 2 (ACE2) is a cellular receptor (Paces et al., 2020). The SARS-CoV-2 infection seems to trigger innate and adaptive immune system (Tang et al., 2005). Toll-like receptors (TLRs) recognize viral particles and eventually activate nuclear factor kappa (NF-ƙβ) pathways. The NF-ƙβ pathway leads to expression of inflammatory cytokines such as IL-6 and IFN-γ (Zu et al., 2020). Then, IFNs activate the Janus Kinase and Signal Transducer and Activator of Transcription pathways, which enhance the production of IFN-stimulating genes. SARS-CoV-2 inhibits the NF-ƙβ-TLR4 pathway, delay the IFN generation, and enable uncontrolled viral replication. Both proinflammatory and anti-inflammatory cytokines showed an upward trend in COVID-19 severe patients, suggesting that cytokine storms are linked to illness severity (Chen et al., 2020).
Zhou et al. (2020a) reported an increase in the total neutrophils, IL-6 serum levels, C-reactive protein (CRP) levels, and a reduction in the total lymphocytes in patients with COVID-19. Zheng et al. (2020) reported a significant decrease in the number of immune cells (Nk cells and T cells), an increase in the stimulation of remaining T cells, and exhaustive T cells in patients with severe COVID-19 compared to those with moderate illness. In addition, Moore and June (2020) found a significant increase in plasma levels of IFN-γ, (MCP)-1, and TNF that were associated with COVID-19 severity. Despite innate immunity, neutralizing antibodies, CD4+, and CD8+ T cells are able to control and suppress viral infection, but the functions and relevance of each component of adaptive immunity vary depending on the virus.
Mazzoni et al. (2020) and Liang et al. (2020) showed a decrease in both CD4+ and CD8+ T cell counts in COVID-19 patients. However, Zhou et al. (2020b) reported a decrease in CD4+ but not CD8+ T cell numbers in patients with severe disease. Anft et al. (2020) and Thieme et al. (2020) reported a stronger response of CD4+ compared to CD8+ cells to S protein and membrane and nucleocapsid proteins of SARS-CoV-2.
Mesenchymal Stem Cells
MSCs are multipotent cells that have self-renewal ability and can differentiate into several cell types (including chondrocytes and hepatocytes). They are applied in cell therapy and tissue engineering (Mishra et al., 2020). They can be extracted from different sources such as the bone marrow and umbilical cord, are easy to isolate, and may be useful in the treatment of a variety of illnesses such as myocardial infarction and meniscus damage (Lazarus et al., 1995; Fung et al., 2017; Li and Hua 2017; Lin et al., 2019). In 1966, MSCs were recognized by Friedenstein et al. (1966) and Caplan et al. (1991), who created the term MSCs in 1991. Although MSCs were initially discovered in bone marrow, they may also be derived from adipose tissue, peripheral blood, lung, synovial fluids, umbilical cord, and cord blood (Samsonraj et al., 2017).
MSCs inhibit the immune system by a variety of mechanisms, including growth factors, exosomes, cytokines, and apoptosis. The exact mechanism of the immunomodulatory function of MSCs is unclear, but researchers believe that these cells contribute to a balanced inflammatory and regenerative microenvironment in the presence of vigorous inflammation (Shi et al., 2018). Also, MSCs have the ability to interact with innate and adaptive immune systems, modulating several effector activities and induce peripheral tolerance. They can migrate to damaged tissues, inhibit inflammatory responses, and enhance the survival of damaged cells (Uccelli et al., 2008). Furthermore, they did not show any life-threatening adverse effects in several clinical trials to date (Golchin et al., 2020). SARS-CoV-2 infection may lead to overproduction of immune response, resulting in cytokine storm. MSCs through their immunomodulatory properties can inhibit cytokine storm and enhance endogenous healing (Mehta et al., 2020).
The infusion of haploidentical bone marrow mesenchymal stem cell in a patient with acute graft versus host-disease was the first clinical use of MSCs for immune/inflammatory disease in 2004 (Le Blanc et al., 2004). Afterward, the increasing amount of trials focused on the immunomodulatory characteristics of MSCs in clinical application. Recent studies showed that MSC immunomodulation may be particularly useful in attenuating the cytokine storm of patients with COVID-19 (Sanders et al., 2020). MSC-mediated immunomodulation runs through operative changes in Macrophages cells, dendritic cells (DCs), T cells (especially Tregs), B cells, and NK cells (Ren et al., 2008). MSCs exert their immunomodulatory roles by cell-cell contact with immune cells. For example, it has been proved that MSCs interaction with macrophages and Tregs lead to development of MSC-secreted cytokines.
Moreover, MSCs can trigger Tregs proliferation through Transforming growth factor beta 1 (TGFβ1), prevent the proliferation of neutrophils via IL-6 production, inhibit the antigen presentation of DC cells and T cells by prostaglandin E2 (PGE2) secretion, and inhibit proliferation and cytotoxicity of NK cells (Gao et al., 2016). In addition, MSCs via degrading T helper type 1 (Th1) and Th17 activation can attenuate T cell proliferation and induce allogeneic T cell tolerance and escape from Cytotoxic T lymphocytes and NK cells (Yadav et al., 2020). These cells have not expressed human leukocyte antigen class II and costimulatory molecules (B71, CD40L, and B72), so they can escape from immune recognition (Majumdar et al., 2003).
MSC Therapy in Patients with COVID-19 and the Changes in Hematologic and Immunologic Parameters
MSCs through their immunomodulatory, anti-inflammatory, self-regenerating, and antimicrobial activities can overcome the clinical challenges in COVID-19 patients (Durand et al., 2020; Sánchez-Guijo et al., 2020; Tang et al., 2020a; Wang et al., 2020b). Cell-based clinical trials using MSCs from variable sources like adipose tissue, umbilical cord blood, Wharton's jelly, and bone marrow—in the treatment of ARDS are undergoing. Indeed, some of the ongoing clinical trials have yet to submit their final reports (Table 1). MSC-based therapy showed a safe application in COVID-19, and most reports show low mortality and morbidity rates in COVID-19 patients. Lenng et al. was the first study to investigate whether MSC infusion could improve the outcome of seven enrolled patients with COVID-19 pneumonia in Beijing, China. In this clinical study, immune function and inflammatory status of patients were evaluated within 14 days after MSC injection.
Ongoing (Until September 18, 2021) Trials of Mesenchymal Stem Cell Therapy Against Coronavirus Disease 2019
BM-MSCs, bone marrow MSCs; CRP, C-reactive protein; FER, ferritin; IL, interleukin; LDH, lactate dehydrogenase; MSCs, mesenchymal stem cells; UCMSCs, umbilical cord MSCs; VEGF, vascular endothelial growth factor; WBC, white blood cells; XCEL-UMC-BETA, Intrathecal allogeneic cell therapy in a blinded syringe.
The symptoms of these patients were significantly improved and MSCs could significantly improve the functional outcomes without any significant adverse effects. Among them, two common and one severe patient were recovered and discharged in 10 days after treatment. After treatment, the peripheral lymphocytes were increased, the CRP and TNF-α significantly decreased, and the overactivated cytokine-secreting immune cells CXCR3+CD4+ T cells, CXCR3+CD8+ T cells, and CXCR3+ NK cells disappeared in 3–6 days. Thus, the result of this study showed that the intravenous transplantation of MSCs is safe and efficient for treatment in patients with COVID-19 pneumonia, especially for the patients in critically severe condition (Leng et al., 2020).
In another study, Liang et al. injected human umbilical cord MSCs (hUCMSCs) to a woman with COVID-19. In this study, human MSCs were successfully isolated from the umbilical cords of a healthy donor and injected to the patient 3 days apart. Injection of hUCMSCs markedly improved COVID-19 symptoms. Hematologic parameters, including bilirubin, CRP, ALT, and AST, lymphocyte, RBC counts, and hemoglobin gradually decreased after second injection. In addition, WBC counts, neutrophils, lymphocytes, and T subpopulation (TCD4+, TCD8+, TCD3+) levels returned to normal level as well. Although this study evaluated only one case, their result showed that hUCMSCs through inhibition of inflammation and modulation of immune system are possibly effective on the treatment of critically ill COVID-19 patient (Liang et al., 2020).
In this line, a case report by Zhang et al. evaluated hUCMSCs as a treatment for COVID-19 with serious symptoms. In this study, when treatment schemes such as antibiotics plus corticosteroids proved to be insufficient, hUCMSC therapy was prescribed. After cell therapy, there was a significant increase in lymphocyte counts and lymphocyte subsets (CD4+, CD8+, CD3+). Serum CRP levels gradually decreased and IL-6 and TNF-α returned to normal, indicating rapid recovery of the patient. After 2 days hUCMSCs transplantation, pulmonary functions and symptoms significantly improved and the patient was discharged 7 days later.
This study showed that hUCMSCs could reduce the cytokine storm in the critically ill COVID-19 patient (Wang et al., 2020a). Probably there is a direct interaction between MSCs with immune cells. Immune system modulate the proliferation and activation of effector T cells and NK cells by releasing anti-inflammatory factors such as IL-10, IL-1RA, TGF-β, indoleamine 2,3 dioxygenase, and nitric oxide. Moreover, MSCs inhibit the response of Th17, induce regulatory T cells (Treg cells), and shift Th1 cells to a Th2 cell phenotype (Chow et al., 2020).
Furthermore, Lange et al. showed that intravenous injection of MSCs improved clinical outcomes and increased peripheral lymphocytes and decreased CRP levels in COVID-19 patients. The treatment group received a dose of intravenous injection of MSCs, which clinical outcomes and inflammatory response were assessed for 14 days. After 14 days, all of patients were recovered in the treatment group while only one patient recovered in the control group. After 5 days of MSCs therapy, peripheral lymphocyte and IL-10 levels were increased, and TNF-α levels were decreased in the treatment group compared with the control group. In this study, after treatment, the CRP, CXCR3+CD4+ T cells, CXCR3+CD8+ T cells, and CXCR3+ NK cells and CD14+CD11c+CD11bmid regulatory DC cell disappeared in 3–6 days (Leng et al., 2020).
Moreover, Tang et al. evaluated routine blood tests, oxygen indicators, inflammatory markers, immunity markers, and coagulation function in severe COVID-19 patients before and after MSCs therapy. They used menstrual blood-derived MSCs for the treatment of two patients with severe COVID-19. Mortality, length of hospital stay, and need for ventilation after MSC infusion were primary endpoints. The blood routine examination, liver function, immune indicator, and inflammation indicator were the secondary endpoints. Before MSC therapy, CRP and IL-6 levels and WBC count, showed a strong correlation with the severity of COVID-19. After MSC and antiviral treatment, the lymphocytes increased, the inflammation indicators (CRP and IL-6) were decreased, and the symptom of dyspnea alleviated. After 3 days of the MSC therapy, the symptoms of shortness of breath were improved, and routine blood tests such as neutrophil counts and platelet counts returned to normal range.
Furthermore, inflammatory markers were decreased in COVID-19 patients (Tang et al., 2020a). However, this study has some limitations, including small sample size and lack of evaluation of long-term efficacy of MSCs for COVID-19.
In another study, Shu et al., randomly divided COVID-19 patients into two groups: control group (n = 29) and treatment group (n = 12). Controls received standard treatment, including oxygen supplementation, antiviral agents, antibiotic agents (moxifloxacin), and glucocorticoids. The treatment group received intravenous injections of hUC-MSCs. In the treatment group, all patients recovered and were discharged. Moreover, in the treatment group, the levels of inflammatory factors, including IL-6 and CRP, rapidly decreased.
This study suggested that MSC therapy can suppress excessive immune system activation and promote endogenous repair by improving the microenvironment. MSCs can enter the human body by intravenous infusion, and then some MSCs accumulate in the lungs, which can improve the lung microenvironment, protect alveolar epithelial cells, prevent pulmonary fibrosis, and improve lung function. However, the sample size of this study was not large enough to stratify subgroups, and some bias was difficult to exclude (Shu et al., 2020).
Feng et al. studied the efficacy of UC-MSCs in 16 patients with COVID-19 (nine critical and seven severe). All patients received four doses of UC-MSCs in addition to standard treatment, and the side effects and oxygen index were recorded. Levels of oxygenation, inflammatory markers, radiological presentation of the disease, and the number of lymphocyte subsets were recorded on days 7, 14, and 28. COVID-19 patients often experienced a significant decrease in lymphocyte counts (CD4 and CD8 T cells). After UC-MSC injection, severe patients showed a decrease in the levels of IL-10 and IFN-γ as inflammatory cytokine.
Furthermore, the number of lymphocytes increased after transplantation, indicating the immune-modulating effect of the MSCs effect in COVID -19. In this study, no MSC-related adverse event or allergic reactions were observed. Also, no delayed hypersensitivity or secondary infections were detected, suggesting safety and efficacy of MSCs in COVID -19. This trial lacked randomization, blinding, and comparison, had a small sample size, lost follow-up and plan deviation, and only 11 − 28% of their patients were positive for SARS-CoV2 by RT-PCR at baseline, which may influence the outcomes (Feng et al., 2020).
In another study, Sánchez-Guijo et al. infused adipose tissue-derived MSCs to 13 COVID-19 patients with severe condition undergoing aggressive mechanical ventilation. Ten patients received two doses, with the second dose administered a median of 3 days after the first one. Two patients received a single dose and another patient received three doses. Reduction in the CRP level, LDH, D-dimer, and ferritin (FER) were observed 6 days after injection with no adverse effect (Sánchez-Guijo et al., 2020).
In a phase 1 clinical trial, Meng et al. infused human UC-MSCs to nine COVID-19 patients in the treatment group. This group received three cycles of intravenous infusion of UC-MSCs on days 0, 3, and 6. This study also had a control group (n = 9) who received standard COVID-treatment. They evaluated laboratory tests, including CRP, ALT, IL-6 IFN-γ, TNF-α, MCP-1, IL-1RA, IL-18, and IL-8 levels, creatinine, SF, and platelets before and after UC-MSCs treatment at days 0, 3, and 7. Their results showed that almost all parameters improved in both groups within 14 days. In this study, the levels of IFN-γ, TNF-α, MCP-1, interferon-inducible cytokine IP-10, IL-22, IL-1RA, IL-18, IL-8, and macrophage inflammatory protein 1-alpha [MIP-1]) were decreased within 14 days.
Also, the levels of IL-6 were decreased within 3 days after UC-MSCs infusion, suggesting that the patients with high IL-6 might be more likely benefit from UC-MSC treatment. Their data showed that intravenous UC-MSCs infusion in patients with moderate and severe COVID-19 is safe and well tolerated (Meng et al., 2020).
In another double controlled trial, Adas et al. evaluated the efficacy of MSCs in critical patients with COVID-19. They divided 30 moderate and critical COVID-19 patients into three groups; group I (n = 10, moderate, treated with standard regimen), group II (n = 10, critical, treated with standard regimen), and group III (n = 10, critical, received three cycles of MSCs infusion on treatment days 0, 3, and 6). Based on the existing evidence, serum FER, fibrinogen, and CRP levels were all significantly decreased in group III compared with group II. These results showed the good efficacy of MSC therapy on critically ill COVID-19 patients (Adas et al., 2021).
Dilogo et al. showed that UC-MSCs, through modulating the immune system toward an anti-inflammatory state, could act as an adjuvant treatment for critically ill patients with COVID-19. They conducted a randomized controlled trial to investigate the application of UC-MSCs as adjuvant in the treatment of critical COVID-19 patients. This study included 40 critically ill patients with COVID-19; the treatment group (n = 20) received an intravenous infusion of 1 × 106/kg body weight UC-MSCs, and controls (n = 20) received 100 mL 0.9% saline solution. This study showed a significantly higher survival rate in the UC-MSCs group than in the control group (p < 0.05). There was no significant difference between D-dimer, fibrinogen, the complete blood count (hemoglobin, hematocrit, leukocyte, lymphocyte, and thrombocyte), procalcitonin, CRP, CD4−CXCR3, and FER between the MSCs group and the control group.
Furthermore, MSCs were better in suppressing lymphocyte subpopulations of CD8−CXCR3 and CD56−CXCR3 among critically ill subjects compared with controls, but this difference was not significant. Collectively, this study showed that MSCs are safe and well tolerated with no life-threatening complications or acute allergic reactions during the administration. However, the small sample size in this study holds up to acquire a statistically significant result, and they did not perform further supplementary tests to check for endotheliitis (Dilogo et al., 2021).
Saleh et al. conducted a phase I clinical trial to evaluate cell therapy with Wharton's jelly MSCs (WJ-MSCs) in patients with COVID-19. They enrolled five patients with severe COVID-19 and infused them three cycles of WJ-MSCs on days 0, 3, 6, and 14. After cell therapy with WJ-MSC, the percentage of lymphocytes, absolute lymphocyte count, and CD4 and CD8 T cell ratio increased, indicating the positive efficacy of these cells in immune system function. Moreover, among LDH, CRP, lymph count, and FER, only FER levels showed a significant decrease. Also, vascular endothelial growth factor, TGF-β, IFN-γ, IL-6, and TNFα decreased after 14 days of cell therapy (Saleh et al., 2021).
In a case series, Hashemian et al. evaluated the efficacy of MSCs derived from perinatal tissues in the treatment of severe phase of COVID-19. A total of 11 patients enrolled in this study and received UC-MSCs (n = 6) and the placental MSCs (PL-MSCs, n = 5) into three doses. Based on their results, a significant reduction in the serum levels of TNF-α, IL-8, and CRP was seen in all six survivors (Hashemian et al., 2021). Collectively, recent studies have shown the safety and efficacy of MSCs in alleviating COVID-19 symptoms. Thus, MSCs through their immunomodulatory features can decrease the inflammatory reactions, inhibit the cytokine storm, and decrease morbidity and mortality rates of COVID-19 (Fig. 1). In between, hematologic and immunologic parameters, including CRP, Procalcitonin Test, ESR, FER, and LDH, were all higher in patients with severe disease compared with normal patients, suggesting a more prominent inflammatory response in those patients.
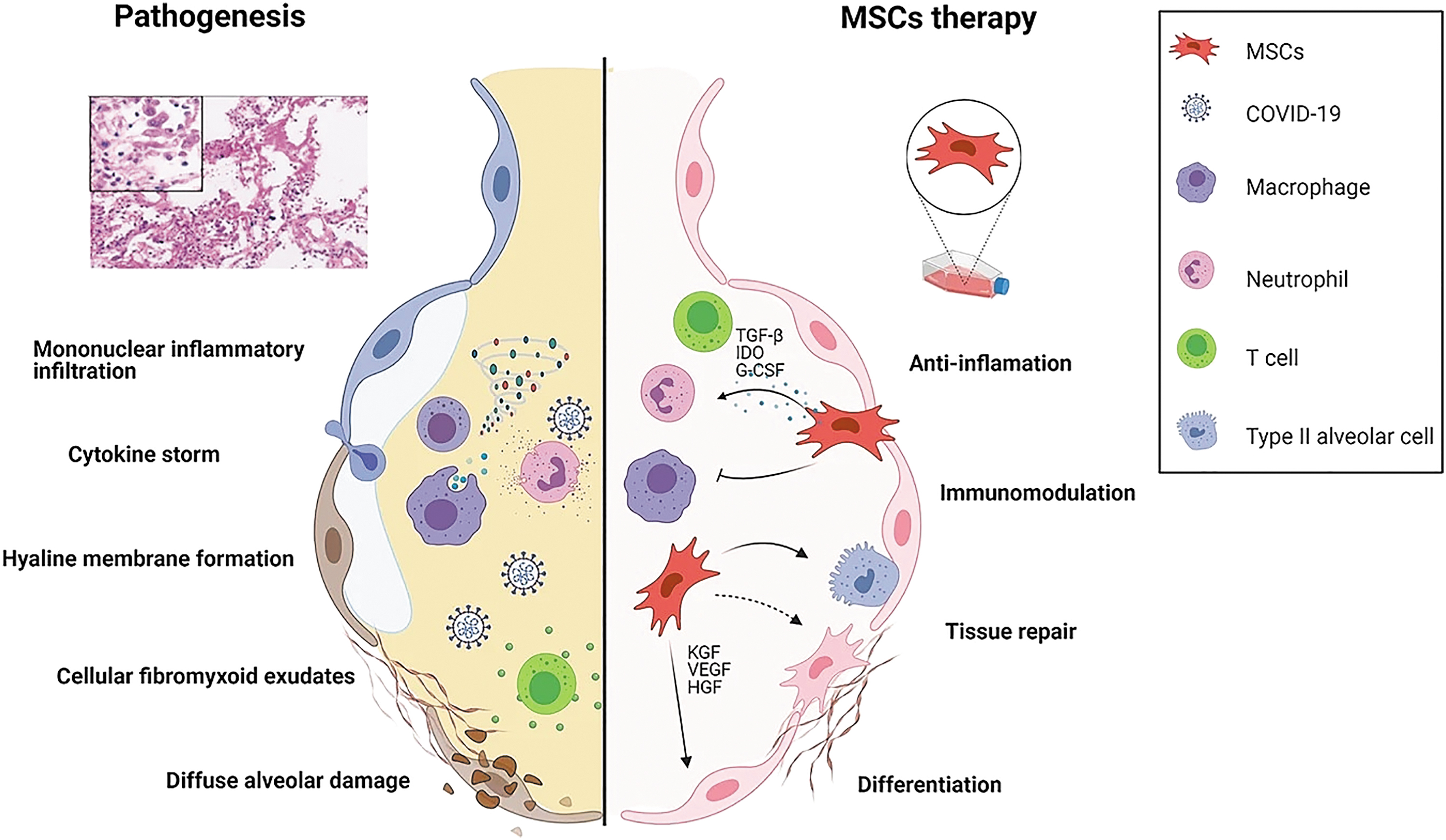
MSCs application in critically ill patients with COVID-19. Primarily, SARS-CoV-2 invade the respiratory tract. Then, we can see an increase in the infiltration of immune cells. Eventually, cytokine storms (including IFN-α, IL-1, IL-6, and TNF-α) occur. After the infusion of MSCs, the levels of inflammatory factors significantly decreased (Figure adopted from Shi et al. (2021)). COVID-19, coronavirus disease 2019; IFN-α, interferon alpha; IL, interleukin; MSCs, mesenchymal stem cells; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; TNF-α, tumor necrosis factor-alpha.
Moreover, we realized that lymphocyte counts and erythrocytes in COVID-19 patients with severe condition were decreased more than regular patients (Shi et al., 2021). Increased levels of inflammatory cytokines such as IL-6 and TNF-alpha were other associated findings that were more obvious in critically ill patients (Yuan et al., 2020).
Challenges for MSC-Based Therapy for COVID-19
MSC-based therapy against COVID-19 might be very effective during the pandemic. However, several immediate and urgent challenges have to be addressed for the development of the more safe and effective MSC-based approaches for COVID-19. The short-term fate of MSCs after intravenous injection is a key issue (Moll et al., 2012). The majority of therapeutic cells are placed in the lung after systemic MSC administration and they have a short life span. Only a small number of infused MSCs can circulate into other tissues. Even they may rapidly remove from the circulation in the lung, where they may also easily cause emboli. MSCs may lead to an innate immune response that may cause adverse events in COVID-19 patients who suffer from a hypercoagulopathy (Pasquarelli-do-Nascimento et al., 2020).
Thus, to avoid this, MSCs should be prescribed in a lower dose and cultured in a lower passage as a treatment. In addition, the humoral immunity (e.g., complements) and macrophages may clear MSCs from the body. It should be considered that the lung microenvironment can significantly change the beneficial effects of MSCs on ARDS after administration. For instance, Islam et al. (2019) showed that treatment of MSCs with plasma of ARDS patients led to a decrease in expression of CD105 and CD90 for 5 days, indicating a phenotype shift. Emerging data suggest that MSCs have an important role in drug resistance, especially in MSC therapy against cancer (Plava et al., 2019).
For instance, a preclinical study showed that bone-marrow-derived mononuclear cell from osteoporotic donors of ovariectomized (OVX) mice failed to prevent bone loss due to resistance to the disease microenvironment. This study emphasized the impact of the microenvironments on the clinical response of MSCs (Zheng et al., 2018). Last but not least, little is known about MSC homing to the sites of inflammation or injury in vivo, because cultured cells in vitro cannot mimic the natural cells (Karp and Leng Teo 2009). Unfortunately, MSC homing is inefficient, with only a small percentage of cells reaching the target tissue following systemic administration. After administration, MSCs must undergo several processes to exit circulation and migrate to the injury site (Sohni and Verfaillie 2013).
These homing processes can be divided into five steps: (1) tethering and rolling, (2) activation, (3) arrest, (4) transmigration or diapedesis, and (5) migration (Ullah et al., 2019). During serial MSC passaging, these cells might lose important receptors related to homing such as CXCR4. However, it is unclear which of these steps is the major bottleneck for MSC attrition and would thus be the most fruitful for further investigation. In conclusion, despite the significant development of the MSC-based therapy field, immunogenicity, limited homing, short life span, limited circulation into tissues, stimulation of unwanted innate immune response, different response in different microenvironments, possible involving in drug resistance, and inefficient MSC homing are the main limitations of this therapeutic approach that have not been solved yet.
COVID-19 and MSCs Clinical Trials
So far several clinical studies registered in
Cell Source and Trial Phase of Mesenchymal Stem Cell Clinical Trials for COVID-19
Conclusion
We conducted this narrative review to investigate the association between hematological and immunological abnormalities, as predictive factors of response to MSC therapy, in COVID-19 patients. At the beginning of the pandemic, COVID-19 was considered a respiratory infection. Later studies have shown that the virus can affect several organs of the human body, including cardiovascular, respiratory, gastrointestinal, nervous, and hematopoietic systems (Rahman et al., 2021). Patients with SARS-CoV-2 infection showed a plethora of hematologic conditions that are associated with disease severity and response to treatment (Copaescu et al., 2021). Based on evidence, COVID-19 significantly affects the hematopoietic system and is associated with leukopenia, lymphopenia, thrombocytopenia, and blood hypercoagulability (Terpos et al., 2020).
Furthermore, liver enzymes, LDH, CRP, troponin, and D-dimer showed significantly higher levels in patients with severe COVID-19 compared with controls and nonsevere patients (Ponti et al., 2020). Measured hematological factors dramatically improved the prediction of death and adverse events related to MSC therapy in COVID-19 patients. Studies found increased level of hemoglobin, RBC counts, lymphocytes, eosinophils, WBC counts, and neutrophils in critically ill patients than regular patients after MSC therapy. It can be concluded that treatment with MSCs decreases CRP levels, FER, and d-dimers in severe patients than controls. The diagnostic accuracy of hematologic parameters for COVID-19 is not significant due to low sensitivity and specificity, but are valuable prognostic indicators and provide some information about disease severity, disease course, and response to treatment (Khalid et al., 2021).
MSCs with their powerful immunomodulatory and regenerative abilities have the potential to overcome the cytokine storm and have been proposed as a potential therapeutic procedure for a group of COVID-19 patients with severe conditions. Based on the evidence, hematologic parameters can be considered as important factors in predicting response to MSC therapy. From our viewpoint, the timing of MSC injections in patients with severe COVID19 is critical. It seems that it is better to inject these cells in the inflammatory phase, and for this purpose, we should check inflammatory and hematopoietic markers for the patient before cell injection. Considering the behavior of MSCs, it seems that paying attention to the precise protocols of isolation, culture, proliferation, an appropriate number, manner, and time of proper injection into humans can be the beginning of a new treatment strategy in COVID19.
Further studies with a large sample size are needed to prove the effective outcomes of MSC therapy to indicate these significant differences. It is also necessary to increase the sample size and use randomization methods in further studies to indicate these cells' positive function and improve the disease.
Footnotes
Acknowledgment
The authors thank the Hematology and Cell Therapy of Tarbiat Modares University of Medical Sciences.
Authors Contribution
All authors read and confirmed the final version of article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.