
Abstract
Plasma cell-free DNA (cfDNA) was elevated in patients with acute myocardial infarction (AMI) or heart failure (HF). However, whether cfDNA could serve as a predictor for risk of HF after AMI remains unknown. In this study, we conducted a pilot prospective cohort study in which 98 AMI patients were enrolled from a single center to assess the association between cfDNA levels at admission and risk of HF in an AMI population. Patients with cfDNA above the median level (14.39 ng/mL) showed higher low-density lipoprotein cholesterol, cardiac troponin I (cTnI), and soluble suppression of tumorigenicity 2 (sST2) levels compared with patients below the median. cfDNA was positively correlated with cTnI (r = 0.377, p < 0.001) and sST2 (r = 0.443, p < 0.001). Within a median follow-up of about 345 days, 46 patients (52.6%) developed HF. Multivariate Cox analysis showed that a higher cfDNA (above the cutoff value: 9.227 ng/mL) was an effective risk predictor (C-index = 0.74, 95% confidence interval [CI]: 0.733–0.748) for HF incidence after AMI (adjusted hazard ratio [HR]: 2.805; 95% CI: 1.087–7.242; p = 0.033). Moreover, a linear association was observed between cfDNA and risk of HF incidence adjusted for by age, gender, and history of chronic kidney disease (p for linear trend = 0.044). Taken together, the cfDNA levels at admission are associated with the incidence of HF in AMI patients. A positive correlation between cfDNA and the fibrotic factor sST2 was proved, but the underlying mechanisms require further study.
Introduction
Cardiovascular disease (CVD) is the leading cause of death in the world, ∼17.9 million deaths annually accounting for 32% of all global mortality rates (Roth et al., 2018). Acute myocardial infarction (AMI) is the most serious manifestation of coronary artery disease. With lifestyle modification and the increasing use of evidence-based medications, the mortality rate of AMI has decreased considerably in recent decades (Puymirat et al., 2017). Nevertheless, the subsequent development of heart failure (HF) is still a common complication of AMI and has emerged as a remarkable cause of long-term adverse consequences and death. Earlier studies had reported that an incidence of HF during hospitalization for an AMI patient varied widely, reaching up to 50% (Hellermann et al., 2002). Even in the revascularization era, the overall rates of HF incidence after AMI remained in the range from 14% to 36%, suggesting that MI was still the most common cause of HF (Bahit et al., 2018).
According to the time of HF onset after AMI, HF can be defined as three different clinical types: HF onset at the time of MI presentation; HF developing during hospitalization for MI; and HF onset after discharge (Jenča et al., 2021). AMI with HF suffers high morbidity and poor prognosis. Evidences showed that the cardiovascular mortality rate was significantly increased fourfold in AMI patients with HF (Gerber et al., 2016). Specially, the mortality risk rate in AMI patients with delayed-onset HF (>3 days after AMI) was substantially higher than those with early-onset HF (≤3 days after AMI) (Gerber et al., 2016). Therefore, reducing discharge mortality rate and improving long-term survival of AMI patients are to be the new challenges in future. Since the time of HF development after AMI affects the optimal management and outcomes of the patients, early screening of high-risk population and prevention of HF development are of extraordinary importance.
Cell-free DNA (cfDNA) is a double-stranded DNA fragment existed in human plasma, urine, cerebrospinal fluid, and other body fluids, originating from apoptotic or necrotic cells (Teo et al., 2019; Papadopoulos, 2020). In recent years, cfDNA has received increasing attention as a damage-associated biomarker in the field of CVD (Bender et al., 2019; Benincasa et al., 2019; Sanchis et al., 2019; Devaux, 2020; Dong et al., 2020; Polina et al., 2020; Yokokawa et al., 2020; Salzano et al., 2021). Studies have reported that the level of cfDNA in AMI patients was significantly higher than that of healthy population and positively correlated with the levels of myocardial markers creatine kinase (CK) and cardiac troponin I (cTnI) (Shimony et al., 2010; Cui et al., 2013; Zemmour et al., 2018; Agiannitopoulos et al., 2020; Yokokawa et al., 2020).
Differing from the classic myocardial damage markers, plasma cfDNA could increase in the early stage of AMI (0–2 h after onset), and maintain elevation within 24 h (Chen et al., 2013; Polina et al., 2020). Especially, released mitochondrial DNA, as a component of plasma cfDNA, was immediately presented in blood at 1 h after onset of initial AMI symptoms, and reached a peak at about 3 h after onset, which was much earlier than the peak time of cTnI or cTnT (10–20 h after AMI)(Bliksoen et al., 2012). Due to its rapid changes, cfDNA was expected to be potential candidate marker for monitoring myocardial infarction.
Moreover, the latest study showed that cfDNA levels were marked higher in HF patients compared with healthy individuals, suggesting a potential of cfDNA to aid in HF diagnosis (Devaux, 2020; Yokokawa et al., 2020; Salzano et al., 2021). However, whether the released cfDNA during AMI would be able to predict the risk of HF incidence has not been well studied. In the present study, we conducted a pilot prospective cohort study to examine the association between plasma cfDNA levels at admission and the risk of HF among AMI patients during 1 year of follow-up.
Methods
Study design and participants
Patients with first-time AMI admitted to the Chest Pain Center of Hunan Provincial People's Hospital, Hunan, China, between June 2020 and December 2020 were recruited in this single-center study. All patients met the diagnostic criteria for AMI according to the Fourth Universal Definition of Myocardial Infarction (Thygesen et al., 2018). Primary percutaneous coronary intervention (PPCI) was performed for eligible patients according to the criteria for myocardial revascularization. The exclusion criteria are as follows: admitted more than 24 h after symptom onset, aged <18 years, presence of active infection including myocarditis and sepsis, stroke, active autoimmune disease, and malignant tumor. As a result of the exclusion of patients with these criteria, 98 patients were included in the study population (Supplementary Fig. S1).
According to the circulating cfDNA level at admission, the enrolled patients were divided into two cohorts as follows: low cfDNA and high cfDNA. The cohorts were followed up to November 25, 2021. Follow-up data were collected through telephone follow-up or patients' return visits to the out-patient clinic. HF was defined as a major adverse cardiovascular event in this study. We used the An et al., 2021 to adjudicate HF incidence in AMI patients. The study was approved by the Ethics Committee of Hunan Provincial People's Hospital ([2020]-41). All patients voluntarily entered the study and signed an informed consent form before their enrollment.
Collection of clinical and biochemical parameters
All data including detailed medical history and patient characteristics were extracted from electronic health records. The first measurements of N-terminal pro-B-type natriuretic peptide (NT-proBNP) and cTnI at admission were determined using the AQT90 FLEX analyzer (Radiometer Medical ApS, Bronshoj, Denmark) in the emergency department, and the results were obtained from clinical records. Circulating soluble suppression of tumorigenicity 2 (sST2) levels were determined using the QuantiCyto® Human ST2 ELISA kit (EHC043.96.2; NeoBioscience, China). Echocardiography was performed and analyzed blindly by a senior echocardiologist on the day after hospital admission.
Preparation and quantification of cfDNA
Blood samples were obtained from all enrolled patients within 24 h of onset and before PPCI. All samples in ethylene diamine tetraacetic acid (EDTA) collection tube were immediately placed on ice. Within 4 h after sample collection, plasma sample was separated by centrifuging twice at 1600 g for 10 min at 4°C, and followed by 16,000 g for 10 min at 4°C. The cfDNA in 1 mL plasma was extracted using the MagMAX™Cell-Free DNA isolation kit (A29319; Thermo Fisher Scientific, Inc.) and then stored at −80°C.
The quantification of cfDNA was carried out within the Qubit™ 4 Fluorometer (Thermo Fisher Scientific, Inc.). Each sample was detected using the Qubit 1 × dsDNA Assay Kits, high sensitivity (Q33231; Thermo Fisher Scientific, Inc.), according to the manufacturer's protocol.
Statistical analysis
SPSS software version 23.0 and R version 4.1.1 were used for statistical analysis in this study. All variables were first performed with the Kolmogorov–Smirnov test to assess normality. Continuous variables were presented as the mean ± standard deviation for variables with normal distribution and as the median (interquartile range [IQR]) for variables with non-normal distribution. Categorical variables were reported as numbers and percentages. According to the normality of variables distribution and homogeneity of variance, the analysis of variance (ANOVA) or the Mann–Whitney U test was used to compare the differences between two groups. Categorical data were compared with χ 2 test or Fisher's exact test.
The relationship between cfDNA and other variables was assessed via Spearman rank correlation analysis. Univariate and multivariate Cox proportional hazard regression analysis was performed to assess risk factors related to HF incidence after MI. The association between cfDNA levels and incidence of HF was evaluated by restricted cubic spline curves based on Cox proportional hazard. Receiver operating characteristic (ROC) analysis was used to determine the predictive efficiency of cfDNA, and statistical differences between curves were assessed via pROC package. Kaplan–Meier survival curves were used to illustrate events between both low cfDNA and high cfDNA cohorts. The data were visualized using R. p < 0.05 was considered statistically significant.
Results
Baseline characteristics of the study patients
After excluding inappropriate cases, a total of 98 enrolled patients were included in this study. The median estimated circulating cfDNA level in the overall study population was 14.39 ng/mL (IQR 9.42–23.02). Based on the median value, 49 patients were grouped as low cfDNA (≤14.39 ng/mL) and the remaining 49 patients constituted the high cfDNA group (>14.39 ng/mL). The baseline demographic and clinical characteristics are described in Table 1. There was no significant difference between the two groups on age, gender, and factors of medical history.
Baseline Characteristics of Acute Myocardial Infarction Patients with Plasma Cell-Free DNA Above and Below the Median
Values are mean ± SD, n (%), or median (IQR).
Others indicate septal or posterior or lateral MI.
ACEI, angiotensin converting enzyme inhibitors; BMI, body mass index; cfDNA, cell-free DNA; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; DBP, diastolic blood pressure; HR, hazard ratio; IQR, interquartile range; LAD, left anterior descending artery; LCx, left circumflex artery; LVEF, left ventricular ejection fraction; PPCI, primary percutaneous coronary intervention; RCA, right coronary artery; SBP, systolic blood pressure; STEMI, ST-elevation myocardial infarction; Time of D to W, door-to-wire crossing time; TIMI, thrombolysis in myocardial infarction; SD, standard deviation; WMSI, wall motion score index.
Circulating cfDNA level and sST2, cTnI
To further analyze the difference of study population in the two groups, a comparison of all biochemical parameters, including routine blood biochemistry, myocardial enzyme profile, and sST2, between the two cohorts was carried out. As shown in Supplementary Figure S2, the plasma low-density lipoprotein cholesterol, cTnI, and sST2 levels at admission were significantly higher in the high cfDNA group than in low cfDNA group. Correlation analysis further showed that cfDNA level was linearly related to cTnI (r = 0.377, p < 0.001; Fig. 1B) and sST2 (r = 0.443, p < 0.001; Fig. 1A) concentrations at admission.
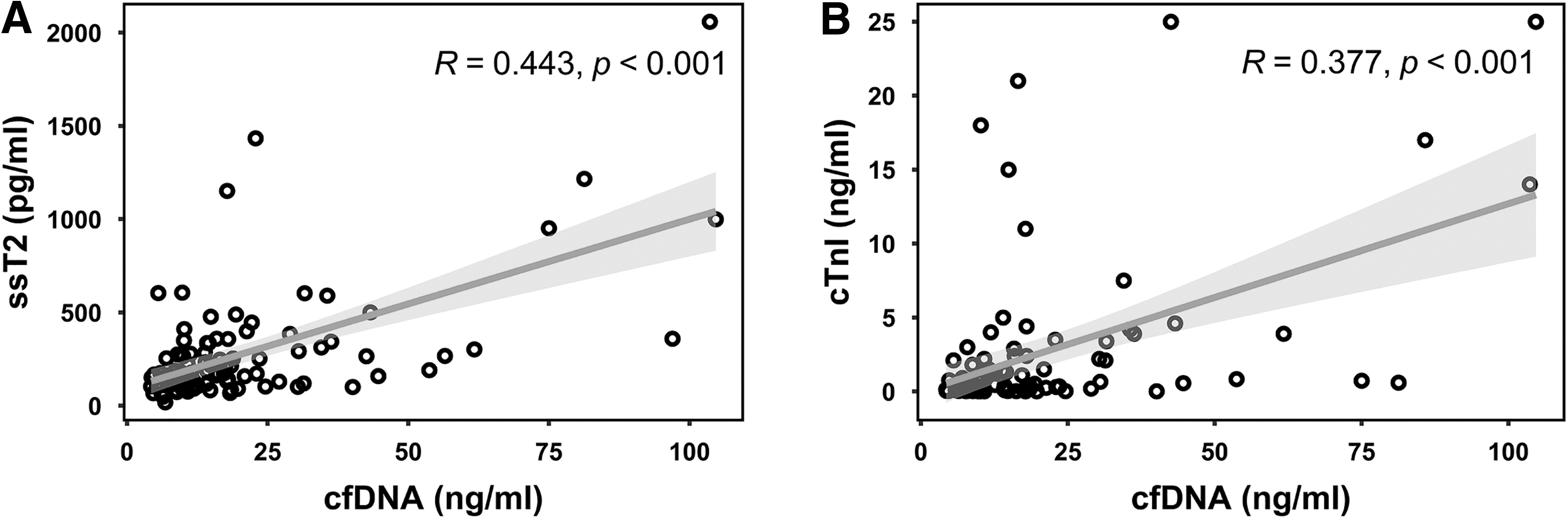
Correlation analysis of plasma cfDNA level and biomarkers at admission.
Circulating cfDNA level at admission and HF risk
In total, there were 46 patients (52.6%) who developed HF within a median follow-up of about 345 days in our study. No death was observed in this study during follow-up. Kaplan–Meier analysis showed a slightly higher probability of HF in AMI patients within the high cfDNA group than those within low cfDNA group (54.2% vs. 40.8%), but the difference was not statistically significant (p = 0.17, Supplementary Fig. S3).
Next, we performed ROC analysis of circulating NT-proBNP, sST2, and cfDNA concentrations at admission to discriminate the incidence of HF in AMI patients. As shown in Supplementary Figure S4, NT-proBNP displayed the largest area under the curve (AUC = 0.738; 95% confidence interval [CI]: 0.628–0.849; p < 0.001), followed by sST2 (AUC = 0.676; 95% CI: 0.571–0.782; p = 0.001) and cfDNA (AUC = 0.635; 95% CI: 0.525–0.746; p = 0.016). However, no significant difference was observed while comparing the discrimination power between cfDNA and NT-proBNP (p = 0.199), or between cfDNA and sST2 (p = 0.598) using the DeLong's test of the AUCs.
To exactly describe the association between circulating cfDNA levels at admission and HF risk, a Cox proportional hazards model was further used to estimate the relevant risk indicators of HF incidence after MI. The results of univariate and multivariate analyses of various parameters are presented in Table 2. In the univariate Cox regression model, variables including age, chronic kidney disease (CKD), wall motion score index (WMSI), numbers of affected vessels, Gensini score, myoglobin (MYO), NT-proBNP, as well as cfDNA were identified as risk factors of HF after AMI. Patients with each unit increase in cfDNA at admission had 1.2% more risk of HF (HR = 1.012; 95% CI: 1.001–1.023; p = 0.029).
Univariate and Multivariate Cox Regression Analysis for Potential Predictors of 1-Year Heart Failure After Myocardial Infarction
Bolded values indicate p-values <0.05.
The median value of cfDNA at admission. The reference was cfDNA <14.39 ng/mL.
The cutoff value of cfDNA at admission. The reference was cfDNA <9.227 ng/mL.
CI, confidential interval; CK-MBadm, creatine kinase-MB at admission; cTnIadm, cardiac troponin I at admission; Hb, hemoglobin; HR, hazard ratio; MYOadm, myoglobin at admission; NT-proBNPadm, N-terminal pro-B-type natriuretic peptide at admission; sST2adm, soluble suppression of tumorigenicity 2 at admission.
However, while adjusted for age, CKD, WMSI, numbers of affected vessels, and Gensini score, the cfDNA level at admission was not shown as an independent risk factor for HF incidence (adjusted HR = 1.003; 95% CI: 0.991–1.015; p = 0.659). Surprisingly, the WMSI was an independent risk factor for HF, and the increase of every additional unit of WMSI indicated a 3.5-fold risk of HF according to the multivariate Cox regression model I (adjusted HR = 3.502; 95% CI: 1.551–7.905; p = 0.003).
Since the ROC analysis showed that the cutoff value of cfDNA to identify HF incidence was 9.227 ng/mL, a further Kaplan–Meier analysis showed a remarkably increasing incidence of HF in AMI patients with a concentration of cfDNA above 9.227 ng/mL (p = 0.0037, Fig. 2). Moreover, the significance of risk prediction remained for cfDNA after stratification based on the cutoff value of 9.227 ng/mL (HR = 3.232; 95% CI: 1.274–8.199; p = 0.014), but not on the median value of 14.39 ng/mL (Table 2).
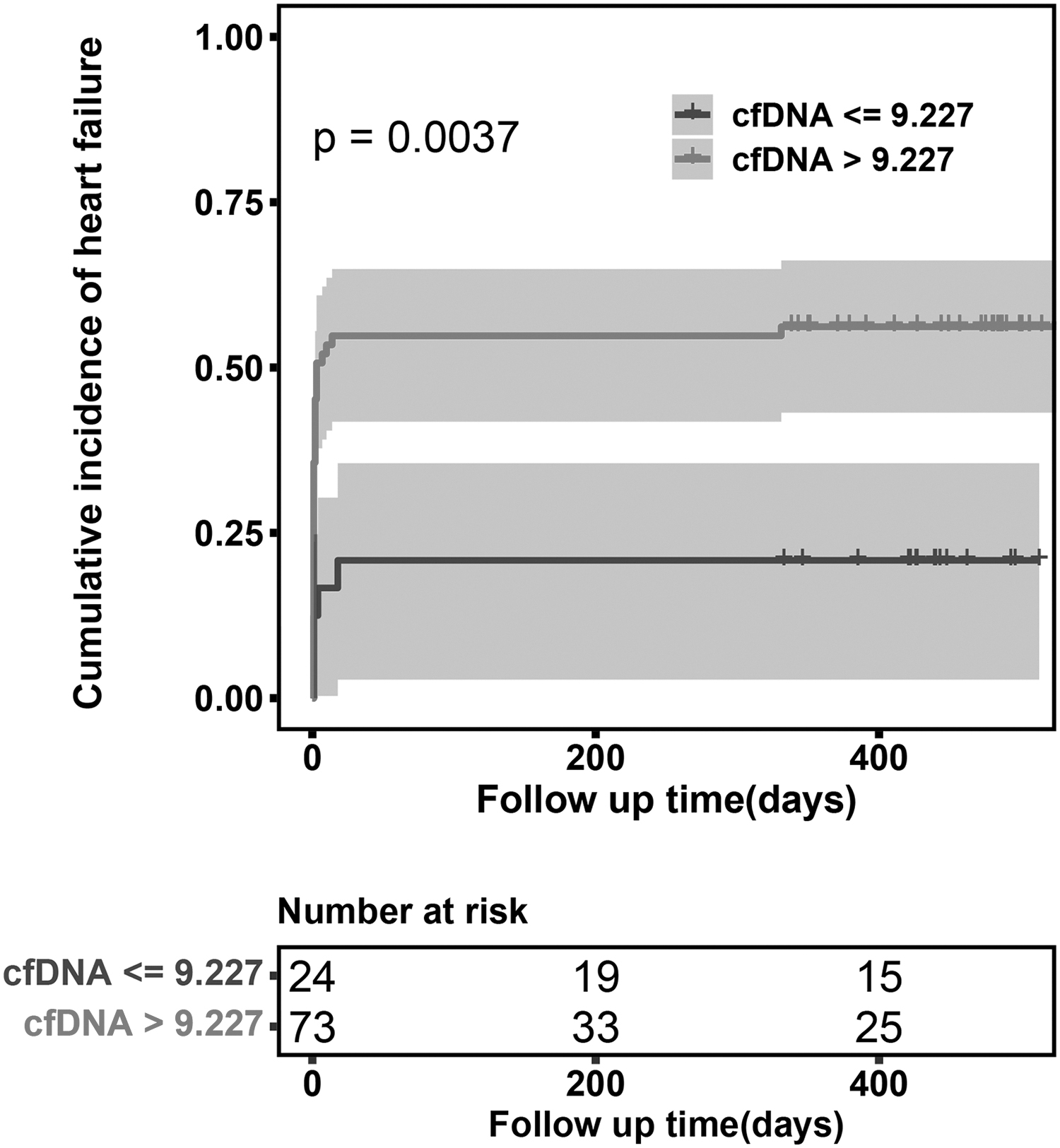
Kaplan–Meier analysis showing the incidence ratios of HF after AMI according to the level of cfDNA at admission. AMI, acute myocardial infarction; HF, heart failure.
Even in model II adjusted for age, CKD, numbers of affected vessels, and Gensini score, the risk of HF was ∼2.8 times higher in patients with cfDNA levels above the cutoff value (adjusted HR = 2.805; 95% CI: 1.087–7.242; p = 0.033). Meanwhile, the model II showed a moderate prediction accuracy in the primary cohort (C-index = 0.74, 95% CI: 0.733–0.748). However, we found no difference in predictive power between cfDNA and other myocardial injury biomarkers, including MYO, cTnI, and creatine kinase-MB (Supplementary Fig. S5).
In addition, we used restricted cubic spline analysis to visualize the relationship between circulating cfDNA levels and the HR of HF incidence after AMI, and found a linear association between cfDNA and the risk of HF (p for linear trend = 0.050, Fig. 3A). Above 14.39 ng/mL, a rising of cfDNA level was accompanied by increasing risk of HF incidence. This trend was also observed after adjustment for age, gender, and CKD (p for linear trend = 0.044, Fig. 3B). Nevertheless, while adjusted for age, CKD, WMSI, numbers of affected vessels, and Gensini score, the HR of incident HF was gradually dropped after a threshold of cfDNA >50 ng/mL (Fig. 3C).

Restricted cubic spline analysis showing the association between plasma cfDNA level at admission and the risk of HF after AMI.
Discussion
In this study, we first evaluated the potential association between circulating cfDNA levels at admission and the risk of HF incidence after AMI. Our results showed that the concentration of plasma cfDNA at admission was associated with increased risk of HF in a 1-year follow-up for AMI patients who had received early successful PPCI and guideline-based therapies, even after adjustment for age, CKD, numbers of affected vessels, and Gensini score. Besides, we found that the elevation of cfDNA was positively correlated to plasma sST2 concentration, which has been included as a biomarker for myocardial fibrosis, suggesting an underlying pathway by which cfDNA released from a damaged myocardium may affect cardiac remodeling and promote HF development. Our study provides a new insight that early monitoring of plasma cfDNA levels in AMI patients may become a strategy to predict the risk of HF incidence.
Previous investigators had shown that plasma cfDNA level was rapidly increased in the very early stage of AMI (0–2 h after onset of a chest pain), suggesting that cfDNA might be a potential new biomarker for acute coronary syndromes (Chen et al., 2013; Polina et al., 2020). In this study, we found that a significantly higher level of myocardial marker cTnI was presented in patients with a circulating cfDNA level above 14.39 ng/mL at admission, and observed a significant linear correlation between cfDNA and cTnI, which were consistent with previous findings (Shimony et al., 2010; Cui et al., 2013; Zemmour et al., 2018; Yokokawa et al., 2020).
Interestingly, the results of this study extended the above observations and showed that the cfDNA concentration was positively related to the plasma sST2 level. Interleukin 33 (IL-33) is a cytokine belonging to the IL-1 superfamily, which had been confirmed as a cardioprotective factor to prevent myocardial fibrosis and cardiomyocyte hypertrophy (Ghali et al., 2018). ST2 as a receptor of IL-33 is universally expressed in various immune cells as well as cardiomyocytes and has two main isoforms: the transmembrane ST2 isoform (ST2L) and the soluble ST2 (sST2) (Ghali et al., 2018). A series of studies suggested that a secreted sST2 isoform could act as a decoy receptor of IL-33 to block IL-33-ST2L axis mediated against myocardial remodeling, and that sST2 was emerged as a novel cardiac biomarker for the diagnosis and prognosis of HF (Somuncu et al., 2020; Jenča et al., 2021).
Our results indicate a potential association between cfDNA and myocardial remodeling after infarction. However, the mechanism by which sST2 is increased in AMI patients with high cfDNA remains unknown in this study. Extracellular DNA was originally considered a waste molecule passively produced under pathological conditions and temporarily retained in body fluids (Kustanovich et al., 2019). Recently, some studies have reported that cfDNA could work as a damage-associated molecular pattern to promote secretion of proinflammatory cytokines via binding to Toll-like receptor 9 (Liang et al., 2018). Therefore, whether cfDNA can trigger the expression and secretion of sST2 during myocardial infarction still needs to be further investigated.
The assessment of WMSI provides a scoring system to directly quantify the intensity and extent of the myocardial damage and systolic function in an AMI patient, in which higher scores implicate the incidence of more serious myocardial damage and a worse outcome in patients (Dall'Armellina et al., 2008; Jurado-Román et al., 2019). Consistently, our results here revealed that WMSI is an independent risk factor for HF after AMI. Several studies have reported that the cardiomyocyte-specific cfDNA was increased in HF patients and associated with mortality rate in patients (Yokokawa et al., 2020; Salzano et al., 2021). Considering that cfDNA is similarly a marker of myocardial damage, we therefore exclude WMSI from the confounding factors while establishing the Cox regression model.
As shown in our results, the present study provided evidence on the performance of using the cfDNA level at admission to predict the incident risk of HF and indicated a higher risk of HF in AMI patients with a concentration of cfDNA above 9.227 ng/mL.
The present analysis has several limitations that merit emphasis. First, the participants enrolled in the cohort are all from a single center, and the small sample size of the cohort makes us fail to incorporate more confounding factors into a model and to further validate the model. Therefore, to be completely and widely representable in the AMI population, the findings, including the cutoff value as well as the prediction performance of cfDNA, obtained in our study need to be confirmed in a multicenter and larger sample-sized study in future. Second, the overall incidence of HF in AMI patients is higher in our study than previous reports (Bahit et al., 2018), which may be attributed to the selection bias caused by the elimination of samples with hemolysis or incomplete clinical information, although it is random.
In conclusion, high levels of cfDNA at admission are an important predictor of HF incidence during the 1-year follow-up in AMI patients. Besides, there is a significant correlation between plasma cfDNA and fibrotic factor sST2 within patients, which raises an important question that is yet to be answered, whether cfDNA could regulate sST2 expression and myocardial remodeling during the progression of HF development after AMI.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by grants from the Key Research and Development Program of Hunan Province (2019SK2021), the Scientific Research Project of Hunan Health Commission (202203013494), and the Science and Technology Innovation Program of Hunan Province (2018SK50711).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.