
Abstract
Abstract
In the United States, the voting right of persons who live in long-term care facilities has not received adequate attention. Residents can lose one of their most cherished rights and electoral credibility can be corrupted. One solution to the problems of voting in long-term care is mobile polling, a process whereby election officials bring the ballot to residents of long-term care facilities, provide voters assistance when needed, and register voters as well. This study compared mobile polling to voting as usual in selected nursing homes in the State of Vermont during the U.S. 2008 general election. Results show that among election officials and nursing homes willing to try mobile polling, it is feasible and generally well accepted by long-term care staff, residents, and election officials; reduces concerns of voter fraud and manipulation; and enhances residents' dignity and rights. The challenges of mobile polling include motivating and training election officials to perform it, providing resources to staff the homes, assuring voter privacy, and obtaining the names of the residents of long-term care facilities in order to assess the proportion of residents who voted. Features of a state or election precinct that can successfully adopt mobile polling include the ability to conduct early voting, access to paper ballots, long-term care facilities which are willing to participate, and a good relationship between the chief election administrator and election officials.
Residents of long-term care facilities, such as nursing homes and assisted living, typically have physical and cognitive impairments that limit their ability to independently register to vote and to cast a vote. For example, in nursing homes where election officials do not provide guidelines or assistance, most residents vote using an absentee ballot. They need assistance in completing this ballot, and facility staff provide most of this assistance. 3
These practices create problems. A facility's staff members may make decisions that can inappropriately limit voter access. For example, they may decide which residents can vote and how best to assist a disabled voter. Staff can also engage in voter fraud.7–9 In short, the absence of election officials assisting with voting means that residents can lose one of their most cherished rights and electoral credibility can be corrupted.
The failure to address the problems of voting in long-term care will only increase these consequences. One million five hundred thousand persons in the United States live in nursing homes, 10 and the United States, like most developed nations, is experiencing a rapid growth in the portion of the population over 65. An estimated 44% of older adults will enter a nursing home before they die, and 23% of these persons will spend at least one year in a nursing home. 11 Many residents have at least mild degrees of cognitive impairment. 12 In addition, not only local but also national elections may be decided by slim margins. Nursing homes thus can become the foci of accusations of voter fraud and exploitation.
Fortunately, in the last several years, federal and state officials have paid increasing attention to improving voter access and limiting voter fraud in long-term care. 6 Federal civil rights laws—most notably the Voting Rights Act of 1965, 13 Title II of the Americans with Disabilities Act, 14 the Voting Accessibility for the Elderly and Handicapped Act of 1984, 15 and the Help American Vote Act of 2002 16 —all require state and federal governments to take steps to remove accessibility barriers to voting by persons with disabilities. Yet the extent to which these mandates apply beyond the obvious disability barriers, such as physical inaccessibility or the right to have someone assist with voting, is difficult to specify.
States have made some accommodations for voting in long-term care, but many of these procedures are quite limited in the degree of involvement that election officials have in voter registration and absentee balloting.6,17 A better solution to the problems of voting in long-term care is a technique called mobile polling.
Mobile polling is a process whereby election officials bring the ballot to residents of long-term care facilities, provide voters assistance when needed, and, where legislative deadlines permit, register voters as well. 18 In some nations, such as Australia, mobile polling is the norm. By placing voting in the hands of skilled, trained, and non-partisan election officials, mobile polling has substantial promise to maximize access and minimize fraud.
Unfortunately, mobile polling is not widely practiced in the United States. In 2007, the American Bar Association (ABA) issued recommendations to address the challenges of voting by older adults with cognitive impairments. 19 These recommendations included the need for research on voting practices in long-term care settings. 20 The purpose of this study was to identify the advantages and challenges of mobile polling, one of the recommended practices, so as to facilitate wider adoption of the practice in the United States.
This study addressed the following questions: What are the benefits of mobile polling? What are its challenges? What resources are needed to accomplish mobile polling? What is the impact of mobile polling on voting rates? To answer these questions, we evaluated mobile polling in selected nursing homes in the State of Vermont during the U.S. 2008 general election.
Methods
The State of Vermont served as our demonstration site because one of our research team was Secretary of State of Vermont and a participant in the project that developed the ABA recommendations. In Vermont, voting policies and procedures are administered by the Office of the Secretary of State. Voter registration and balloting are implemented by town clerks, nonpartisan public officials elected every one to three years, and hereafter in this report described as “election officials.” Vermont uses a paper ballot and is an “early voting state”; meaning, in a general election, voting starts no later than 30 days prior to a general election.
Design of the mobile polling intervention
We used voting materials developed by Cook County, Illinois 21 and Australian 22 election officials to develop a mobile polling policy and procedures manual and to train election officials to conduct mobile polling. The training consisted of printed materials, a face-to-face group training meeting, and a telephone follow up to answer questions that focused on how to (1) ask whether a person needs assistance; (2) read the ballot to a voter; and (3) respond to a request for assistance, questions about the ballot content, and help selecting a candidate. Officials were trained not to assess resident capacity to vote. Rather, they were trained to know the limits of assistance they could provide to residents. (A copy of the mobile polling policy and procedures manual is available upon request to the first author or by visiting the American Bar Association Commission on Law and Aging website, at <http://www.abanet.org/aging/voting/pdfs/Mobile_Polling_Project_Handbook.pdf>. 23
Nursing home selection and random assignment to mobile polling intervention
Eligible nursing homes were long-term care facilities in the State of Vermont that were designated as nursing homes by Medicare guidelines, had a residential capacity of at least 40 residents, and were located in a town whose clerk had experience conducting at least one general election.
This study employed a randomized, matched case-control design so as to estimate the effect of the intervention. In particular, eligible nursing homes were matched on the basis of the number of residents with pre-specified levels of cognitive skills of either independent or modified independence. We obtained this proportion by multiplying the facility's residential capacity by the proportion of residents with Medicare Minimum Data Set cognitive skills for daily decision-making level 0 or 1 (independent or modified independence). This matching assured us that, between the homes where mobile polling occurred versus where voting occurred as usual, there was reasonable similarity in the residents' cognitive status. Within each matched pair, sites were then randomly assigned to either the mobile polling intervention or the voting-as-usual control group.
Data Gathering
This study had three data sources: the person at the nursing home most familiar with voting, local election officials, and the Secretary of State of Vermont. We adapted survey methods used in a prior study to examine voting in long-term care. 3 To facilitate the pace of interviews while assuring the accuracy of data collection, we digitally recorded the interviews and transcribed answers to open-ended questions.
(1) Nursing home staff.
The week after the November 4, 2008 general election, a research assistant faxed a letter to each site's activities director, followed up by a phone call, to identify the person who was most familiar with voting practices. A research assistant conducted a telephone interview that consisted of short-answer and open-ended questions to assess the following: (i) how many residents voted; (ii) the reasons residents did not vote; (iii) procedures for voter registration, voting, and voter assistance; and (iv) staff satisfaction with voting procedures including, if applicable, mobile polling. We developed the interview by modifying questions used in a previous study 3 to fit our current objectives. The interview included questions to ascertain both site and respondent characteristics, such as the number of residents, the respondent's position, years worked at the site, and years working in long-term care.
(2) Local election officials.
The week following the November 2008 general election, a research assistant contacted the town clerk's office to identify each person who had served as a mobile polling site presiding officer (the election official in charge of voting) and recruited those individuals for an interview.
The interview consisted of a telephone administered survey, with short-answer and open-ended questions to assess the following: (i) procedures for voter registration, voting, and voter assistance; (ii) resources needed for mobile polling; (iii) problems or challenges with mobile polling; and (iv) satisfaction with mobile polling. We developed the interview in collaboration with Vermont's Secretary of State by modifying the questions asked to nursing home staff. The interview included questions to ascertain respondent characteristics such as the respondent's role and years worked in elections.
Election officials who served as presiding officers were also asked to identify individuals who assisted them at mobile polling sites. With their permission, we contacted at least one of these individuals in each site and recruited these assistants to participate in a shorter version of the election official telephone interview.
(3) The Secretary of State
Three months after the election, three of the investigators and the research assistant team interviewed the Secretary of State to assess her experiences, lessons learned, and views on the benefits and challenges of conducting mobile polling. The interview was transcribed and reviewed by the investigators and research assistants for key themes and points.
Data analyses
Answers to fixed-choice questions were summarized using appropriate summary statistics. We used parametric or non-parametric statistics to compare voting practices and voting rates in control versus intervention sites.
To analyze the answers to the open-ended questions, we used a two-step method of qualitative data analysis. In phase 1 of open coding, two research assistants generated a summary of the responses to each open-ended question. Because we anticipated a small data set, we were able to examine the full set of open-ended responses for each question. In phase 2, the research assistants and principal investigator met as a group to review these summaries in order to generate a list of codes for the answers to each question. At these meetings, consensus was reached on the meaning of each code, and similar codes were combined and grouped into categories. After each question had been assigned codes, the research assistants and the principal investigator met to examine agreement, refine the code categories to accurately match the data, and develop consensus codes for the open-ended questions in each interview. The last step of data analysis was development of the codebook and final coding. The three research assistants used the final set of codes to code all interviews. All disagreements among the three coders were resolved by group discussion. The results were a final set of consensus codes for each qualitative question.
Human subjects protections
All subjects gave verbal informed consent to participate in this University of Pennsylvania institutional review board-approved study.
Results
Characteristics of the nursing homes
Of the 42 nursing homes in Vermont, 28 met our eligibility criteria, 14 were randomly assigned to the mobile polling intervention and the remaining 14 were assigned to the control condition. Figure 1 displays the disposition of these facilities to either mobile polling or voting as usual; that is, a comparison facility.
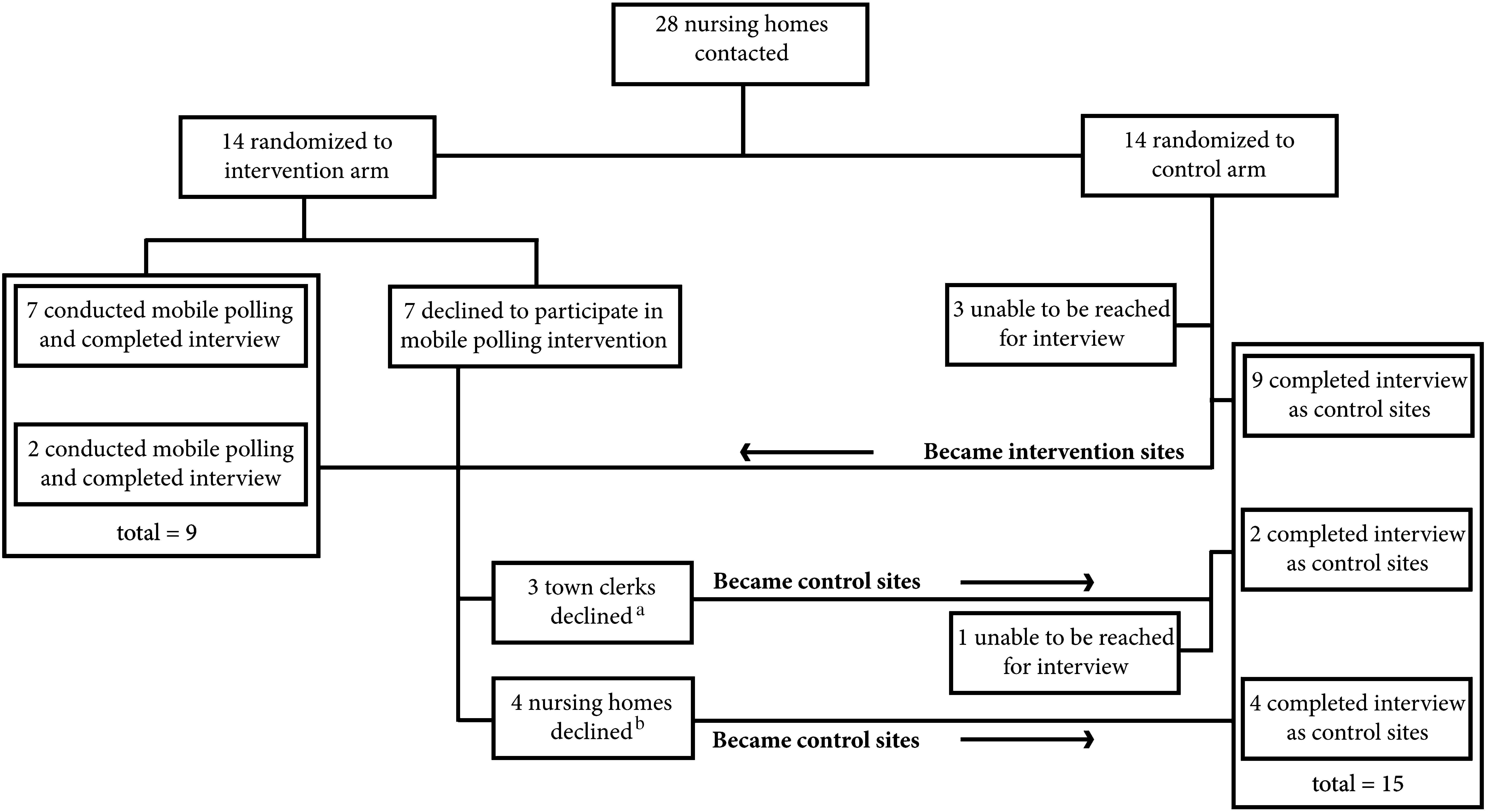
Disposition of nursing homes to either mobile voting or comparison facility. aClerk did not feel capable (2); clerk could not find enough poll workers (1). bStaff had already begun absentee voting process (2); no reason stated (2).
Among the 14 comparison facilities, we were unable to reach three for an interview. Among the 14 facilities randomly assigned to mobile polling, seven did not participate: three because the election official declined and four because the home declined. Two of these homes did not give a reason and two stated they needed more time to prepare for mobile polling. Among these seven facilities, all but one were studied as voting-as-usual sites.
If a home's declining to participate in mobile polling is considered equivalent to a home's being unreachable for interview, we can infer that this field trial had a 3/14–4/14 (22–28%) noncooperation rate. Further, we can also infer that, despite official state support for the field trial, the prospective burden or complication of mobile polling reduced election officials' cooperation by ∼22%.
To assure we had adequate survey data from intervention sites, we reassigned two control sites to mobile polling and matched them to appropriate control homes. In summary, a total of nine facilities received mobile polling and 15 facilities performed voting as usual. On Election Day, 879 residents resided in the nine mobile polling homes and 1,397 in the 15 voting-as-usual homes. The combination of this experimental and quasi-experimental design means that all statistical comparisons were made twice: once for the full dataset (9 intervention and 15 control) and a secondary analysis for the sites which carried out the experiment as randomized (7 intervention and 9 control sites). Analyzing the data both ways recognizes the tradeoff between loss of power and taking advantage of the randomization scheme.
The impact of mobile polling on voting rates
Nearly all long-term care facilities were unwilling or nonresponsive to requests from the Secretary of State's Office for a list of their residents. The most common reason was that they could not disclose the information because they viewed it as information protected under the Health Insurance Portability and Accountability Act (HIPAA). 24
As a result of the interpretation of HIPAA law by the people who manage these facilities, we could not accurately assess the impact of mobile polling on voting rates. In particular, the Secretary of State's office was unable to match the resident lists to the State of Vermont voter checklist and thereby determine the exact proportion of registered residents who voted at each nursing home. However, we did ask each staff member responsible for voting at the long-term care facility to estimate how many residents voted.
Comparing the nine intervention homes to the 15 voting-as-usual control homes, the estimated proportions of residents who voted were 37%±22 (range 15–79%) versus 25%±11 (range 2–41%). The difference between these proportions was not greater than chance (Wilcoxon Mann-Whitney z =−1.16, p = 0.24). Using only the as randomized sites, staff estimates of intervention site voting rates was 34%±22 (range 15–79%) compared to 20%±10 (range 2–40%) for control sites. The difference between these proportions was also not greater than chance (Wilcoxon Mann-Whitney z =−1.54, p = 0.12).
How residents voted
As expected, most (72%±19, range 45–100%) residents at homes assigned to mobile polling voted using mobile polling and all homes assigned to mobile polling reported that an election official had to help residents complete their ballot. A smaller portion of homes assigned to mobile polling reported that some residents voted absentee (31%± 17, range 12–55%), and a much smaller portion voted at a polling booth (0.7%±1.4, range 0–3.8%). In contrast, at comparison homes, most residents voted using an absentee ballot (95%±13, range 50–100%) and all comparison homes reported that someone had to help residents complete their ballot, and nursing home staff provided most of this assistance. At both mobile polling and comparison homes, residents needed assistance to read the ballot and fill it out. At mobile polling homes, a total of 43 residents registered to vote immediately before they voted (representing approximately 5% [43/879] of the total number of residents in those homes).
The benefits of mobile polling
The election officials we surveyed described three advantages of mobile polling: decreased workload, improved voter access, and high satisfaction with the process.
Comparing the views of long-term care staff members at nursing homes where voting as usual occurred to the views of the staff members at mobile polling sites shows that mobile polling generally reduced the challenges that staff members faced with voting. At voting in the “as usual” homes, staff described seven challenges: (1) difficulty judging whether a resident has the capacity to vote; (2) not being sure of what is proper voter assistance; (3) the voting process is time consuming; (4) a potential for staff to either inappropriately influence a resident's vote or commit voter fraud; (5) the effort to figure out whether a voter is registered; (6) the process was unofficial and not part of communal civic process; and (7) the burden of paperwork.
Among these challenges, most staff members' remarks were notable for their perception that it was part of their task, and a very uncomfortable part, to decide who has the capacity to vote. Staff members also questioned whether their own skills were adequate to assist resident voters and worried that they could inappropriately influence a resident's vote. The following quote from a staff member at a control site illustrates how these issues interplayed:
QUESTION: Could you please describe any problems or issues you experienced with voting by residents at your facility? We are interested in any of your experiences related to your role in facilitating voting or any issues at all that could have come up.
ANSWER: There are very few people who initiate the request for a ballot. So it does leave it up to someone to initiate that if we want to help people exercise their right to vote … I've always struggled, for 27 years, with how far to go to encourage people to vote because perhaps as many as 80% have some cognitive impairment-memory issues.… I don't feel comfortable being the person who makes [voting] happen.
In contrast, the following quote from a staff member at a mobile polling site illustrates how mobile polling addressed the interrelated issues of voter capacity, voter assistance, and fraud.
QUESTION: Why would you want other facilities like yours to have mobile polling available to residents?
ANSWER: We really cannot even read the ballot to them but you know in the past, residents would say ‘what do you think? who do you think I should vote for?’ so with these two officials there representing both parties, mobile polling took the load off us. It took the uncomfortableness out of it for us. As much as we want to help people do the right thing, or what we think they would think is the right thing, this was not an area that we could get into. So mobile polling took a lot of pressure off us.
The remark that “we cannot even read the ballot to them” illustrates how some long-term care staff members mistakenly understood what constitutes proper voter assistance. The remark “mobile polling took a lot of pressure off us” was a common theme across mobile polling sites and illustrates how mobile polling relieved staff anxiety over how best to conduct voting and whether their voter selection and assistance techniques were appropriate.
Staff members at mobile polling homes typically reported that mobile polling enhanced resident dignity and self-esteem. This observation is illustrated by the following quote in answer to the question: “Why would you want your facility to participate in mobile polling again?”
I think mobile polling is very good for the residents' self-esteem. It makes them continue to feel like a worthy part of the community and in the political system.
All of the facilities that received mobile polling reported that it was helpful, that they would do it again, and that they would recommend it for facilities like theirs. The following remark illustrates this finding:
I think that mobile polling would be extremely helpful. It would assist the town clerk's office. It would also assist the residents in being able to register and vote, both, if they needed to do that. And not having to go through the whole process of the absentee ballot making sure they remember to ask or to let someone know that they want to participate. It's right there in their facility, they don't have to leave. It's handy.
Thirteen of the 15 facilities that performed voting as usual expressed a willingness to conduct mobile polling after being given an explanation of mobile polling. The following explanation from a control facility illustrates how facility staff would value the effect of mobile polling on resident dignity and the benefits of the reduced hassle of voting:
The residents would love that. They would feel like a human being … They love the fact that they can participate in our country and our residents are so proud to be members of this country and take voting seriously and they would love to have one less hurdle and do something they have done all their lives, going to a polling place.
The two control facilities that did not want mobile polling conducted in the future explained that most of their residents had Alzheimer disease and whether these residents voted was, for one facility, the responsibility of family members or someone else the resident trusted, or, for the other facility, that the residents' council would have to decide whether to have mobile polling.
The challenges of mobile polling
Long-term care staff in the intervention facilities noted that mobile polling challenges included the time to conduct it, getting comfortable with the procedures, and the threats to the privacy of voting. Respondents' discussion of voting privacy noted how most residents needed assistance with completing the ballot and that the most common form of assistance was reading the ballot aloud to the residents. Election officials noted similar challenges. One explained:
It was difficult to maintain privacy for the residents when the ballots had to be read out loud and there was more than one voter present in the room at the time. This was especially true in facilities which provided an inadequate space for the mobile polling station, when the location of the voting area was too small.
However, respondents did note that a resident's loss of privacy was mitigated by a gain in not having to tell one's vote to a staff member at the nursing home.
The election officials who participated in mobile polling generated the following list of necessary resources: (1) a large and private space; (2) a nursing home staff member dedicated to assist the election officials, such as bringing residents to the room; (3) a laptop computer with the voter database; (4) a list of the residents who expressed an interest in voting on the day of mobile polling; (5) a voting booth that is accessible to a disabled person; (6) a container to hold supplies; and (7) nametags for the election workers.
The statewide perspective on mobile polling
The Secretary of State's experience with mobile polling revealed that to achieve the goal of universal mobile polling in a state, the process should be set up and implemented using a culture change effort. This approach is distinct from a top-down mandate requiring that all voting districts perform mobile polling. Rather, the approach requires election officials and long-term residential care staff members to value the intervention, undergo training, and recognize their own biases to adopting mobile polling. These biases include views on whether persons who may have cognitive impairment can vote or even should vote and whether it is worth assisting such voters. States with early voting may be well suited to implement mobile polling. In such a state, mobile polling is essentially “early voting on the go.”
Administrative challenges to studying mobile polling include obtaining legislative authority because some representatives were concerned that mobile polling would limit their ability to campaign in long-term care facilities. A state that wishes to assess the impact of mobile polling on voting rates would also need to clarify laws to allow the state authority charged with enforcing voting to obtain a list of residents of a long-term care facility.
Discussion
In the U.S., the rapid increase in the population of older and disabled adults presents substantial challenges. One key challenge is that these adults have disabilities that are not only the result of physical impairments, but cognitive impairments as well. Policymakers need to address these disabilities to assure that older adults maintain their right to vote. This is particularly true for residents of nursing homes who face issues of exercising their voting rights as well as their vulnerability to being victims of voter fraud. Mobile polling is an attractive means to address all of these issues.
Despite official State support for mobile polling, the willingness of residential sites or election officials to participate in mobile polling was not high: only 7 of the 14 sites and election officials that were randomly assigned to the mobile polling condition were willing to participate. In effect, this is then a randomized controlled trial of the extent to which an invitation to try an innovation and participate in a survey actually results in cooperation. The sites and election officials targeted for mobile polling are likely to have perceived a burden or distraction from usual routines. We of course cannot comment directly on other unstated reasons for not cooperating.
Nonetheless, this study comparing mobile polling to voting as usual has the following key findings: (1) among election officials and nursing homes willing to try mobile polling, it is feasible and generally well accepted by long-term care staff, residents, and election officials; (2) it reduces concerns of voter fraud and manipulation; and (3) it enhances residents' dignity and rights. The challenges of mobile polling include motivating and training election officials to perform it, providing resources to staff the homes, assuring voter privacy, and obtaining the names of the residents of long-term care facilities in order to assess the proportion of residents who voted.
A notable finding was that nursing home staff are uncomfortable with their perceived duty to decide who has capacity to vote, the vagueness of this role, and the uncertainty in knowing how best to assist residents to vote. The findings that absentee balloting was the dominant method of voting in voting-as-usual homes and that residents needed assistance to complete the absentee ballot reiterates previous studies of voting in long-term care facilities. 3 These data support the value of mobile polling to assure resident access, proper assistance, and to limit voter fraud. Notably, the election officials who assisted residents did not perceive their role to be one of assessing capacity to vote. This finding suggests that the training they received was effective to avoid capacity assessment and to learn the limits of assistance permissible to give voters.
Both staff and election officials reported that mobile polling enhanced resident dignity and self-worth. Such a benefit can have substantial impact on enhancing resident quality of life, an essential goal in the care of persons who have chronic and often progressive illnesses that cause substantial disability. Election officials can use this finding as part of their efforts to promote mobile polling.
Medicare regulations require that long-term care facilities “protect and promote the rights of each resident, including … the right to exercise his or her rights … as a citizen or resident of the United States.” 25 The results of this study warrant the Center for Medicare and Medicaid Services, the federal body in charge of enforcing long-term care regulations, encouraging long-term care facilities to reach out to election officials to engage them in conducting voting. These results also support the value of legislative or regulatory protocols for election officials to do outreach to long-term care facilities in the form of mobile polling, or at least to facilitate absentee balloting in those facilities. Election officials can find assistance in the U.S. Election Assistance Commission guidance on voting in long-term care. 26 Models of successful voting in long-term care exist such as in Cook County, Illinois; Kitsap County, Washington; and Multnomah County, Oregon; 6 and the ABA has prepared a website summarizing these programs as well as other models and resources. 27
Currently, these models are viewed as promising practices, but if their utility and feasibility become more widely affirmed and routinized, as the Vermont experience suggests is possible, then the case for universal application of these models as necessary reasonable accommodations under existing voter rights laws becomes a potential instrument for disability and voting rights advocates, particularly when combined with the obligation of long-term care facilities to promote residents' civil rights.
A notable finding of this study was that we were unable to precisely assess the impact of mobile polling on the number of residents who voted. This problem was the result of the failure to obtain the lists of residents from most of the long-term care facilities. Many facilities claimed that they could not release this information because they thought it was protected under HIPAA. This finding is notable because our efforts were coordinated by the Office of the Vermont Secretary of State and a review of the applicable law supported that this information is not protected health information. This result is important because it suggests that the federal Department of Health and Human Services and Department of Justice, along with relevant state departments and agencies, need to clarify the legality of a request for long-term care resident names for the purpose of monitoring registration and outcomes of an election. Alternatively, the authority of the state election director to receive facility resident rosters for purposes of voting oversight should be strengthened legislatively. The unexpected problems in study execution and obstacles in access to data, despite support of the state government, are important for future related efforts.
Limitations of this study include that the number of sites randomly allocated to the mobile polling intervention was too low to permit statistical power to make formal comparisons between mobile polling and voting-as-usual sites. Also, the State of Vermont is a largely rural state with small urban settings. Hence, our findings may not be readily generalizable to large and diverse urban locations. Finally, we limited our study to residents of nursing homes. We did this because we needed data available from Medicare that describe the residents at study sites so that we could properly match mobile polling to voting-as-usual sites. As a result, we did not study residents in assisted living facilities because no state or federal data existed to describe these residents' cognitive abilities. Nonetheless, given the prevalence of disability in residents of assisted living and the challenges of voting at these sites, 3 we can infer that mobile polling would likely have been applicable in this setting as well. In fact, it is quite possible it would be even better suited to assisted living facilities as residents of these facilities generally are less disabled than residents of nursing homes.
This study suggests that features of a state or election precinct that can successfully adopt mobile polling include the ability to conduct early voting, access to paper ballots such as absentee ballots, long-term care facilities which are willing to participate, and a good relationship between the chief election administrator and election officials. Election officials will need training in how to assist voters who require the ballot to be read to them and how to address challenges of voter privacy and voters who ask for assistance in picking a candidate or deciding upon a ballot initiative. A top-down mandate will likely not be as successful as an effort that targets culture change among motivated election officials and long-term care staff.
Footnotes
Acknowledgments
The authors thank the staff at the long-term care facilities and the elections officials who participated in this project, Ginny Colbert of the Office of the Secretary of State of Vermont, Faye Silag, and the team of research assistants: Paige Brookstein, Kristin Harkins, and Elizabeth Sullo.