
Abstract
Purpose:
We evaluated the feasibility and outcomes of performing a novel laparoscopic adhesiolysis technique before robot-assisted laparoscopic radical prostatectomy (RALRP) in patients with previous abdominal surgery.
Patients and Methods:
A total of 18 men with incision scars from previous abdominal surgeries underwent RALRP. A 12-mm trocar was placed at the lateral lower quadrant away from the incision site, and a teaching laparoscope was introduced into the peritoneal cavity. Meticulous adhesiolysis was performed through a single trocar to subsequently allow safe placement of additional robotic trocars. Age, type of previous surgery, total operative time, console time, anastomosis time, estimated blood loss, transfusion rate, complications, and conversion rate were recorded.
Results:
All patients had multiple abdominal surgeries. Mean operative time was 297 minutes, mean console time was 194 minutes, and mean estimated blood loss was 241 mL. No access-related complication and no conversion to open surgery occurred.
Conclusion:
This novel laparoscopic technique of adhesiolysis with a teaching laparoscope through a single trocar facilitates safe placement of trocars and accomplishment of RALRP in patients with previous abdominal surgery.
Introduction
Although conflicting data have been reported regarding the effect of previous abdominal surgery on the successful completion of laparoscopic renal surgery, 3,4 recent articles focusing on the impact of adhesions on robot-assisted laparoscopic radical prostatectomy (RALRP) reveal no increased complication rate. 5,6 Nevertheless, the extraperitoneal approach is an option in patients with previous abdominal surgery. 7 –9 This may not be feasible, however, if the surgeon is not experienced in this approach. In addition, the extraperitoneal approach is not suitable for surgeries such as extended lymphadenectomy, adrenalectomy, cystectomy, or intestinal surgery.
We aimed to evaluate the feasibility and outcomes of performing transperitoneal laparoscopic adhesiolysis through a single trocar using an offset teaching laparoscope with a built-in instrument channel in patients who were undergoing RALRP because of prostate cancer and had previous abdominal surgery.
Patients and Methods
A total of 18 men with previous abdominal surgery underwent RALRP because of organ-confined prostate cancer. After endotracheal general anesthesia, the patient was placed in the lithotomy position as necessary for robot-assisted prostatectomy. We usually use three assistant ports while performing RALRP with a three-arm robot (Fig. 1). The Veress needle was inserted at an off-site location and away from the previous incision sites. Depending on the location of previous incision scars, this could be on the left or right quadrant at the site where we place our assistant ports.
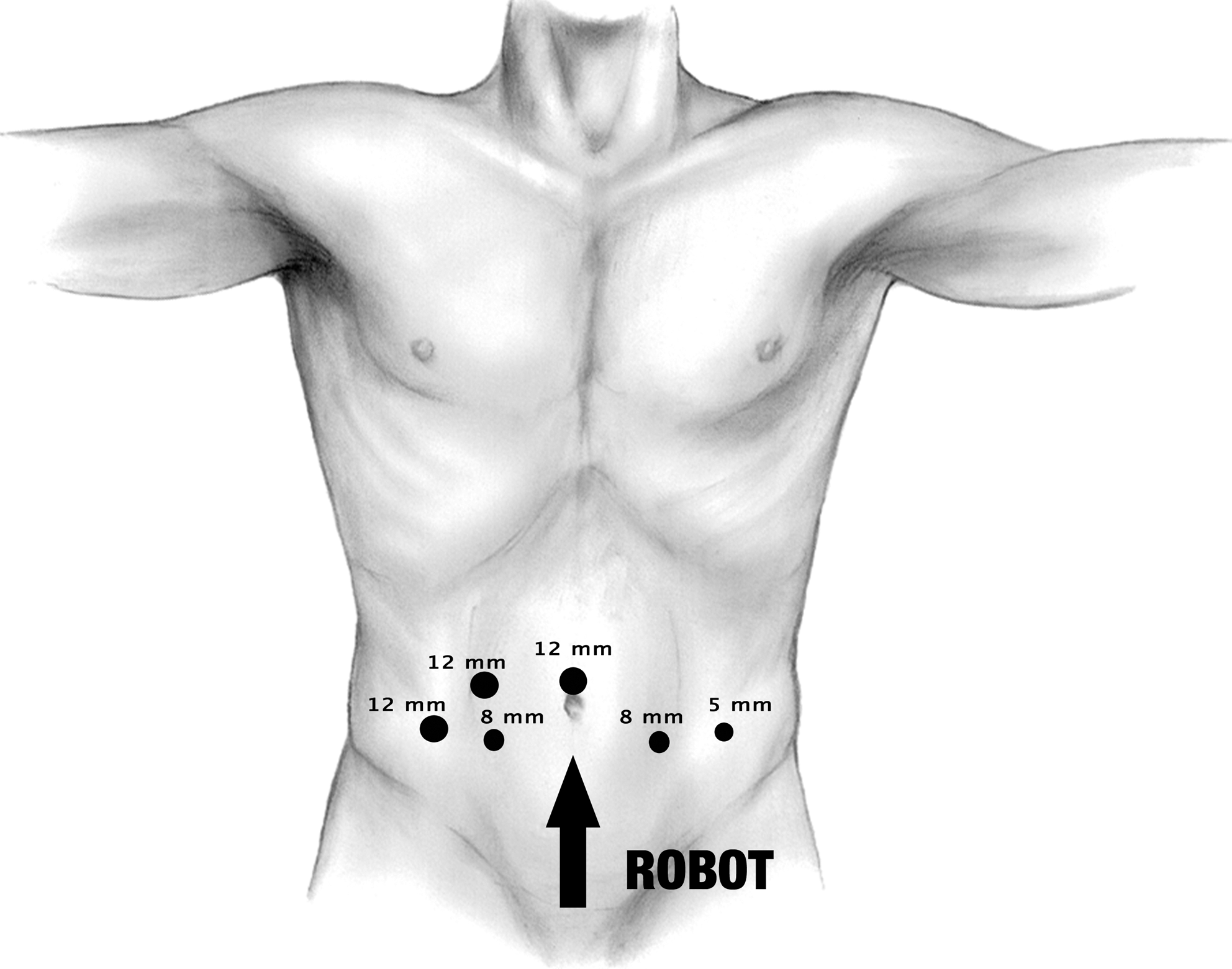
The diagram demonstrates the location of ports during robot-assisted radical prostatectomy (RALRP). A 12-mm umbilical camera port and two 8-mm robotic ports are used by the three-arm robot. Two 12-mm ports on the right side and one 5-mm port on the left side are used for assistance during RALRP.
After confirmation of opening pressures less than 10 mm Hg and achievement of adequate pneumoperitoneum, a 12-mm blunt trocar was placed at the same site as the Veress needle before introduction of the teaching laparoscope. A teaching laparoscope (Fig. 2) has an offset eyepiece and a built-in working channel, which allows the operative field to be visualized with concomitant passage of 5-mm laparoscopic scissors through the instrument (Figs. 3, 4). Careful and meticulous adhesiolysis was performed to allow subsequent safe placement of trocars (Fig. 5). With caution to avoid any bowel injury, adhesions were dissected free from the abdominal wall. Each time a site was cleared of adhesions, another trocar was introduced under direct vision, allowing the use of additional instruments such as graspers and scissors until all six trocars were in position. RALRP was then performed in standard fashion. 10

Teaching laparoscope with an offset eyepiece and a 5-mm scissors through its working channel.

Tip of the teaching laparoscope.

Teaching laparoscope through a single 12-mm port with 5-mm scissors.
Adhesiolysis with the teaching laparoscope.
With approval from the Institutional Review Board, the following parameters were retrospectively evaluated: Age, total operative time, console time, anastomosis time, estimated blood loss, transfusions, complications, type of previous surgery, and conversion to open surgery. SPSS (SPSS Inc, Chicago, IL) software was used for all data analysis. All data were expressed as mean ± standard deviation.
Results
Mean age was 59.67 ± 5.1 years (Table 1). All patients had an average of 2 abdominal procedures (12 colectomies, 9 open inguinal hernia repairs, 8 appendectomies, 6 explorative laparotomies, 4 cholecystectomies, and 1 failed RALRP attempt). Intraoperatively, extensive adhesions because of multiple previous surgeries, which would likely prevent a standard access, were observed in all patients.
SD = standard deviation.
Mean operative time was 297 ± 64.1 minutes, and mean console time was 194.67 ± 44.3 minutes. The 102.33 min difference between operative time and console time consisted of placement of ports, adhesiolysis, and preparation of the robot. The mean anastomosis time was 28.83 ± 16.4 minutes. There were no access related or intraoperative complications. In this series, no conversion to open surgery was necessary. The mean estimated blood loss was 241.67 ± 146.8 mL, and mean hospital stay was 1.33 ± 0.5 days. One patient needed a blood transfusion. No patient had a nasogastric tube, and all patients began oral intake on postoperative day 1. Postoperatively, one patient had hematuria and one had urinary retention.
Discussion
Patients with previous intraperitoneal abdominal operations may face increased risk of complications because of intra-abdominal adhesions of the bowel to the abdominal wall, as well as resulting distorted anatomy. In laparoscopic and robot-assisted prostatic surgery, the need for five or more trocar sites along with these adhesions may increase access-related injuries and subsequently cause significant morbidity and increased rate of conversion to open surgery. Moreover, urologists with inadequate experience in laparoscopic and/or robot-assisted surgery may not consider such minimally invasive surgical procedures as an option in patients with previous abdominal surgery. In addition, robot-assisted surgery needs particular attention to the location of the trocars in relation to the camera and the working arms, so as to prevent physical interference between robotic arms and the camera. Once the robot is docked, there is no way to alter the position of the patient without undocking the robotic arms and withdrawing the camera. This fact compels one to place the initial location of the ports in a crucial and strategic manner.
This study reports on 18 patients with an average of two previous abdominal surgeries in each patient. The outcomes of this novel technique of adhesiolysis with a teaching laparoscope and 5-mm scissors through its working channel for lysis of adhesions before robot-assisted prostatectomy is described for the first time. Our results demonstrate that no additional access-related or intraoperative complications were encountered.
Controversy exists regarding the “appropriate” technique for gaining pneumoperitoneum. Although open technique is suggested to access the peritoneal cavity in patients with previous abdominal surgery, no evidence exists of one technique's superiority to another. 11 Whether the Veress needle should be used first as opposed to directly using a blunt trocar or the Hasson technique is dependent on individual experience, training background, and availability of appropriate equipment. Veress needle technique may help in gaining quicker access to the abdominal cavity in comparison with Hasson technique, thus likely resulting in reduced operative time.
Seifman and colleagues 4 evaluated outcomes of laparoscopic renal/adrenal surgeries in previously operated (abdominal surgery) patients. To achieve pneumoperitoneum, the Veress needle was placed in the ipsilateral abdominal quadrant farthest from the previous incision. Radially expandable sheaths were the most commonly used trocars. The authors found no statistically significant difference in access-related complications between 76 patients who had undergone previous abdominal operation and 114 control patients.
Viterbo and associates 12 reported that the retroperitoneoscopic approach can be used for renal/adrenal surgery in patients with previous abdominal surgery and/or radiation without significant increases in morbidity. Lecuru and colleagues 13 reported data of laparoscopic surgeries with blind access performed in 881 patients, 39 with previous abdominal surgery and 842 without any abdominal surgery. There was no statistical difference between groups in complications because of insertion of a Veress needle or laparoscopic trocar.
There is no question that in the appropriate patient with previous abdominal surgery, one can proceed with an extraperitoneal robot-assisted prostatectomy. 14 This may not be feasible, however, if there are dense scars and adhesions infraumbilically and if the surgeon lacks experience in this technique. In RALRP with the extraperitoneal approach, a large prostate is associated with a slight increase in postoperative urinary complications. 15 In addition, an extended robotic pelvic lymph node dissection is very challenging, if not impossible, with the extraperitoneal approach. Moreover, for any type of robot-assisted surgery, in which the extraperitoneal approach may not be appropriate, such as cystectomy, adrenalectomy, and intestinal surgery, this technique will provide safe placement of robotic ports and will adequately let the surgeon perform the procedure with a transperitoneal approach.
Besides the absolute contraindications of laparoscopic/robot-assisted surgery, such as increased intracranial pressure, abnormalities of cardiac output and gas exchange in the lungs, chronic liver disease, and coagulopathy, the only relative contraindication of this novel adhesiolysis technique is insufficient surgical experience.
With the advent of robotic technology, a wide transition to robot-assisted surgery began and robot-assisted radical prostatectomy has taken the lead in urologic surgery. The vast majority of surgeons have learned and still perform this procedure with a transperitoneal approach. We strongly believe in “sticking with one technique” during the learning curve. Therefore, this novel adhesiolysis technique will prevent alternating approaches in robotic procedures in patients with previous abdominal surgery. We acknowledge the value and the indications of the extraperitoneal approach in appropriate patients, and we do not suggest this laparoscopic adhesiolysis technique through a single trocar instead of extraperitoneal prostatectomy. Further studies with larger series should be conducted to investigate the absolute clinical value of this novel technique.
Conclusion
This novel laparoscopic technique of adhesiolysis with a teaching laparoscope through a single trocar facilitates safe placement of trocars and accomplishment of RALRP in patients with previous abdominal surgery.
Disclosure Statement
No competing financial interests exist.