
Abstract
Introduction:
Congenital anomalies of the genitourinary tract are usually diagnosed and corrected in childhood. Robot-assisted management of congenital urologic abnormalities in adult patients has not been described previously. We present a series of patients with congenital renal abnormalities diagnosed in adulthood and managed using a robotic approach.
Methods:
Four patients at our institution were identified with congenital renal abnormalities diagnosed in adulthood. One had a duplicated collecting system with hydronephrosis of a thinned out upper pole moiety and underwent heminephroureterectomy. A second had right hydronephrosis, complete atrophy of the right renal cortex, and a dilated tortuous ureter with obstructing ureterocele and underwent simple nephrectomy. A third patient had a duplicated system with distal ureteral reflux and an ureterocele and underwent ureteroureterostomy and distal ureterectomy. The fourth had a duplicated collecting system with ureterovaginal fistula of the upper pole moiety. Perioperative variables were collected including operative time, estimated blood loss, length of hospital stay, and change in estimated creatinine clearance.
Results:
Mean age was 35 years (range 16–54), mean body mass index was 30.9 kg/m2 (21.8–42.5), and mean baseline estimated creatinine clearance was 147.7 mL/minutes (107.7–214.6). Mean operative time was 258 minutes (151–374) and mean estimated blood loss was 44 mL (25–50). Postoperative estimated creatinine clearance was 133.1 mL/minutes (115.9–160.9), which was not statistically different from preoperative values (p = 0.608). All patients were discharged by postoperative day 2. There were no perioperative complications.
Conclusions:
Robot-assisted management of congenital renal abnormalities is a feasible and efficacious treatment modality in adult patients with low morbidity and good outcomes.
Introduction
Congenital anomalies of the genitourinary tract are usually diagnosed and corrected in childhood. When symptoms arise from complications of a duplex system, surgical treatment is often nephroureterectomy or heminephrectomy with a flank incision causing postoperative morbidity. Since the first laparoscopic upper pole heminephrectomy by Jordan and Winslow 1 in 1993, there have been several reports of minimally invasive treatments for congenital renal abnormalities in children, 2 –9 but few in adults. 10,11 To the best of our knowledge, there have been no reports of robot-assisted management of congenital renal abnormalities in adult patents. In this article we describe our experience of robot-assisted surgery for congenital renal abnormalities in adult patients.
Patients and Methods
After retrospective review of our Institutional Review Board–approved robotic kidney surgery database, we identified four adult patients who underwent robot-assisted repair of a congenital renal abnormality between July 2008 and October 2009. Patients' medical records were reviewed, including operative notes, clinic notes, laboratory tests, and radiographic imaging.
One patient was found to have a duplicated collecting system with hydronephrosis and parenchymal loss in the upper pole moiety with hydroureter and an ectopic insertion (Fig. 1). She underwent a heminephroureterectomy. A second patient was found to have right hydronephrosis, complete atrophy of the right renal cortex (Fig. 2), and a dilated tortuous ureter with obstructing ureterocele and underwent simple nephrectomy. A third patient was found to have a duplicated system with distal ureteral reflux and an ureterocele in the upper pole ureter (Fig. 3) and underwent ureteroureterostomy and distal ureterectomy. The fourth patient had a duplicated collecting system with complete incontinence from a ureterovaginal fistula of the upper pole moiety after hysterectomy. She underwent a ureteroureterostomy. All patients had preoperative imaging with either CT or ultrasonography. Perioperative variables were collected, including total operative time, estimated blood loss (EBL), length of hospital stay, American Society of Anesthesiologists (ASA) score, and change in 24 hour postoperative estimated creatinine clearance using the Cockcroft–Gault formula.
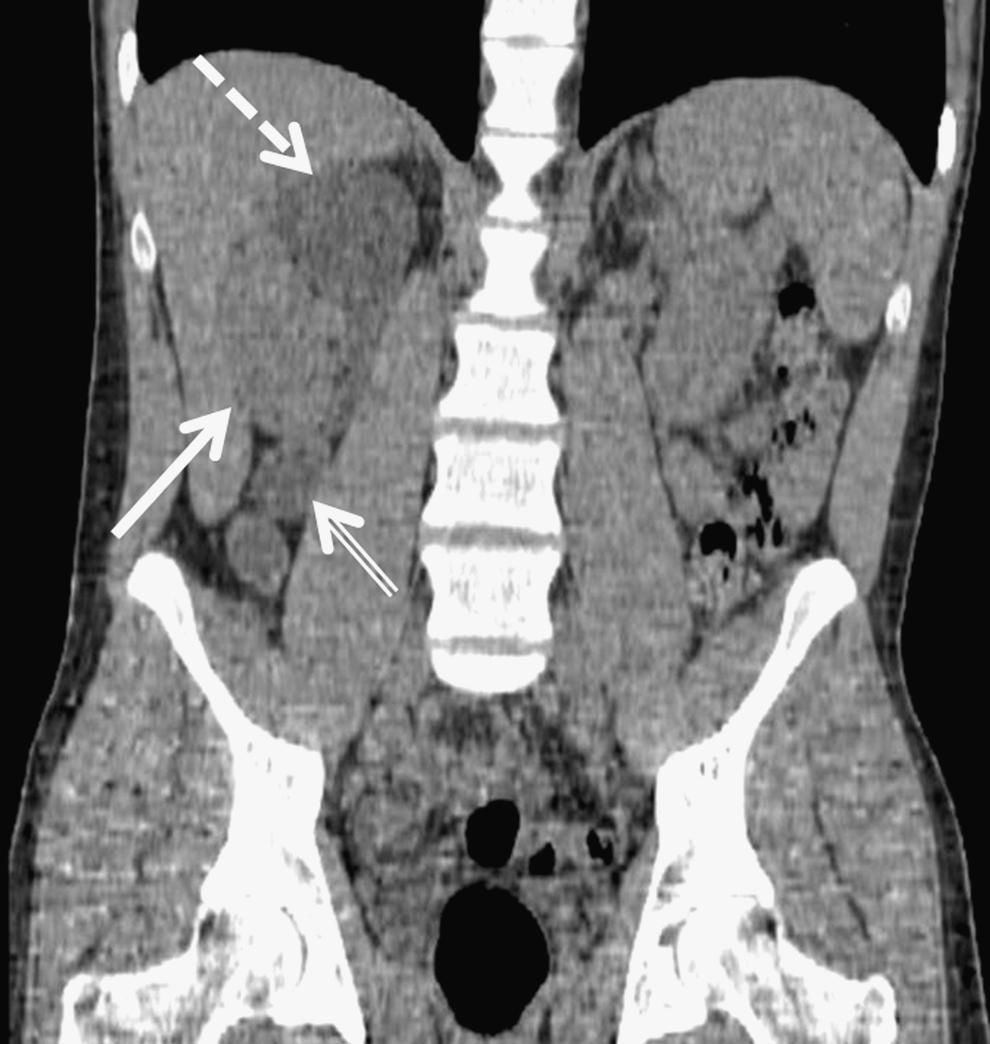
Reconstructed coronal CT demonstrating duplication of the right collecting system. The normal lower pole moiety (solid arrow) is seen adjacent to the dilated upper pole moiety (dashed arrow) with a dilated hydroureter (double arrow).
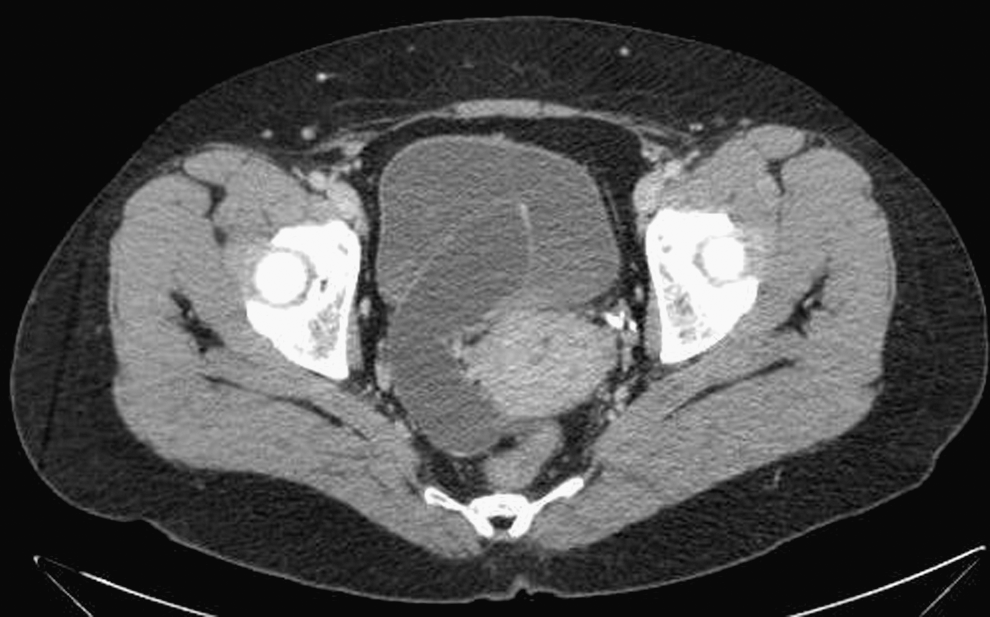
CT demonstrating a dilated ureter visible to its junction with the bladder, and a large ureterocele extending into the bladder.
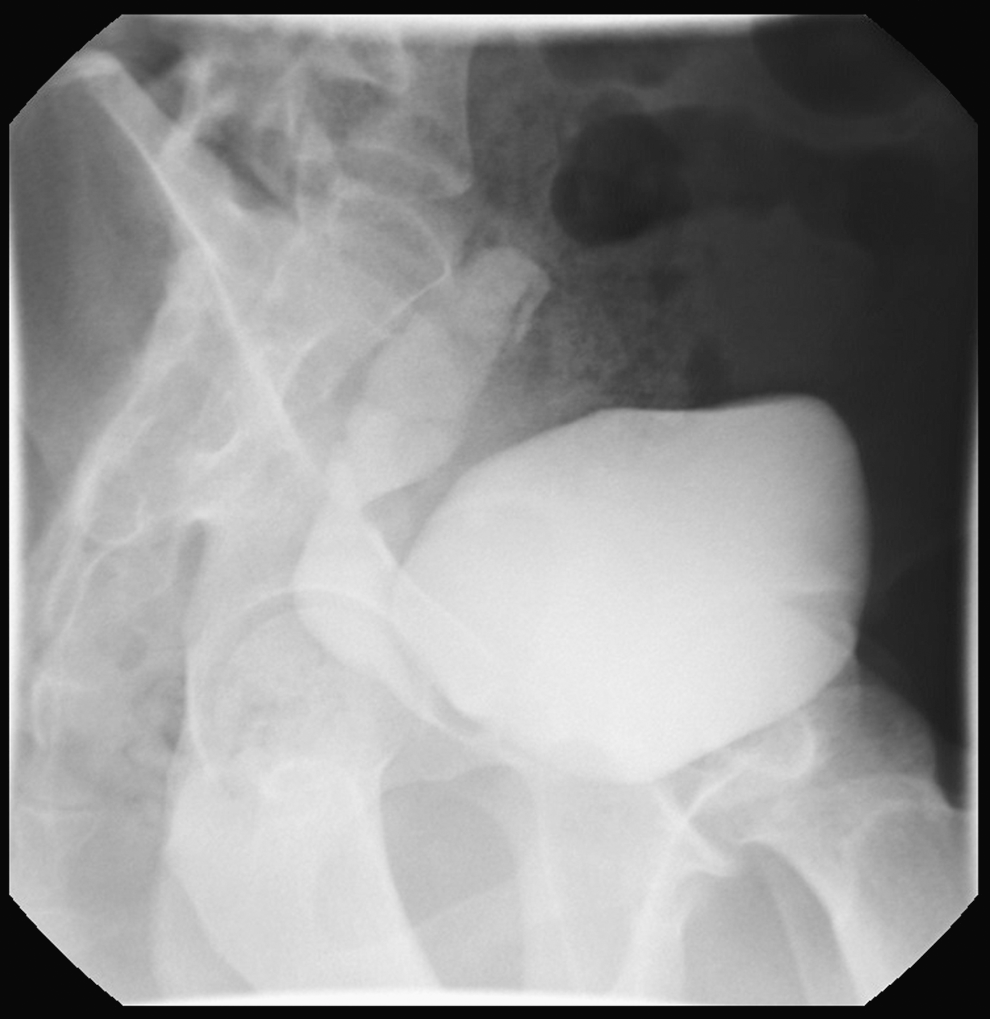
Voiding cystourethrogram demonstrating vesicoureteral reflux into the distal right ureter.
A lower pole ureteral catheter was placed in the three patients with duplicated systems. In the fourth patient with the ureterovaginal fistula a Double-J ureteral stent was placed in the lower pole ureter and a ureteral catheter was placed transvaginally. Insufflation to a pressure of 20 mm Hg was achieved using a Veress needle. A standardized port placement was used as shown in Figure 4 with the robotic camera in a lateral position, and the working ports in nearly a straight line that is perpendicular to a line drawn between the camera and the renal hilum. A 12 mm assistant port was placed periumbilically, and a port for the fourth robotic arm was placed 4 to 5 fingerbreadths medially and inferiorly to the most caudal robotic instrument port. For the ureteral portion of the case, the camera was moved to the assistant port, the left robotic instrument was moved to the fourth robotic arm port, and the right instrument was moved to the left robotic arm port.
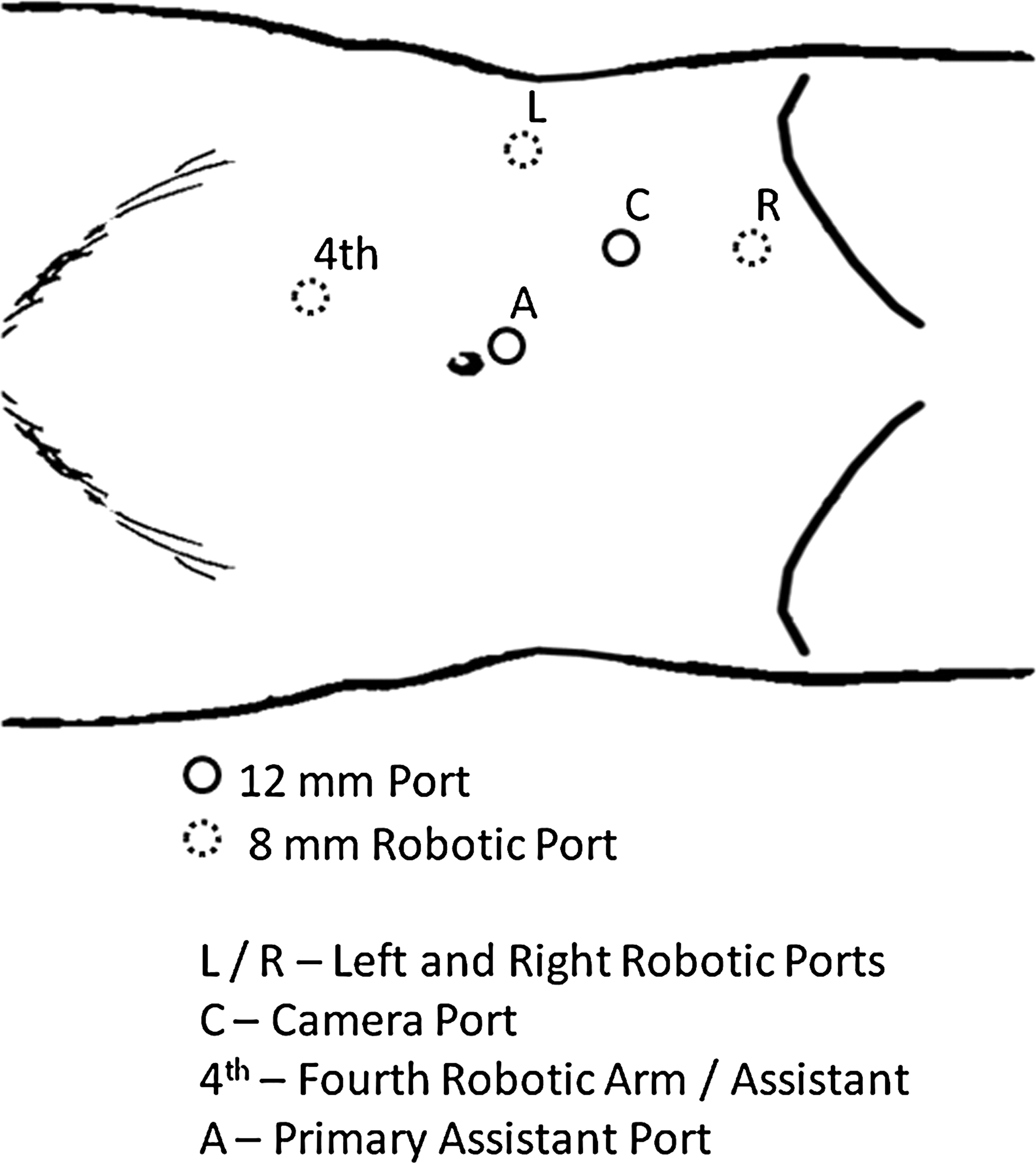
Port setup for robot-assisted repair of congenital renal abnormalities. The camera is placed laterally with a periumbilical assistant port and a caudal robotic port for fourth robotic arm assistance. To access the distal ureter, instruments can be moved by placing the camera in the periumbilical assistant port, the left robotic instrument in the most caudal port, and the right robotic instrument in the lateral robotic port.
In the first patient, the white line of Toldt was incised, the colon was mobilized medially, and the duodenum was kocherized exposing the renal hilum. The dilated upper pole ureter was dissected inferiorly to the pelvic brim. The ureter was transected at the level of pelvic brim, and the distal end of the ureter was left open for drainage. The ureter was transposed posterior to the renal vessels to facilitate dissection. The upper pole moiety was excised along the atrophic cleavage plane using sharp dissection, transected, and removed. Retrograde injection of indigo carmine through the lower pole ureteral catheter confirmed the collecting system to be intact.
For the second patient, the colon was mobilized medially along the white line of Toldt, and the duodenum was kocherized. The dilated ureter and gonadal vessels were identified and traced cranially to the renal hilum. The renal hilar vessels were ligated individually using Hemolock clips for the renal artery and a stapler for renal vein. The distal end of the ureteral stump was excised, decompressed with a suction aspirator, and left open.
For the third patient, the colon was mobilized medially along the white line of Toldt. The dilated upper pole ureter was identified and separated from the lower pole ureter. The upper pole ureter was transected at the level of the lower pole of kidney. Ureterotomy was performed in the lower pole ureter, and the lower pole ureter was spatulated. An upper-to-lower ureteroureterostomy was performed with two running 5-0 polydioxanone sutures. The upper pole ureter was then dissected out with blunt dissection and low cautery. The distal portion of the upper pole ureter was dissected to the bladder, and the ureterocele was identified. With an extravesical approach, the ureterocele was excised. The bladder defect was over sewn within the bladder wall by bringing the edges of the detrusor muscle over it in an imbricating manner using a running 4-0 Vicryl stitch. The bladder was filled with sterile water to ensure a watertight seal.
In the fourth patient, before insufflation, vaginoscopy was performed and a ureteral catheter was placed into the upper pole ureter. The colon was mobilized, and upon inspection it was noted that both ureters were present in a common sheath. The ureters were dissected and the upper pole catheter was retracted to identify this ureter. Once the ureters were identified, a transureteroureterostomy was performed. A longitudinal incision was made on the lower pole ureter, the upper pole ureter was spatulated, and an end-to-side anastomosis was performed using 4-0 PDS suture. The proximal end of the upper pole ureter was then ligated with a Hemolock clip.
Results
Mean age of the patients was 35 years (range 16–54), with a mean body mass index of 30.9 kg/m2 (21.8–42.5). Mean preoperative estimated creatinine clearance was 147.7 mL/minutes (107.7–214.6), and all patients had an ASA classification score of 3 or less. Preoperative voiding cystourethrogram (VCUG) was performed in two patients, demonstrating a nonrefluxing system in patient 1 and distal reflux in patient 3. Two patients refused to undergo testing.
Mean operative time was 256 minutes (151–374); mean EBL was 44 mL (25–50). Twenty-four hour postoperative estimated creatinine clearance was 133.1 mL/minutes (115.9–160.9), which was not statistically different from preoperative values (p = 0.608). All patients were discharged on postoperative day 1 or 2, and there were no perioperative complications.
Discussion
Complications of congenital renal abnormalities are a relatively common complaint seen by pediatric urologists. Duplicated systems are caused by incomplete fusion of the upper and lower pole of the kidneys. With this, an accessory ureteral bud creates a complete duplication of the excretory system, with the upper pole ureter entering the bladder more inferiorly and medially than the lower pole ureter (Weigert–Meyer rule). 12 The upper pole ureter is more likely to be associated with ureterocele and obstruction, whereas the lower pole ureter is associated with ureteral reflux. 13 In children, 80% of ureteroceles are associated with the upper pole moiety of a duplex system with an ectopically located orifice, whereas in adults they are usually part of an intravesical single system. 14
When the signs or symptoms of duplicated systems do appear, patients generally present with flank pain or urinary tract infection, and surgical intervention is aimed at heminephrectomy of the nonfunctioning moiety. For instances of isolated ureterocele in single systems, similar symptoms may occur, but surgical intervention is aimed at total nephrectomy since obstruction usually results in atrophy of the kidney. Traditionally, these procedures require flank incisions, which cause significant morbidity in terms of postoperative pain, and scarring. Since 1993 when Jordan and Winslow 1 performed the first laparoscopic heminephrectomy for a duplex system, minimally invasive approaches to surgical management of congenital renal abnormalities have become more common. Many reports of laparoscopic treatment for congenital abnormalities children 2 –9 have been published, but few laparoscopic reports have been published in adults, 10,11 and no reports have been published of robot-assisted treatment of congenital renal abnormalities in adults.
In each of the four cases reported, the patient presented with different variations of a renal abnormality, which was treated with robotic assistance. A VCUG is recommended preoperatively for all patients with congenital renal abnormalities to document the presence or absence of vesicoureteral reflux. In the first patient with a duplicated collecting system and atrophic upper pole moiety, VCUG demonstrated a nonrefluxing ureter that allowed the transected distal ureteral stump to remain open after heminephroureterectomy. If reflux had been documented on VCUG, the ureter would have been transected as low as possible and closed to avoid urine leakage and the possibility an infected ureteral diverticula. The second patient with an obstructing ureterocele refused to undergo preoperative VCUG. In this case, there was no clinical evidence of reflux and the decision was made to leave the ureteral stump open to drain any collected urine. Had the ureter been refluxing with creation of an urinoma, a percutaneous drain would have been placed until the stump closed off. In the third case, since VCUG only demonstrated distal reflux, a ureteroureterostomy was performed to preserve the function of the upper pole kidney. The fourth patient did not have a VCUG ordered, as her major complaint was incontinence after her hysterectomy without any clinical evidence of infection or reflux.
Laparoscopic repair of congenital renal abnormalities in adults has been described. 11 However, laparoscopy is technically challenging, requiring advanced training to perform upper tract reconstruction. A robotic approach gives the surgeon a number of tools that may aid with the technical challenges of upper tract reconstruction, including magnified three-dimensional vision, articulating instruments, scaling of movement, and fourth robotic arm assistance. The magnified three-dimensional vision and articulating instruments may facilitate precise tumor excision and reconstruction, while the fourth robotic arm allows the console surgeon to perform more tasks independently from the bedside assistant such as kidney retraction and hilar dissection.
In each case, ports were placed to allow access to both the kidney as well as the distal ureter without the need to undock the robot. For the renal portion of each procedure, ports were used as demonstrated in Figure 4. For the ureteral portion of each case, robotic instruments were switched between ports eliminating the need to place new ports or move the robot; the camera is moved to the periumbilical assistant port, the left robotic instrument to the most caudal port, and the right robotic instrument to the lateral robotic port.
In all cases, procedures were performed with complete robotic assistance without the need to undock the robot or add additional ports. EBL and hospital stay were comparable to similar laparoscopic series with operative times being slightly longer. 3,4,9,11 Limitations to this study include the small sample, limited follow-up, and the retrospective nature of the study. We have demonstrated that robot-assisted management of congenital renal abnormalities is a feasible and efficacious treatment modality in adult patients with low morbidity and good outcomes.
Footnotes
Disclosure Statement
No competing financial interests exist.