
Abstract
There is a continuous increase in incidentally diagnosed small renal masses, with a predominant rise in the elderly and frail population, making less invasive energy ablative therapy strategies more desirable. The decision for treatment and follow-up strategies, however, are commonly based on sequential radiologic CT or MRI investigations only. In small renal masses, up to 30% benign tumors may be found, not necessitating any treatment. Likewise, all currently available energy ablative techniques must be compared with respect to safety and efficacy; this is only possible by histologic definition of the treated target. Finally, not only for academic reasons, the malignant entity of the treated mass must be known for further follow-up investigations, especially when insufficient ablation is suggested during follow-up—suggested by lack of shrinkage and persisting contrast enhancement on CT or MRI. Therefore, liberal use of renal mass biopsy (Bx) is mandatory before any focal therapy. There is some role for intraoperative biopsy in selected cases and for study purposes. Conversely, the role of postfocal therapy Bx protocols remains unclear but seems at least mandatory in lesions that are seemingly insufficiently treated during follow-up. This article gives an overview of Bx protocols suggested in the literature and obtained by personal experience in the continuous use of several energy ablative techniques.
Introduction
Cryoablation seems to be the most reliable technique with a 1.6% recurrence rate over 3 years of follow-up with only 1.8% complications, 4 –8 but percutaneous techniques seem less effective compared with laparoscopy with recurrences rates ranging between 13% and 21% (cryoablation) 9 and 14% to 18% (RFA). 10 –12
All recently developed energy ablative techniques have one main drawback: They rely mostly on vague radiologic parameters such as attenuation or contrast enhancement patterns on standard CT or MRI scans. 13 –15 There are accumulation data, however, that radiologic measurements alone seem insufficient. 10,16–17 For benign solid renal masses, particularly angiomyolipoma, a distinctive radiologic pattern may be anticipated. 18
At our own institution, we performed a prospective CT-guided biopsy (Bx) protocol in 118 renal masses (patients) before surgery with a median tumor size of 4.1 cm (<4 cm 68%). At final histologic examination, 21% were benign lesions—mainly oncocytoma and angiomyolipoma. 3,16,19 These tumors would not need any treatment, particularly in elderly and frail patients.
Kim and associates 18 demonstrated a high attenuation rate on biphasic helical CT of 53% vs 13% in renal-cell carcinoma (RCC, P = 0.04); still, a high number of malignant tumors may present with the very same patterns. Likewise, Remzi and colleagues 3,19 evaluated 614 surgically removed renal tumors. At final histologic evaluation, 76 tumors were found to be benign. Unfortunately, at preoperative CT scans, only 17% were correctly diagnosed as benign lesions, 58% were intermediate, and 25% were even classified as malignant masses.
Sheir and coworkers 20 investigated clear cell, papillary, and chromophobe RCC (mean size 9 cm) with serial contrast-enhanced CT with respect to CT attenuation and enhancement but could not demonstrate any statistically significant differences. Recent published data suggest that even small renal tumors may represent aggressive tumors, necessitating more aggressive treatment. Remzi and colleagues 19 found 20% benign lesions in their series but with no correlation to tumor size. Of all solid tumors, 79% were RCC, of which 70% were clear-cell carcinoma, 14% multifocal, 14% grade 3/4, 22% ≥pT3a, and 6% M+. Likewise, in RCC 3.0 to 4.0 cm, 26% were grade 3/4, 36% ≥pT3a, and 8.4% M+. Therefore, they concluded that small tumors are not harmless, but some are less aggressive only.
A meta-analysis performed by Chawla and coworkers 21 with respect to tumor growth in 157 patients with a mean tumor size of 2.4 cm over a mean follow-up period of 3 years, demonstrates no correlation with respect to primary tumor size, Fuhrman grade, or with respect to oncocytomy vs RCC. The use of serial CT/MRI scans to evaluate tumor growth in surveillance protocols has proven unreliable, because volume change within 12 months accounted for a mean 10.3 cm3 vs 18.4 cm3. In addition, the surgical excision volume at the time of final surgery was already a mean 4.5 cm3. 11,22
In all ablative surgical techniques that leave the tumor in situ after treatment, patients have to be followed precisely with serial CT or MR (Fig. 1). Any nonshrinking lesion or, even worse, combined with persisting central contrast enhancement of the lesion suggests insufficient ablation. The radiologic result, however, may remain vague or would necessitate long-term and sequential follow-up CT or MRI scans. All these concerns with respect to the use of energy ablative techniques promote liberal use of renal mass biopsy to define the lesion and the success more precisely. 4,5,9,16,19

CT scan after 9 months of follow-up demonstrates complete disappearance of the tumor in patient GL, who was treated with laparoscopic high-intensity focused ultrasound ablation.
The suggested Bx protocol (Fig. 2) is an attempt to give an overview and recent suggestions and is also based on personal experience in this field. It must be noted that no commonly respected guidelines are available, leaving this field open for extensive discussion.
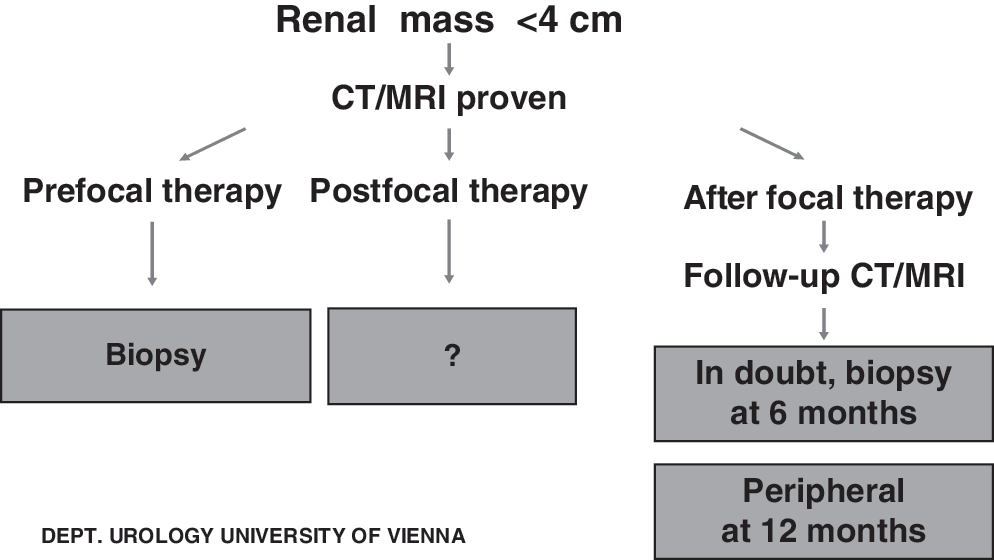
Suggested biopsy protocol, based on published data and standard operating procedure at own department.
Prefocal Therapy
Common radiologic assessment is based for cystic lesions according to the Bosniak classification. 23 In solid, contrast-enhancing lesions, histopathologic definition is possible for angiomyolipoma only, but may be difficult to interpret particularly in small lesions with low angio-content. 18 In all other cases, radiologic definition of malignancy remains insufficient or unreliable. 16,17,19 Therefore, the liberal us of core needle Bx seems essential before ablation to know the pathology with respect to benign vs malignant lesions, before any focal therapy; the results may even determine the precise follow-up requirements. Likewise, definition of success is then based on more detailed histophathologic data compared with vague radiologic investigation—being related to biases ranging from excellence of performing the CT/MRI scan protocols to (subjective) interpretations of results.
Core needle Bx should be performed with the patient receiving local anesthesia with CT guidance only. 7,16,24 At least two 17G representative core Bx samples should be taken and immediately checked for sample quality. An attempt should be made to get sufficient material for analysis, and two representative sites must be chosen. At our own institution, we performed a prospective CT-guided Bx protocol 16 in 118 (n = 118) renal masses before surgery with a median tumor size of 4.1 cm (<4 cm 68%); 21% were benign lesions at final histologic evluation—mainly oncocytoma and angiomyolipoma. Only 3/118 samples obtained were insufficient. The accuracy of defining malignancy was 97%; even the subtype classification was acceptable with 92%. Only grading (grade 1/2 vs grade 3/4) proved difficult, with only 74% correctly diagnosed cases.
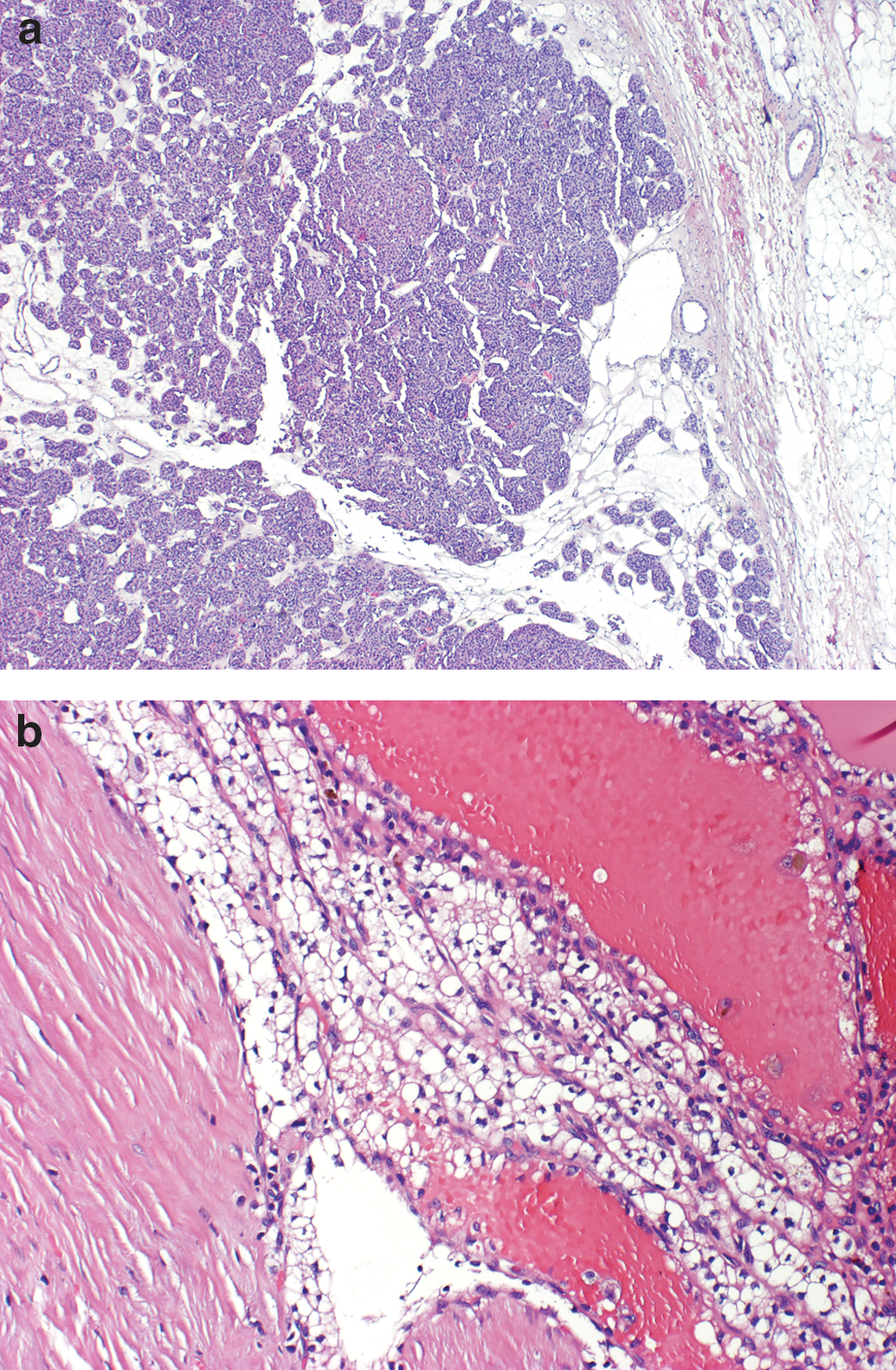
Still, any Bx material will at best represent 1% of the entire tumor volume and that having a specific proven tumor does not rule out tumors of other histology elsewhere (Figs. 3a and 3b). Detailed histopathologic analysis should be obtained only. 25 –27 Frozen section may be helpful to check for sufficiency of the sample only. Performing additional aspiration Bx seems particularly helpful in soft lesions; this, however, needs an experienced cytopathologist at hand. 16
(
Postablation Bx
There is little rationale for intraoperative biopsy except for selected cases. In addition, for study purposes, continuous online monitoring of the entire ablative procedure is not feasible for RFA because of interference with intraoperative ultrasound. 28 Likewise, monitoring of the ice ball during cryoablation is not synonymous for core temperatures <−20°C. 4 –8,9 Therefore, Bx may open a chance for immediate monitoring of the ablative process.
In all ablative surgical techniques that leave the tumor in situ after treatment, patients have to be followed precisely with serial CT or MR. Over time, the serial use of contrast-enhanced CT would amount to significant radiation exposure. 7,14,15 Alternative MRI may not be available at all times, and even contrast-enhanced renal ultrasonography is not reliable enough for routine use in such cases. Therefore, any immediate proof of irreversible tissue damage may be of help in the early defining of lesions that are at low risk for development of recurrence or persistence (Fig. 4). This could result in a significant reduction in the number of serial CT scans. This would be supported by results of Bastide and colleagues 24 in 10 patients with Bx-proven RCC treated with RFA before radical nephrectomy. Complete tumor-cell death was obtained in only 50% of cases, as proven by interpretation of histologic evaluation and nicotinamide adenine dinucleotide stains.
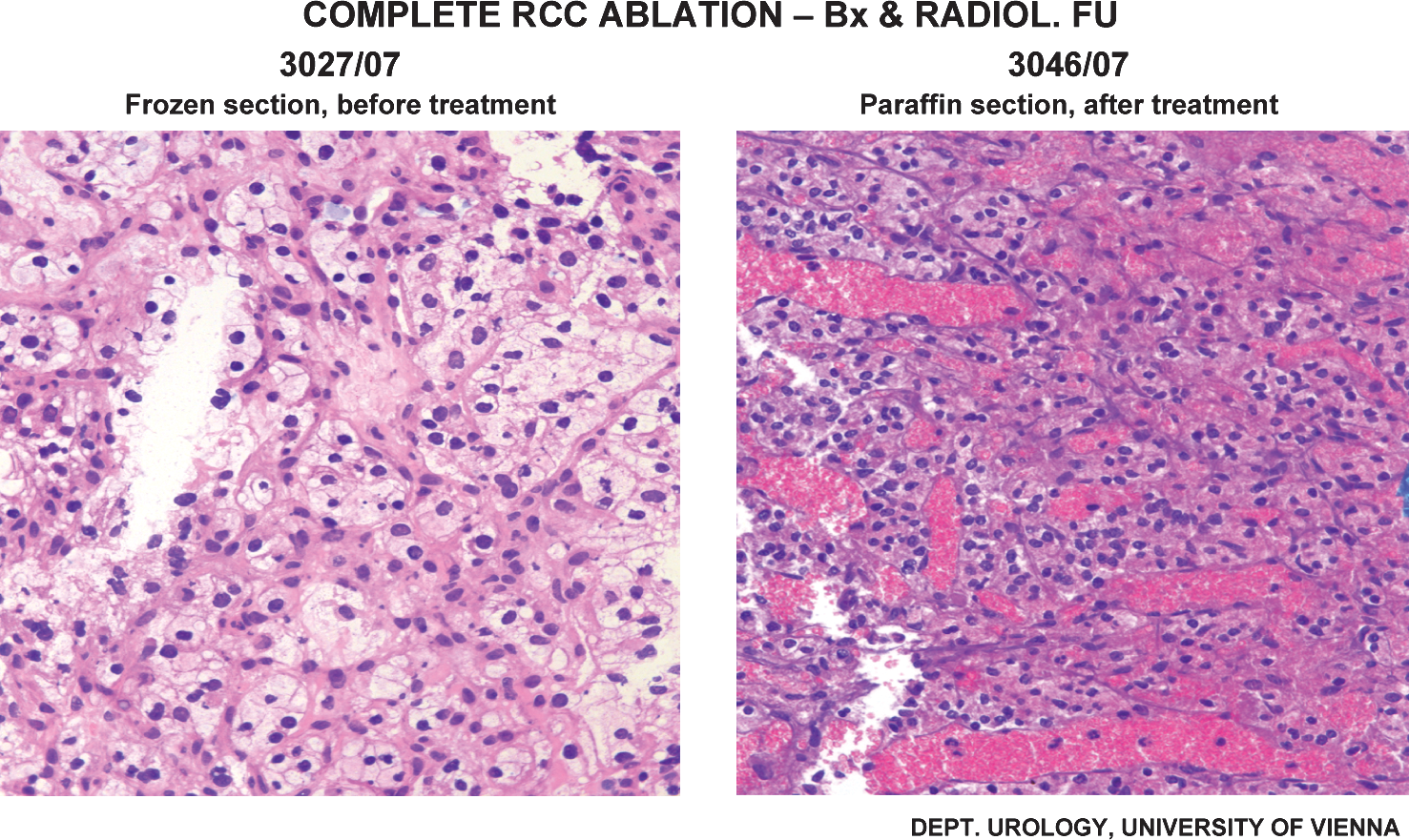
Patient GL, who was treated with laparoscopic high-intensity focused ultrasound ablation, demonstrates complete ablation at postablation biopsy.
Because vital tumor is more frequently present than previously anticipated, oncologic follow-up in tumors that remain in situ after treatment must primarily be grounded on histologic confirmation of malignancy and cannot rely solely on radiologic follow-up measurements alone. Definition of irreversible tissue damage after energy ablative therapy is difficult, however. Cell apoptosis and histologic signs of cell necrosis are dependent on time. In addition, vascular damage may lead to ischemic damage of the ablated tissue. Consequently, postfocal therapy Bx is jeopardized by the need to take immediate Bx postablation. With extensive histopathologic workup, however, definition of successful ablation may be possible (Fig. 4).
Follow-Up Procedures
During follow-up after focal ablative therapy, patients are routinely monitored with serial CT or MRI (Fig. 1). Kawamoto and associates 29 evaluated the accurate assessment of ablated tumors at postprocedural imaging. Renal tumors that were managed with RFA or cryoablation appear as low-attenuation regions at CT and, relative to renal parenchyma, are generally hypointense at T2-weighted MRI and isointense to hyperintense at T1-weighted imaging. The use of intravenous contrast material was found to be mandatory for the evaluation of residual or recurrent tumor, because no evidence of contrast enhancement is mandatory.
Decrease in size over time is a less common finding, particularly within the first year. 22 Matin and coworkers 30 evaluated 616 patients who were undergoing RFA or cryoablation in a multi-institutional study to determine how follow-up imaging should be performed after renal energy-ablative therapy. Sixty-three were found to have residual or recurrent disease after RFA (13.4%) or cryoablation (3.9%), but most incomplete treatments (70%) were detected within the first 3 months. The investigators suggested a minimum of three to four imaging studies in the first year after ablative therapy at 1, 3, 6 (optional), and 12 months. In addition, long-term follow-up at 18, 24, and 48 months is suggested. Still, the precise time points are not commonly accepted; in particular, the overall high radiation dose applied is of concern—at least for low-risk tumors (Fuhrman grade 1–2) for which close monitoring is not necessary.
A continuously shrinking lesion, particularly when there is absence of contrast enhancement of the lesion, suggests sufficient ablation. Therefore, in standard cases, routine core Bx of the ablated area seems unnecessary. Conversely, as per protocol and for study purposes, Bx of the ablated area is highly recommended, commonly after 6 months postfocal therapy. At least two representative Bx from different sites of the ablation zone are recommended. Early biopsy should be avoided, because the interpretation may prove difficult because of artefacts.
Park and associates 31 evaluated radiographic and histologic data in patients who underwent delayed partial or total nephrectomy after RFA. All three patients had Bx-proven RCC, and the mean time to nephrectomy was 18 months; all demonstrated absence of residual cancer within the ablation zone. The authors concluded that new enhancement at the peripheral margin of the tumor-ablation zone is not synonymous with tumor recurrence but may commonly represent a benign granulomatous reaction.
An interesting case of asymptomatic enterococcal abscess-mimicking recurrent RCC on MRI and positron-emission tomography-CT 15 months after RFA was reported by Roarke and colleagues. 32 This case illustrates that indolent infection can mimic recurrent neoplasm on imaging, thus making interpretation of “success” even more difficult. The need for post focal therapy Bx, however, is supported by recent reports that, even in radiologically nonsuspicious lesions, there is a good chance of identifying persistent or recurrent tumor at the ablation site. 7,9,17 Consequently, at least for any new ablative procedure, a 6-month follow-up Bx seems advisable to prove ablative effectiveness and reliability. In standard cases, follow-up after tumor ablation is grounded on changes in serial CT/MRI investigations, particularly the absence of contrast enhancement, and tumor shrinkage over time is a crucial finding for defining successful ablation. 7,29 Any persistent nonshrinking and contrast-enhancing tumor should be have a Bx performed. In cases in which central contrast enhancement is present, the Bx should be considered at 6 months; for persistent peripheral contrast enhancement, Bx at 12 months may be advisable.
Conclusions
Focal therapy with the aid of energy ablative techniques necessitates the liberal use of renal Bx protocols, essential before ablation to reveal pathology and at follow-up with signs of insufficient ablation of the targeted lesion. Core Bx is, at present, the best but not perfect option to define tumors that are suitablefor focal therapy. CT-guided needle Bx correctly identifies benign tumor with 100% sensitivity and 95% specificity, RCC with 93.5% sensitivity and 100% specificity, but RCC subtype and grade with 91% and 76%, respectively. Bx strategies, the precise techniques including staining, and the recommended time points for taking the Bx sample are still open to discussion.
Footnotes
Disclosure Statement
No competing financial interests exist.