
Abstract
Background and Purpose:
Greenlight® photoselective vaporization of the prostate (PVP) is an effective method for treating men with lower urinary tract symptoms. A rise in prostate specific antigen (PSA) levels, however, may be noticed in some patients during follow-up. The aim of this study was to determine whether the prostate cancer gene 3 (PCA3) urinary test would help identify patients who were in need of a prostate biopsy.
Patients and Methods:
The PSA of all patients undergoing PVP were analyzed. Patients with an elevated (above reference range) or rising PSA level (defined as >0.75 ng/mL/year if the PSA was between 4.1 and 10 or a doubling time of less than 2 years) were offered a transrectal ultrasonography (TRUS) guided prostate biopsy. Before the biopsy procedure, all patients had a PCA3 test. The relationships between PSA, PCA3, and TRUS prostate biopsy findings were analyzed to determine sensitivity and specificity for the PCA3 test in this setting.
Results:
50 patients were identified. The mean age was 69.97 (range 57–83) years. The mean PSA level was 10.1 ng/mL (range 3.03–44.2 ng/mL). Six patients were found to have prostate cancer. Of those, five patients had a positive PCA3 test. One patient had a negative PCA3 test but positive biopsy findings. This gives a sensitivity of 83.3%, and a positive predictive value of 21.7%. The negative predictive value was 96%.
Conclusion:
The results suggest that a negative PCA3 test in our group of patients is a good predictor of negative biopsy results. The low positive predictive value may be an artefact of the group size. This will need further investigation and greater patient numbers to determine.
Introduction
We have been performing Greenlight PVP since 2004. 4 During the routine follow-up of our patients, which included PSA monitoring every 3 to 6 months, we noticed a small proportion of patients had a rise in the PSA level after PVP. Usually, we would expect the level of PSA to fall after PVP, because the volume of the prostate had been reduced. To determine whether these patients harbored prostate cancer, or if the PSA level rise was secondary to an inflammatory reaction to laser surgery, a TRUS biopsy of the prostate would be indicated.
TRUS biopsy of the prostate is not without risk of discomfort and morbidity. 5 Recently, the prostate cancer gene 3 (PCA3), a urinary biomarker for prostate cancer, has been shown to be a useful test in the assessment of men with suspected prostate cancer 6 and in patients who have had negative biopsy results and have a persistently raised or rising PSA level. 7 The PCA3 assay detects the presence of PCA3 messenger RNA (mRNA) from a first-catch urine sample after a DRE. PCA3 is highly specific to prostate cancer, and this gene is overexpressed in more than 95% of prostate cancer cases. 6 In contrast to PSA, which may be increased by conditions such as BPE or prostatitis, the PCA3 test result is not affected by these conditions. The exact role of the PCA3 test in the context of a rising PSA level after Greenlight PVP has not yet been studied. We undertook this study to determine whether PCA3 test has a role in identifying patients who would benefit from a prostate biopsy in this setting.
Patients and Methods
This prospective study was performed from April 2008 to December 2008. The PCA3 test began to be used in our department from January 2007. Patients undergoing Greenlight PVP from January 2005 to May 2008 were identified from a prospectively collated database. Greenlight PVP was performed as a day case procedure by one of two surgeons using a 22F Richard Wolfe continuous irrigation cystoscope with the 80 W machine (Greenlight™, American Medical Systems, MN, USA). The PSA results of all patients before and after surgery were analyzed, and those with a significant rise in PSA level (defined as >0.75 ng/mL/year if the PSA was between 4.1 and 10 or a doubling time of less than 2 years 8,9 ) were identified. This group of patients underwent PCA3 testing followed by a TRUS biopsy of the prostate.
The PCA3 test was performed in a standardized manner by one of three clinicians who had all received training from an industry representative. It consisted of a DRE and palpation of each lobe of the prostate (enough to depress the surface by approximately 0.5 to 1 cm) three times in the direction from the base to apex and from the lateral to the median line. After DRE, the patient was asked to immediately void and 20 to 30 mL of the first-catch urine was collected into a universal container. The urine sample was then inverted five times to resuspend the cells. Using a pipette, 2.5 mL of urine was obtained and transferred into a dedicated sample tube for processing. This was stored below 30°C and shipped to a certified laboratory (The Doctors Laboratory, London). PCA3 and PSA mRNA concentrations were then calculated using the Progensa® PCA3 assay 10 method that uses transcript-mediated amplification technology to quantify the mRNA expression of both PCA3 and PSA in prostate cells collected from patient urine. The PCA3 score was calculated as [mRNA PCA3]/[mRNA PSA] × 1000. A PCA3 score of 35 or greater has been considered the cutoff point to suggest a risk of prostate cancer and is considered a positive score in this study. This is consistent with laboratory advice and has been shown to give the best diagnostic accuracy. 11
Regardless of the PCA3 test, all patients underwent a TRUS biopsy of the prostate. Clinicians were blinded to the results of the PCA3 test at the time of the biopsy. TRUS biopsy of the prostate was conducted using a protocol in keeping with nationally produced guidance. 12,13 Patients had 10 to 12 cores taken with antibiotic coverage and under local anesthesia. Biopsy samples were obtained using a standardized template. Abnormal areas seen on ultrasonography underwent further targeted biopsies. Results of the PCA3 test and histological findings from the TRUS-guided prostate biopsy were then compared. All calculations were performed using Prism for Macintosh 4.0 (GraphPad Software Inc). P < 0.05 was considered statistically significant.
Results
Over the 3-year period, 569 patients underwent Greenlight PVP in our unit. Of these, 50 patients were found to have a significant rise in their PSA level and underwent a TRUS biopsy of the prostate. The mean age of the 50 patients at the time of the TRUS biopsy was 69.9 years (range 57–83 y). The mean PSA level at the time of PVP surgery was 10.1 ng/mL (range 3.03–44.2 ng/mL). Within this group, 27 (54%) patients had a TRUS biopsy before the PVP that had negative findings for malignancy.
Of the 50 patients undergoing a TRUS biopsy, 6 patients (12%) patients received a diagnosis of prostate adenocarcinoma (positive biopsy group). Table 1 demonstrates the demographics between those patients with positive and negative biopsy findings after the rise in PSA level. Men who had positive biopsy results had a higher mean PSA density and serum PSA level. This is despite the mean prostate volume being significantly lower in the positive biopsy group (46.9 vs 80.4). The mean PCA3 score in the positive biopsy group (101.2) was significantly greater than that in the negative biopsy group (50.8).
PSA = prostate-specific antigen; PSAD = prostate-specific antigen density; PCA3 = prostate cancer gene 3.
Table 2 demonstrates the number of patients with positive and negative TRUS biopsy results for prostate cancer and their relationship to the PCA3 cutoff score of 35. The sensitivity of the PCA3 test for detecting prostate cancer was 0.833 (95% confidence interval [CI] = 0.356–0.996). The specificity was 0.591 (95% CI = 0.432–0.737).
PCA3 = prostate cancer gene 3.
The positive and negative predictive values were 21.7% and 96.3%, respectively. Figure 1 demonstrates the receiver operating characteristics of the PCA3 test in this study using a threshold PCA3 score of 35 for a TRUS biopsy. The curve shows that the PCA3 test result predicts biopsy result much better than expected by chance. In particular, a negative PCA3 test is a good predictor of a negative TRUS biopsy of the prostate. The overall accuracy of the PCA3 test as determined using the area under the curve was 0.773 (standard error 0.091).
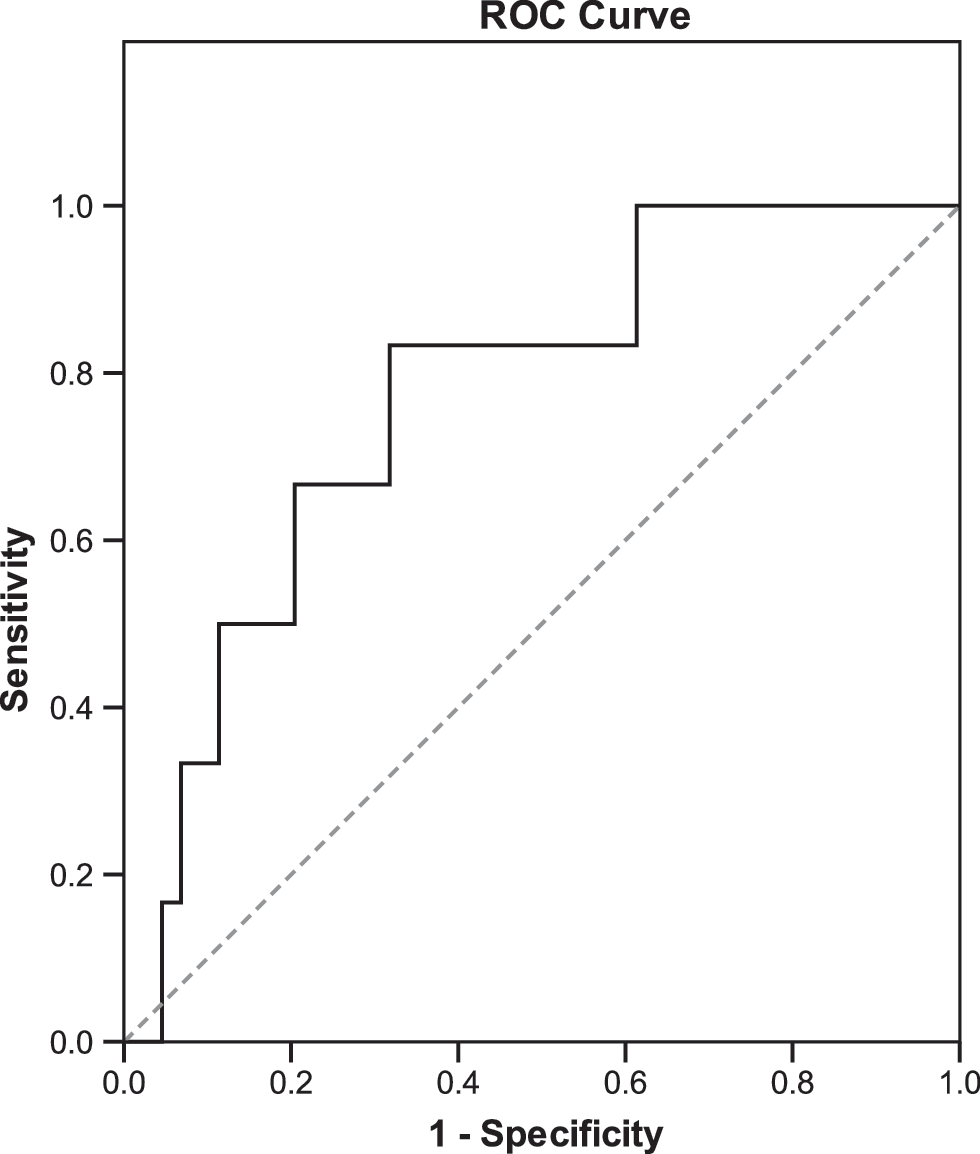
The stairstep line is the (nonparametric) receiver-operating curve (ROC) of the PCA3 test constructed using the biopsy threshold of a PCA3 score of ≥35. The dotted line is the ROC curve one would expect by chance alone.
Of the six patients with a diagnosis of prostate cancer, five patients had a Gleason score 6 adenocarcinoma, and the number of positive cores in these patients ranged from 1 to 4. There was one Gleason score 9 prostate cancer, and the corresponding PCA3 score in this patient was 83. In the one patient who had a positive biopsy results but had a negative PCA3 score (score = 22), the Gleason score was 6, with disease in only 7% of one core.
Discussion
Greenlight PVP is becoming a well recognized, safe, and efficacious method of treatment for patients with benign prostatic hyperplasia (BPH). 14 It has the advantages of shorter catheterization and hospital stay times compared with TURP and does not need the patient to stop receiving most anticoagulants. 3 This growing evidence has led to the increasing number of patients undergoing this minimally invasive procedure. Therefore, the group of patients who were identified in this study could become a frequently encountered diagnostic problem.
In this pilot study, we have identified a group of patients who, under current PSA follow-up, would need a biopsy to exclude malignancy. In this group, only 12% of the patients had positive biopsy findings. This is almost half the rate you would expect for a group made up of men in whom the majority had had a previous negative biopsy. This means we are doing unnecessary biopsies in nearly 9 of 10 patients. There is, therefore, an argument for not obtaining biopsies in this group at all, especially if the majority of cancers in the group are small, low grade, and noninvasive (indolent cancer). 15
The numbers of patients in our study with positive biopsies is low, and therefore we cannot accurately comment on the rate of indolent disease in this population. In keeping with previous studies, significant cancer was detected, highlighting the importance of repeated biopsies in selected patients. 16
PCA3 has been demonstrated to correlate with tumor volume and is associated with Gleason grade. 17 It therefore has the potential to help select the patients with significant disease who would benefit from active treatment. The high negative predictive value of PCA3 in our group suggests that it can be incorporated into the follow-up investigation of these patients to prevent men undergoing unnecessary biopsy procedures.
The results from this group may be able to be extrapolated onto patients treated with other modalities for BPH (ie, transurethral resection of the prostate, holmium laser enucleation of the prostate, and holmium laser resection of the prostate). A high PSA velocity level in these patients has been shown to be associated with an increased risk of prostate cancer. 18 PCA3 test could therefore be a valuable tool in helping identify patients needing a biopsy procedure after any type of BPH surgery.
The low percentage of patients with a positive biopsy compared with previous studies 16 may be a reflection of the group of patients and that the PSA rise could be due to inflammation in the prostate postlaser surgery and not malignancy. The low positive predictive value may be an artefact of the group size. It also could be a reflection of biopsy technique. In other words, the patients with positive PCA3 test findings may well have a malignancy that has not been discovered on initial biopsy, and only with repeat/saturation biopsy will the malignancy come to light.
This will need further investigation and greater patient numbers to determine.
Conclusion
The exact role of PCA3 testing in the assessment of men who present with prostate disease is yet to be determined. The initial results in our study suggest that it will be a valuable test to help decide which patients with raised PSA results post-PVP need a biopsy of the prostate. Our initial results suggest that a PCA3 test with negative results is a good predictor of a biopsy with negative findings.
Footnotes
Disclosure Statement
No competing financial interests exists.