
Abstract
Background and Purpose:
To compare the oncologic results, functional outcomes, and complications of transperitoneal (TP) and extraperitoneal (EP) robotic radical prostatectomy.
Patients and Methods:
From June 2007 to April 2009, 105 patients underwent TP robotic radical prostatectomy, and 155 patients underwent EP robotic radical prostatectomy. Clinicopathological and perioperative data were compared between the two groups. Postoperative complications and functional outcomes including potency and incontinence were assessed.
Results:
Patient demographics were similar in the TP and EP groups. No significant differences in positive surgical margins were noted between the groups. The total operative time, number of lymph nodes removed, and estimated blood loss were also not significantly different. However, the robot console time was shorter for the EP group than for the TP group (89.1 vs. 107.8 minutes, p = 0.03). Postoperative pain scale scores were lower in the EP group than in the TP group (2.7 vs. 6.3, p < 0.001). The incidence of ileus and hernia were lower in the EP group; however, the incidence of lymphocele was higher in the EP group. Postoperative potency and continence rates were similar between the groups; however, the EP group had a faster recovery of continence compared with the TP group.
Conclusions:
The EP approach has similar oncological and perioperative results, less postoperative pain, less bowel-associated complication, and better functional outcomes than those of the TP approach. The EP approach may be an important alternative in robotic radical prostatectomy.
Introduction
The TP approach offers a larger working space and relatively easy port placement and docking, yet it is performed in a steep trendelenburg position to retract the bowel cephalad. 7 Although uncommon, bowel complications can cause significant morbidity from the TP operation. The concerns regarding the EP approach are the perceived small working space and the difficulty in gaining access to the pelvis. 8 However, the EP approach avoids exposure to the abdominal contents and offers access without requiring much trendelenburg positioning.
Since Gettman et al 9 presented the first clinical cases of EP robot-assisted radical prostatectomy, several studies have evaluated the oncological outcomes as well as the complications of both approaches. However, it remains difficult to draw any conclusions regarding which approach is superior. In particular, limited data exist for comparisons of functional outcomes between the two approaches. In this study, we evaluated and compared functional results, including potency and incontinence, and complications of both operative approaches.
Materials and Methods
Patient population
After the surgeon had performed more than 200 robotic prostatectomies using the TP approach to overcome the learning curve before June 2007, patients were entered into the study. Two hundred and sixty consecutive patients underwent robot-assisted laparoscopic radical prostatectomy performed by a single surgeon between June 2007 and April 2009. One hundred and five patients underwent surgery with the TP approach from June 2007 to June 2008, and the last 155 patients underwent surgery by EP approach from June 2008 to April 2009. Demographic data and patient histories were collected. Postoperative parameters including operation time, estimated blood loss, length of stay, robotic console time, positive surgical margins, postoperative pain, functional outcomes, and complications were analyzed.
Operative technique
All surgeries were performed by a single urologist. TP robotic radical prostatectomy was performed in the previously described manner. 10 In the EP robotic radical prostatectomy, the patient was placed with mild trendelenburg angulation. An infraumbilical incision was made through the anterior rectus fascia. With digital dissection, a space behind the posterior sheath of the fascia was developed for balloon dilation. The balloon was inflated to create an EP space. Insufflation of the space was achieved using CO2 gas with a pressure at 15 mm Hg. A 12 mm camera was placed through this trocar site using the Hassan technique. Two 8 mm daVinci® ports were placed 8 cm away from the umbilicus between the umbilicus and anterior superior iliac spine on the pararectal line (Fig. 1). Two additional ports (5 and 12 mm) were placed on the left side, for the assistant. A 5 mm port site was prepared on the supraumbilical level, also for the assistant. The following steps were similar in both approaches. The dorsal vein was not ligated, and the puboprostatic ligament was preserved. The endopelvic fascia was only minimally dissected. Preservation of the neurovascular bundles was routinely accomplished except in patients with palpable disease, higher than clinical stage T3 disease or a Gleason score greater than 7.
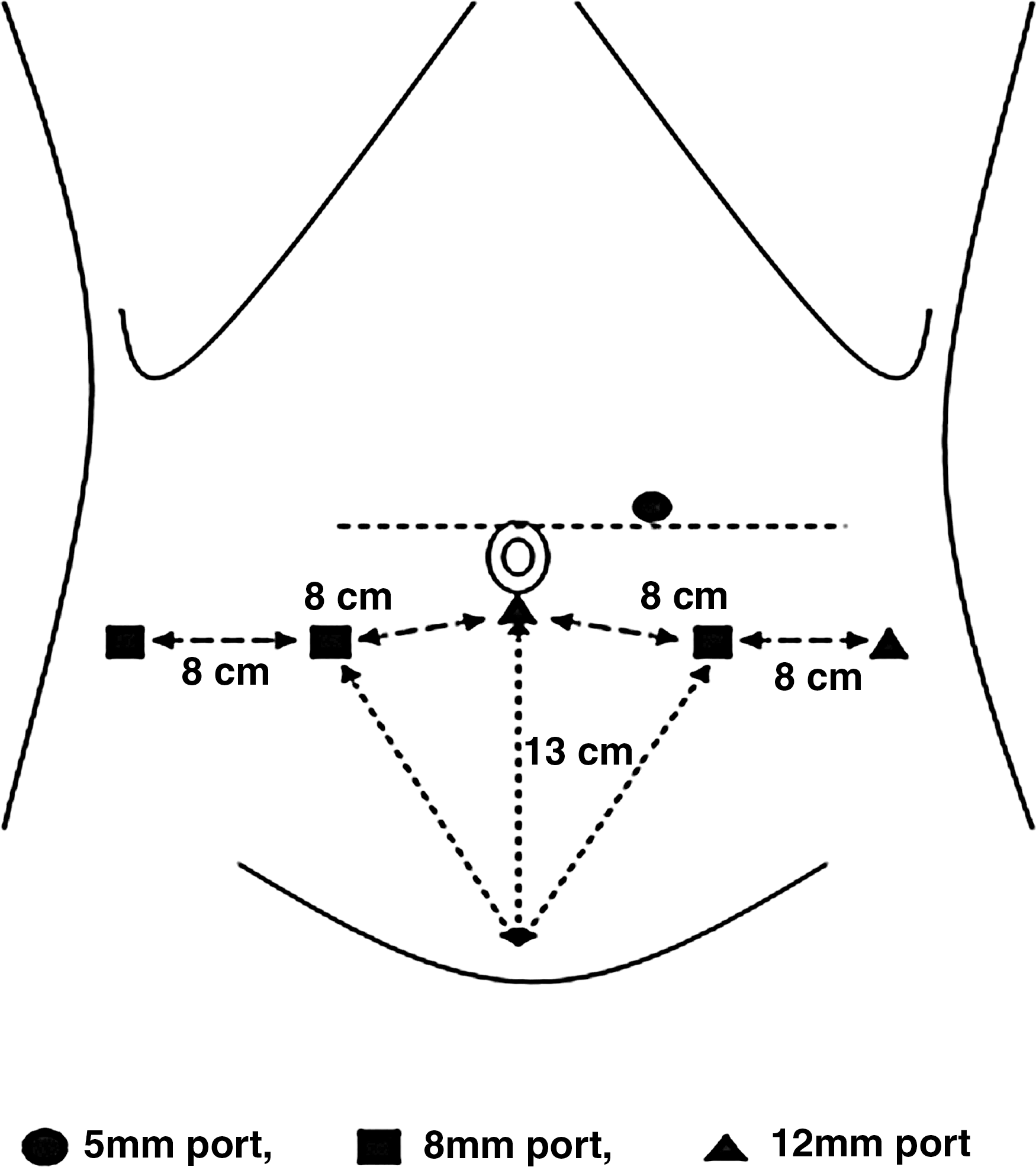
The positions of port placements in extraperitoneal robotic radical prostatectomy.
Functional outcomes and complication evaluations
Prostate specimens were placed in formalin before processing. Specimens were stained to evaluate surgical margins on histological slides. Positive margins were defined as extension of tumor to the stained surface of the resected specimen. Postoperative perceived pain intensity was assessed with a 10 cm visual analog scale, with values between 0 and 10, with 0 defined as “no pain sensation” and 10 defined as “the worst pain possible.”
All patients were provided with an intravenous patient controlled analgesia device with Fentanyl in postanesthesia care unit. Postoperatively, no additioinal intravenous or oral opioid analgesics were routinely ordered. Tylenol-ER 650 mg/T (acetaminophen) was prescribed only at patient request or the physician's discretion.
The opioid analgesic medication (Fentanyl) was converted to morphine sulfate equivalents for purpose of analysis. All of the patients completed a confidential, self-administered questionnaire regarding their sexual function and urinary incontinence. These questionnaires were the International Index of Erectile Function (IIEF)-5 questionnaire and incontinence questionnaire-urinary incontinence short form. 11,12 In the TP group, patients were asked to complete the questionnaire before and 1, 3, 6, and 12 months after surgery. Continence was evaluated immediately after Foley catheter removal, at 2 weeks, and then monthly. For the EP group, the last follow-up was also at 12 months. Unless contraindicated, all patients who were potent preoperatively were started on phosphodiesterase inhibitors for a month after catheter removal. Potency was defined as IIEF-5 score of 22 or greater. Continence was defined as using no pads.
Statistical analysis
The Student's t-test was used to compare continuous variables, and Fisher's exact test or the Chi-square test was used to compare categorical variables. Statistical differences were determined at a p-value of <0.05. The test was carried out with SPSS, version 12 (Chicago, IL).
Results
Patient and tumor characteristics are listed in Table 1. No statistically significant differences were found in mean patient age, serum prostate specific antigen level, prostate volume, clinical stage, pathological stage, or Gleason score. The oncological outcomes including positive surgical margins, number of removed lymph nodes, and tumor volume were also not different between the two groups.
Data are presented as number (%) or mean ± standard deviation.
TP = transperitoneal; EP = extraperitoneal.
Table 2 shows that mean operation time, blood loss, time until resumption of normal diet, length of hospital stay, and duration of bladder catheterization were not significantly different (p > 0.05). However, robot console time was significantly shorter in the EP group than in the TP group (89.1 vs. 107.8 minutes, p = 0.03). Although there were no significant differences between the two groups in quantity of opioids intraoperatively and postoperatively, the pain score using the visual analog scale on postoperative days 1 and 2 were lower in the EP group compared with the TP group (2.7 vs. 6.3 and 2.1 vs. 4.8, respectively, p < 0.001).
Data are presented as number (%) or mean ± standard deviation.
POD = postoperative day.
The complication rate of the TP group was higher than that of the EP group. The incidences of postoperative ileus and hernia were lower in the EP group. Lymphoceles were higher in the EP group (6.6 vs. 3.8%).
A functional evaluation including potency and continence was performed. The completion rates (also known as response rate) of the questionnaires were 71.2% (185/260) for the IIEF and 90.0% (234/240) for the incontinence questionnaire, respectively. For patients with preserved bilateral neurovascular bundles, the potency rates were 51.8% in the TP group and 54.8% in the EP group at 12 months after surgery (Table 3). Overall potency rates were similar between the two groups. The number of patients reporting continence increased from 12.6%, 42.1%, 52.1%, to 90.4% according to immediate, 2-week, 1-month, and 3-month follow-ups in the TP group and 35.7%, 55.8%, 61.2%, and 92.1% in the EP group, respectively (Table 4). The continence rates at 6 and 12 months were no different between the EP and TP groups (94.6 vs. 96.7% at 6 months, 96.6 vs. 98.6% at 12 months). However, the continence rates immediately after surgery, at 2 weeks, and at 1 month were higher in the EP than in the TP group. Thus, postoperative continence rates were similar in the groups, but the EP group showed a faster recovery of continence than did the TP group.
Data are presented as percentage (%).
Data are presented as percentage (%).
Discussion
Since robot-assisted radical prostatectomy was introduced in 2001, it has become an important treatment choice for localized prostate cancer. 13 Although the TP approach in robotic radical prostatectomy remains popular at present, the EP approach has been introduced, because this approach may offer certain advantages in terms of reduced intraperitoneal complications and possibly slightly faster return to normal diet.
Most previous studies comparing the TP and EP approaches have demonstrated little or no difference in complications and pathological outcomes. 14,15 Ruiz et al 16 compared laparoscopic radical prostatectomy outcomes in 165 patients with TP approach and 165 subsequent patients with EP approach and found no difference in convalescence, positive margin rates, or complications. In robot-assisted radical prostatectomy, Atug et al 14 found that complications and positive surgical margin rates were similar in both groups. Other authors have reported similar early oncological outcomes and postoperative complications regardless of the approach. 7,8
In the current study, after the surgeon had performed more than 200 robotic prostatectomies using the TP approach to overcome learning curve, patients were entered into the study. Therefore, before initiation of the EP approach, the surgeon had significantly more experience with the TP approach, having conducted 305 cases. In the EP approach, more preparation time was required to establish the pneumoperitoneum and to create the space of Retzius, which is not necessary in the TP technique. Still, there was no significant difference in the total operation times, because the EP approach required less console time.
Our study demonstrated similar oncological outcomes irrespective of the approach. Although prostate dissection techniques have been improved as surgeons gain increasing experience with robotic surgery, classic high anterior release and curtain dissection methods were used in the EP approach and did not have an impact on positive surgical margins. The space up to the bifurcation of the iliac vessels, which is required to perform a complete bilateral pelvic lymphadenectomy, can be slightly more challenging to access during the EP approach because of the limited working space. 14 However, due to increased surgical proficiency gained with the earlier TP cases, the mean number of lymph nodes removed showed no difference between the two groups. Concerning the surgical complications, most studies have reported that complications were nearly the same for the two methods. In our study, estimated blood loss, length of hospital stay, and time until resumption of normal diet were not different. Although the differences were not statistically significant, the majority of the complications resulted from the TP approach with the exception of lymphoceles. There were eight cases of hernia, seven cases of ileus, and one case of rectal injury in patients with TP. Even if lymphocele formation is not very high, its eventual formation seems to be a drawback of the EP procedure. No herniation from the trocar sites in our EP locations was noted. In addition, the risk of ileus was decreased by avoiding peritoneal entry in the EP approach.
In this study, pain intensity was measured with a 10 cm visual analog scale. The pain intensity of the EP approach was lower than that of the TP approach. This may be because the EP approach avoids the peritoneal cavity, thus preventing the potential risk of pain resulting from pneumoperitoneum or peritoneal irritation caused by urine leakage into the peritoneal cavity.
To date, very few attempts have been made at comparing the functional outcomes of the TP versus EP approaches in robot surgery, though similar functional results in laparoscopic radical prostatectomy have been investigated. 17 –19 Since both approaches well preserve the neurovascular bundle, it is reasonable that no differences were noted in our potency data. However, the return of sexual function after unilateral and bilateral nerve sparing radical prostatectomy may take from 6 to 48 months. 20 Thus, our short-term potency return rates should be carefully considered. Significant differences in the return of continence were present at immediate, 2-week, and 1-month follow-ups after surgery within the two groups. The EP group had faster continence recovery rates than the TP group in the early days after surgery.
Although the precise mechanism remains unclear, faster continence recovery might be the result of our modified technique and not strictly the EP approach itself. With advancing skills, we performed robotic radical prostatectomy with minimal ligation; very little electrical cauterization and good preservation of the endopelvic fascia, dorsal vein, puboprostatic ligaments, external urethal sphincter, and pelvic floor muscles; high anterior release; and curtain dissection. Consequently, improvements in continence rate may be the result of efficient surgery and not necessarily of the approach used. It remains difficult to draw any conclusions regarding whether the EP approach offers real advantages regarding the recovery of continence.
Our study focused on a single surgeon to eliminate the bias of different techniques and skill levels that come into question when multiple surgeons are involved. It should be also noted that, to our knowledge, our study is the largest comparison study of the two approaches in robotic surgery.
There are some limitations to our study. First, our results were drawn from a nonrandomized, comparative study with patients who underwent TP access surgery early in the series compared with more recent patients having EP access surgery. Therefore, it is not possible to say whether a particular approach to radical prostatectomy delivers better outcomes without the performance of prospective randomized trials. Second, potency rates appear to be similar between the two approaches, though the EP group showed faster continence recovery rates. Interpretation of functional outcomes was limited by short follow-up. Third, the surgical technique, particularly with regard to prostate dissection, has been modified over time. Thus, it was difficult to evaluate differences in the functional outcomes of each approach; we, therefore, cannot comment meaningfully on functional outcomes. Despite the shortcomings of the available evidence, our results suggest that the EP approach can be effectively and safely performed to achieve cancer removal without a significant increase in complications.
Conclusion
The TP approach has been the standard prostatectomy technique, whereas the EP approach has similar oncological and perioperative results, less postoperative pain, and better functional outcomes. The EP approach avoids potential bowel injury and may reduce morbidity from urinary extravasation. Considering our results, the EP approach may be an important alternative in robotic radical prostatectomy.
Footnotes
Acknowledgments
This study was supported by the grant of the Korean Urological Oncology Society sponsored by Korea Ipsen and the grant of the Korea Healthcare Technology R&D Project, Ministry for Health, Welfare & Family Affairs, Republic of Korea. (A084120)
Disclosure Statement
No competing financial interests exist.