
Abstract
Background and Purpose:
Histotripsy is a pulsed focused ultrasound technology in which initiation and control of acoustic cavitation allow for precise mechanical fractionation of tissues. The present study examines the feasibility of using histotripsy for erosion of urinary calculi.
Materials and Methods:
Histotripsy treatment was delivered from a 750-kHz transducer in the form of 5-cycle acoustic pulses at a 1-kHz pulse repetition frequency. Model stones were sonicated for 5 minutes at peak negative pressures (p-) of 10, 15, 19, 22, and 24-MPa. Resulting fragment sizes and comminution rates were assessed and compared with those achieved with a piezoelectric lithotripter (Wolf Piezolith 3000) operated at 2-Hz pulse repetition frequency and power level 17 (p- = 14-MPa).
Results:
Histotripsy eroded the surface of stones producing fine (<100 μm) particulate debris in contrast to the progressive and incomplete subdivision of stones achieved with piezoelectric lithotripsy. The histotripsy erosion rate increased with increasing peak negative pressure from 10 to 19 MPa and then saturated, yielding an average rate of 87.9 ± 12.8 mg/min at maximum treatment intensity. Piezoelectric lithotripsy achieved an average treatment rate of 110.7 ± 27.4 mg/min.
Conclusions:
Histotripsy comminution of urinary calculi is a surface erosion phenomenon that is mechanistically distinct from conventional shockwave lithotripsy (SWL), producing only fine debris as opposed to coarse fragments. These characteristics suggest that histotripsy offers a potential adjunct to traditional SWL procedures, and synergistic interplay of the two modalities may lead to possible increases in both rate and degree of stone fragmentation.
Introduction
Histotripsy is a novel technique for noninvasive, mechanical fractionation of tissues. Using pulsed focused ultrasound to control cavitation activity, histotripsy has been demonstrated to mechanically homogenize tissues within the focus to acellular debris after several minutes of treatment. 6 –8 Initiation and maintenance of a cavitational bubble cloud can be directed via proper ultrasound pulse sequences, 9 which typically include very short (<50 cycles), high peak-negative pressure (>6-MPa), nonlinear pulses delivered at low duty cycles (0.1%–5%). With the recent success in applying histotripsy for controlled fractionation of soft tissues, we sought to assess its usefulness for erosion of Ultracal-30 model urinary calculi.
Materials and Methods
Preparation of model urinary stones
Artificial stones were cast from Ultracal-30 gypsum cement (U.S. Gypsum, Chicago, IL), which has been implemented in several in-vitro lithotripsy assessments. 10 –12 The cement slurry was prepared per the protocol of McAteer and associates, 10 and 0.8-mL aliquots of the solution were subsequently distributed into the cylindrical wells of an aluminum suppository mold (Gallipot, Inc, St. Paul, MN). Each well was 10 mm in diameter, which resulted in cylindrical stones of 7.76 ±0.23 mm (mean ± standard deviation) height and 900.0 ±4.3 mg weight.
Ultrasound generation and treatment
The selection of histotripsy treatment parameters was guided based on a preliminary exploration of the histotripsy parameter space. Stones were sonicated using a piezocomposite spherically focused 750-kHz transducer (Imasonic, S.A., Voray sur l'Ognon, France) measuring 15 cm in diameter and having a 12 cm focal length. The focal volume is cigar-shaped, extending 16 mm in the axial direction and 2.3 mm in the lateral direction. All stones were treated using 5-cycle pulses delivered at a pulse repetition frequency of 1-kHz. To investigate the efficiency of histotripsy treatment, ultrasound was applied to stones at different peak negative pressures of 10, 15, 19, 22, and 24-MPa.
Lithotripsy was performed using a Wolf Piezolith 3000 piezoelectric lithotripter (Richard Wolf Medical Instruments Corporation, Vernon Hills, IL). Shockwaves were delivered at a rate of 2 Hz at power level 17, corresponding to peak negative/peak positive pressures of 14-MPa/76-MPa.
For each modality, Ultracal-30 stones were treated in a 21°C water tank with an oxygen level 80% of saturation to mimic that of urine. 13 Stones that were treated with lithotripsy were held in a thin finger cot, while those exposed to histotripsy were placed in a wire-mesh basket to prevent prefocal cavitation. Eight stones were treated with each parameter set, and all were sonicated for 5 minutes.
Debris size and treatment rate measurements
The distribution of stone fragment sizes resulting from both treatments was evaluated by sequentially sieving fragmented stone debris through 2 mm, 1 mm, and 100 μm filters. The change in dry weight of each filter was measured to assess the fraction of stone mass corresponding to a given pore size.
The treatment rate for each modality was defined as the mass of stone fragments less than 2 mm divided by the treatment time (5 minutes). The 2 mm threshold was chosen as the criterion for fragments to be considered “treated” based on clinical observations that those less than 2 mm can be discharged spontaneously after treatment. 14
Results
Stone fragment size distribution
The cavitational bubble cloud produced by histotripsy eroded away the face of the stone adjacent to the therapy transducer, producing a plume of fine particulate debris throughout the treatment. No subdivision of stones into coarse fragments occurred as a result of histotripsy, and following the 5-minute sonication period, a single stone piece of reduced size remained. At maximum treatment intensity, this solitary residual piece had a mass of 509.0 ± 98.4 mg, representing 53.4% ± 6.8% of the original stone. Stone fragments that were generated by histotripsy were smaller than 100 μm in the largest dimension, and as such were not measurable by the filters used in this study. Microscopic imaging of histotripsy debris provided visualization of stone fragments <100 μm (Fig. 1a).
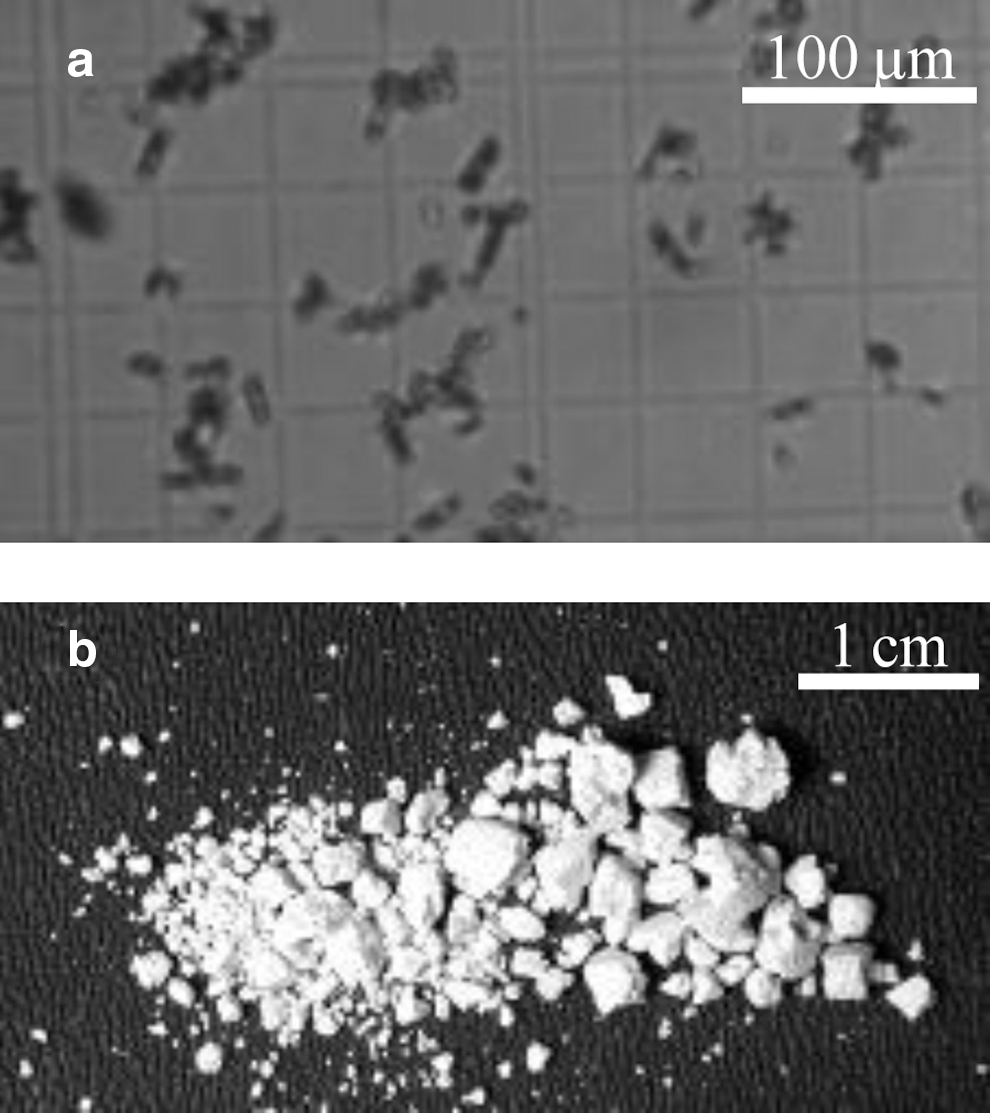
Ultracal-30 stone fragments following treatment with
The Piezolith 3000 progressively fractionated stones throughout the 5-minute treatment, and resulting fragments were of varying size (Fig. 1b). On the 2 mm, 1 mm, and 100 μm filters, 32% ± 16%, 30% ± 10%, and 26% ± 11% were captured, respectively.
Stone treatment rate
The rate of histotripsy stone erosion is plotted as a function of peak negative pressure (p-) in Figure 2. Control group stones were handled in the same way as the stones that received histotripsy treatment, but were not exposed to ultrasound. No visible damage to control stones was observed, although they did display a mass loss and calculated erosion rate of 1.68 ± 0.68 mg/min (not plotted) assuming a 5-minute treatment. This mass loss is likely the result of simply handling the stone. All stones receiving ultrasound exposure displayed a statistically significant increase in erosion rate relative to control (P < 0.001), and the erosion rate was found to increase with increasing p- from 10 to 19-MPa (P < 0.003). Stones that were treated at a p- of 10-MPa had an erosion rate of 21.6 ± 1.5 mg/min, those at 15-MPa, a rate of 65.1 ± 8.6 mg/min, and those at 19-MPa, a rate of 85.1 ± 12.0 mg/min. Treatment at higher pressure levels did not yield a statistically significant difference in rate relative to that observed at 19-MPa (P > 0.7). Stones treated at 22-MPa displayed an erosion rate of 86.0 ± 10.3 mg/min, while those treated at 24-MPa had a rate of 87.9 ± 12.8 mg/min.
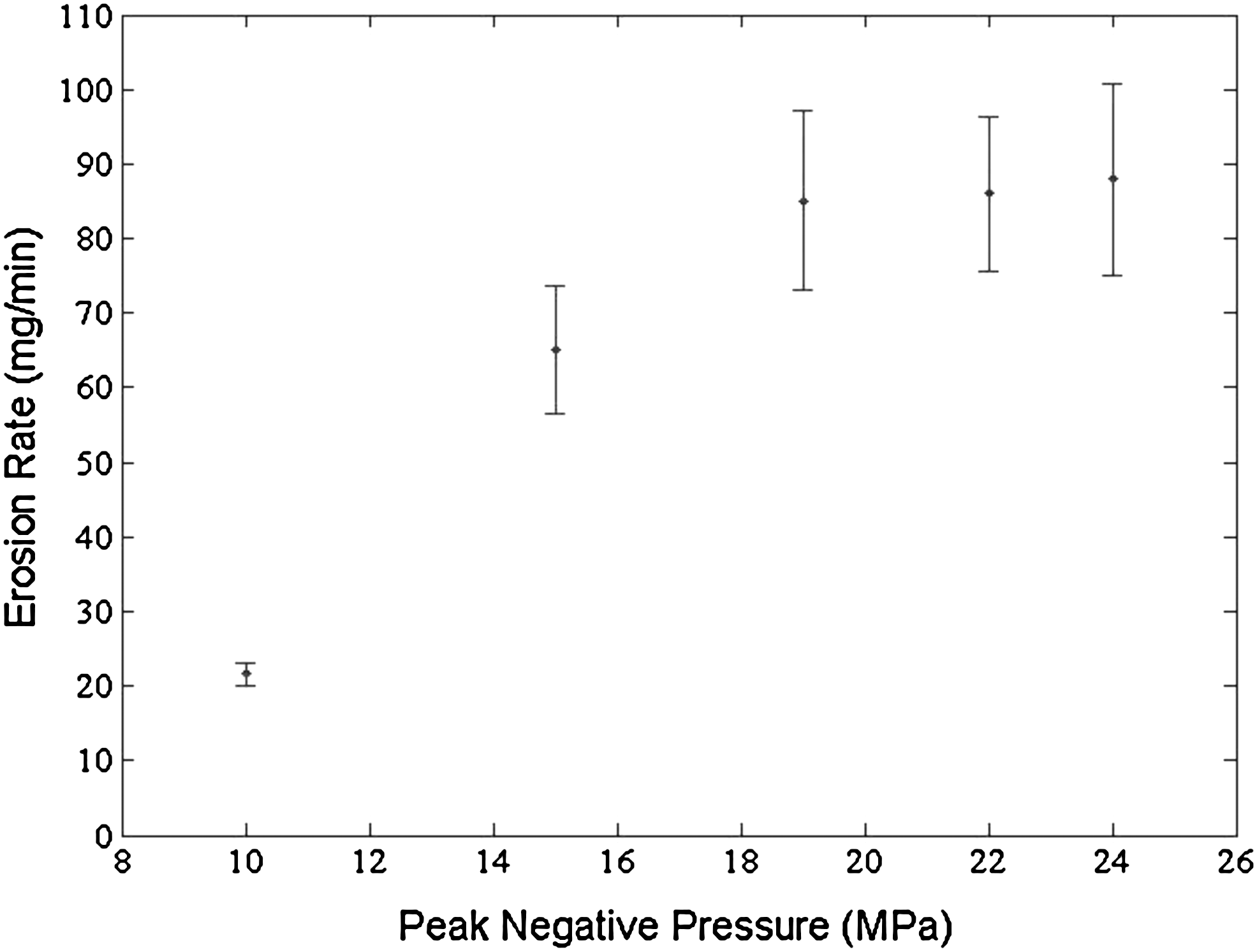
The histotripsy stone erosion rate plotted as a function of peak negative pressure (p-).
Progressive stone fractionation with the Piezolith 3000 resulted in a stone treatment rate of 110.7 ± 27.4 mg/min.
Discussion
Histotripsy effectively comminutes Ultracal-30 model stones, eroding the surface to sub 100 μm debris via a cloud of cavitating microbubbles. Similar results were observed by Yoshizawa and colleagues, 15 who demonstrated that application of high intensity focused ultrasound lithotripsy to natural stones produces small stone fragments (<1 mm) as a result of localized cavitation on the stone surface. It is important to distinguish the cavitation erosion in histotripsy from the comminution characteristics of SWL. In SWL, a primary calculus is comminuted in a progressive manner, involving initial stone breakage into several large pieces, followed by subsequent fractionation into smaller and smaller fragments as more shockwaves are applied. It has been documented that SWL is highly effective during the initial subdivision phase of comminution, rapidly producing several large pieces (within the first 200 shockwaves). 4 Subsequent fragmentation, however, is much less efficient, generally necessitating hundreds to thousands of additional shockwaves to achieve debris less than 2 mm. 4 This fragment reduction phase thus accounts for the majority of the procedure time.
In addition, because stone comminution with histotripsy is a surface erosion phenomenon, an increase in exposed stone surface area yields an increase in erosion rate. This characteristic—coupled with decreased efficacy of SWL for small fragments—suggests that histotripsy offers a potential adjunct to conventional SWL. Using the strengths of each treatment modality, lithotripsy could first be applied to fractionate a stone into multiple fragments (and thus increase the exposed surface area), and then histotripsy could be used to erode those fragments into tiny particulate debris. Such synergistic interplay between the two modalities could potentially increase both rate and degree of stone comminution.
Although this study demonstrated the feasibility of using histotripsy to manage renal calculi, several experimental limitations existed. There is a disconnect between treating model stones in a water tank and the physiologic setting, and despite the fact that Ultracal-30 is a commonly accepted stone model, it only mimics properties of natural stones to a certain extent. With respect to treatment rate, the progressive stone comminution in lithotripsy implies that clinically passable fragments (<2 mm) are not produced at a constant rate throughout the treatment. Thus, it is somewhat difficult to define a “treatment rate” for lithotripsy, and the rate presented here is solely for the purpose of comparison with histotripsy.
Finally, a technical challenge in moving forward with in-vivo histotripsy stone treatment is targeting. Although previous work has demonstrated that the collecting system displays a marked resistance to histotripsy damage, 16 the ability to track stone movement is essential for minimizing cavitational damage to surrounding tissues. We anticipate that targeting may eventually become a strong suit of histotripsy stone erosion; both the calculus and the histotripsy bubble cloud appear as hyperechoic regions on B-mode ultrasound imaging, presenting the opportunity for focal tracking algorithms. With this in mind, our continued work will include further investigation of histotripsy-induced stone erosion in more physiologically relevant settings, the exploration of potential focal respiratory tracking strategies, and further optimization of the histotripsy parameter space.
Conclusion
Histotripsy comminution of model urinary calculi is a surface erosion phenomenon mechanistically distinct from conventional SWL, producing only fine debris as opposed to coarse fragments. Whereas lithotripsy uses shockwaves to progressively fractionate a stone, histotripsy uses appropriately designed ultrasound pulse sequences to control cavitation activity on the stone surface. The characteristics of comminution via cavitation erosion in histotripsy are complementary to conventional SWL, and as such have the potential to augment traditional SWL protocols.
Footnotes
Acknowledgments
The authors would like to thank Harry West and the Livonia Center for Specialty Care for their help in performing experiments with the Piezolith 3000.
Disclosure Statement
Timothy L. Hall, Zhen Xu, Charles A. Cain, and William W. Roberts are inventors of intellectual property licensed to HistoSonics, Inc, hold stock in HistoSonics, Inc, and consult for HistoSonics, Inc. Adam D. Maxwell consults for HistoSonics, Inc.